Rationale of the Week | KR is on Metformin & 4 Weeks Pregnant. Best action?
For last week’s practice question, we quizzed participants on ADA recommendations for metformin while pregnant. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: KR has polycystic ovary syndrome and takes metformin 850mg twice daily. KR just discovered they are 4 weeks pregnant. Fasting glucose is 103 mg/dl.
According to ADA Guidelines, if prediabetes diagnosis is confirmed, what is the next step?
Answer Choices:
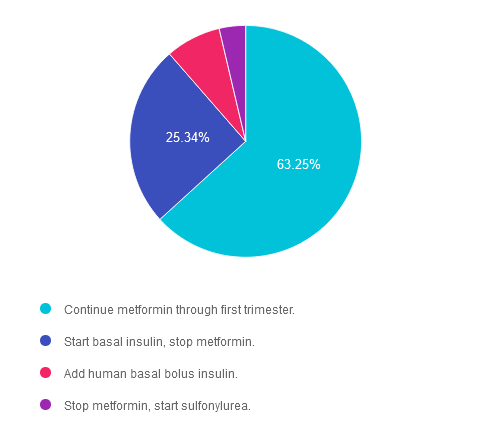
- Continue metformin through first trimester.
- Start basal insulin, stop metformin.
- Add human basal bolus insulin.
- Stop metformin, start sulfonylurea.
Getting to the Best Answer
Answer 1 is correct. 63.25% chose this answer. “Continue metformin through first trimester.” YES, this is the best answer. According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Standard 15 goes on to say, “Insulin is the preferred medication for treating hyperglycemia in GDM. Metformin and glyburide, individually or in combination, should not be used as first-line agents, as both cross the placenta to the fetus. Other oral and noninsulin injectable glucose-lowering medications lack long-term safety data.” Given that KR has a fasting glucose in the prediabetes range, basal insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Answer 2 is incorrect. 25.34% of you chose this very tempting answer. “Start basal insulin, stop metformin.” However, according to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Given that KR has a fasting glucose in the prediabetes range, basal insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Answer 3 is incorrect. About 7.74% of respondents chose this. “Add human basal bolus insulin.” According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Given that KR has a fasting glucose in the prediabetes range, basal bolus insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Finally, Answer 4 is incorrect. 3.68% chose this answer. “Stop metformin, start sulfonylurea.” According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Standard 15 goes on to say, “Insulin is the preferred medication for treating hyperglycemia in GDM. Metformin and glyburide, individually or in combination, should not be used as first-line agents, as both cross the placenta to the fetus. Other oral and noninsulin injectable glucose-lowering medications lack long-term safety data.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join us live on June 11th at 11:30 am PST for our
Pregnancy & Diabetes
Level 2 Standards of Care Intensive
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, & understanding. This course reviews those special needs while focusing on Gestational Diabetes & Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, & prevention of complications during pregnancy. This is a helpful review for Certification Exams & those who want more information on people who are pregnant & live with diabetes.
Objectives:
- List three issues that affect pregnancy with diabetes.
- Describe the unique attributes of pre-existing diabetes in pregnancy & gestational diabetes.
- State the diagnostic criteria & management goals for gestational diabetes.
- Potential short-term & long-term complications of fetal exposure to hypoglycemia.
- Prevention measures to keep mother & baby healthy.
Learning Outcome:
Participants will gain knowledge of special considerations, individualized goals, and standards for people experiencing diabetes during pregnancy to improve outcomes.
Target Audience:
This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs/RDNs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions. The practice areas for RDs/RDNs for CDR reporting are healthcare, preventative care, wellness, and, lifestyle along with, education and research.
CDR Performance Indicators:
- 9.6.7
- 9.6.8
- 10.3.1
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working diabetes specialist and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Are statins indicated for Peds with Diabetes?
For last week’s practice question, we quizzed participants on when to start statin therapy for pediatrics with diabetes. 50% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Based on the ADA Standards, in addition to dietary intervention, lifestyle and glucose management, when is it indicated to consider starting statin therapy for pediatrics with diabetes?
Answer Choices:
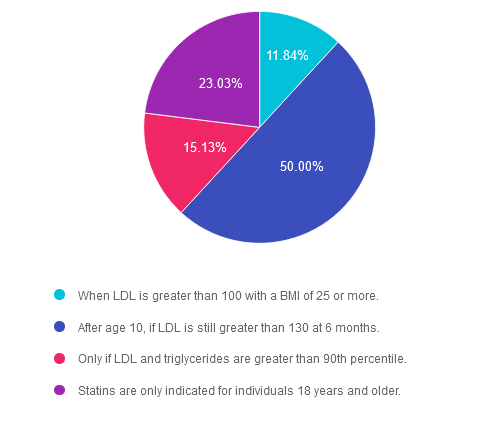
- When LDL is greater than 100 with a BMI of 25 or more.
- After age 10, if LDL is still greater than 130 at 6 months.
- Only if LDL and triglycerides are greater than 90thpercentile.
- Statins are only indicated for individuals 18 years and older.
Getting to the Best Answer
Answer 1 is incorrect. 11.84% chose this answer. “When LDL is greater than 100 with a BMI of 25 or more.” This is a tempting answer. However, according to ADA Standards, if after 6 months of intensive lifestyle intervention, the LDL is still greater than 130mg/dL and the child is 10 years or older, statin therapy is indicated to prevent cardiovascular complications.
Answer 2 is correct. 50% of you chose this answer. “After the age of 10 if LDL is 130 or greater.” Great job, this is the BEST answer. According to ADA Standards, if after 6 months of intensive lifestyle intervention, the LDL is still greater than 130mg/dL and the child is 10 years or older, statin therapy is indicated to prevent cardiovascular complications.
Answer 3 is incorrect. About 15.13% of respondents chose this. “Only if LDL and triglycerides are greater than 90thpercentile.” According to ADA Standards, if after 6 months of intensive lifestyle intervention, the LDL is still greater than 130mg/dL and the child is 10 years or older, statin therapy is indicated to prevent cardiovascular complications.
Finally, Answer 4 is incorrect. 23.03% chose this answer. “Statins are only indicated for individuals 18 years and older.” According to ADA Standards, if after 6 months of intensive lifestyle intervention, the LDL is still greater than 130mg/dL and the child is 10 years or older, statin therapy is indicated to prevent cardiovascular complications.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join us live on May 30th at 11:30 PST for our
From Tots to Teens
Level 2 Standards of Care Intensive
This course includes updated goals & guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes & their families. We discuss the clinical presentation of diabetes, goals of care, & normal growth & development through the early years through adolescence. Strategies to prevent acute & long-term complications are included with an emphasis on positive coping for families & children with diabetes.
Objectives:
- Discuss the goals of care for Type 1 and Type 2 Kids with Diabetes.
- State Strategies to prevent acute and chronic complications.
- Discuss the importance of positive psychosocial adjustment & resources.
Learning Outcome:
Attendees will have comprehensive knowledge of special considerations, individualized goals and standards for children with diabetes to include in their practice.
Target Audience:
This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs/RDNs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions. The practice areas for RDs/RDNs for CDR reporting are healthcare, preventative care, wellness, and, lifestyle along with, education and research.
CDR Performance Indicators:
- 9.6.7
- 9.6.8
- 10.3.1
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working diabetes specialist and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Best treatment for Hypoglycemia with Gastroparesis
For last week’s practice question, we quizzed participants on how to treat hypoglycemia while dealing with gastroparesis. 73% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 diabetes and was recently diagnosed with gastroparesis. JR is a runner and has not been able to exercise recently due to nausea, vomiting, bloating, and intestinal pain. They experience hypoglycemia about 3 times a week.
Based on this information, what is the best treatment for hypoglycemia?
Answer Choices:
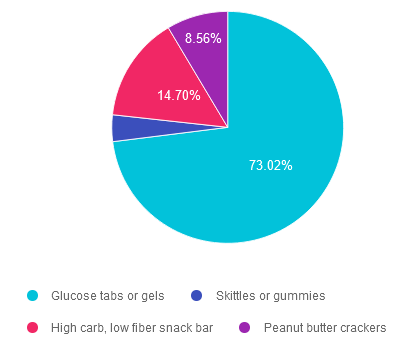
- Glucose tabs or gels.
- Skittles or gummies.
- High carb, low fiber snack bar.
- Peanut butter crackers.
Getting to the Best Answer
Answer 1 is correct. 73.02% chose this answer. “Glucose tabs or gels.” Great job! Since JR has gastroparesis with slowed gastric emptying and delayed absorption of nutrients, we need to provide a fast acting carb that can instantly raise blood sugar. Fast absorption of sugar from glucose tabs and gels begins in the mouth, to quickly raise blood sugar levels.
Answer 2 is incorrect. 3.72% of you chose this answer. “Skittles or gummies.” Since JR has gastroparesis with slowed gastric emptying and delayed absorption of nutrients, we need to provide a fast acting carb that can instantly raise blood sugar. Gummies and skittles are more challenging to chew and need to be broken down in the stomach, which would delay the blood sugar from increasing to a safe level. Another consideration is that the ability to chew can be impaired when someone is experiencing significant hypoglycemia. Glucose tabs and gel, are quickly absorbed and require minimal chewing and are the best choice.
Answer 3 is incorrect. About 14.70% of respondents chose this. “High carb, low fiber snack bar.” Since JR has gastroparesis with slowed gastric emptying and delayed absorption of nutrients, we need to provide a fast acting carb that can instantly raise blood sugar. A snack bar, even though it is low fiber, is more challenging to chew and needs to be broken down in the stomach, which would delay the blood sugar from increasing to a safe level. Another consideration is that the ability to chew can be impaired when someone is experiencing significant hypoglycemia. Glucose tabs and gel, are quickly absorbed and require minimal chewing and are the best choice.
Finally, Answer 4 is incorrect. 8.56% chose this answer. “Peanut butter crackers.” Since JR has gastroparesis with slowed gastric emptying and delayed absorption of nutrients, we need to provide a fast acting carb that can instantly raise blood sugar. Peanut butter crackers are more challenging to chew and need to be broken down in the stomach, which would delay the blood sugar from increasing to a safe level. Another consideration is that peanut butter is a protein and fat combination food that would delay the absorption of the carbs from the crackers. Glucose tabs and gel, are quickly absorbed and would be the best choice!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity
Unlock insights for managing diabetes distress with the experts!
Join us live on June 17th & 24th, 2024 for our
ReVive 5 Diabetes Training Program:

The 2024 ADA Standards of Care now recommends annual screening for diabetes distress. If you are wondering how to screen for distress and tailor education based on the results, we encourage you to join this unique training program.
This two-session training provides the essential steps to address diabetes distress combined with an innovative approach to helping people make sense of their glucose data.
The first session is team-taught by experts in the field of diabetes distress and effective communication approaches. Dr. Larry Fisher kicks off the program by describing the difference between depression and distress and interpreting Diabetes Distress screening results. Dr. Susan Guzman uses a case study approach and step-by-step communication strategies to address responses from the Diabetes Distress screening tool. This session includes an abundance of evidence-based approaches that you can apply in your clinical setting.
Coach Beverly leads the second session. During this three-hour program, Beverly describes insulin dosing strategies, meter and sensor data interpretation, and common issues encountered by people using diabetes technology. Case studies include tools to help individuals discover what changes are needed to get glucose to target, coupled with the communication skills discussed in the first session. In conclusion, the team of instructors review a case study that pulls together all the ReVive 5 elements.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Can’t join live? That’s okay. Your registration guarantees you access to the recorded version of the series, along with podcasts and resources for one full year.
Accredited Training Program:
- 15+ CEs – Includes the 7-hour ReVive 5 Training Program, Certificate, and 5 FREE bonus courses to supplement content.
- A comprehensive set of assessment tools, educational materials, log sheets, and resources.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
- Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
- Susan Guzman, PhD
- Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Speakers Interviews – Learn more about the ReVive 5 Team
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Assessment of Hypoglycemia
For last week’s practice question, we quizzed participants on assessing risk factors for hypoglycemia. 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LM has had type 2 diabetes for over 30 years and takes 1000 mg metformin BID, 30 units of glargine at bedtime, 25 mg empagliflozin, as well as daily lisinopril and lovastatin. A1c was 7.2%, LDL: 56, and eGFR was 38 mL/min/1.73m2 last visit. CGM ambulatory glucose profile report indicates a time in range of 71%, time below range of 4%, and time above range of 25%. LM reports living on a fixed income, relying on social security, and an increase in recent financial stress. They are concerned they may not have enough money to purchase foods by the end of the month.
Select the best answer considering LM’s potential risk factors for hypoglycemia?
Answer Choices:
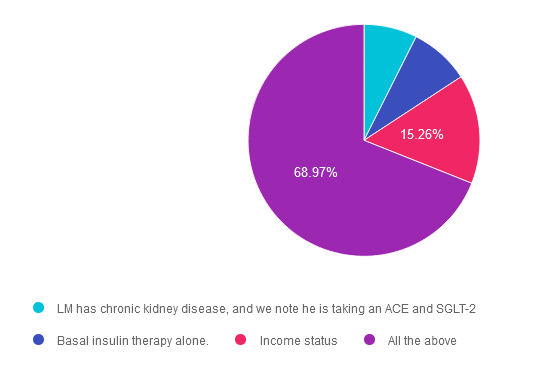
- LM has chronic kidney disease, and we note he is taking an ACE and SGLT-2
- Basal insulin therapy alone.
- Income status.
- All the above.
Getting to the Best Answer
Answer 1 is incorrect. 7.42% chose this answer. “LM has chronic kidney disease, and we note he is taking an ACE and SGLT-2.” Answer 1 is somewhat true but is not the best answer. We may consider this question incorrect due to the statement that LM is taking ACE and SGLT-2 medications, and we know these have a low risk of hypoglycemia. However, a diagnosis of CKD, especially along with basal insulin therapy, can be a factor that increases hypoglycemia risk. If LM’s GFR was below 15 with a diagnosis of end-stage renal disease, then we would consider this a major risk factor. Let’s keep reading for the best answer.
Answer 2 is incorrect. 8.36% of you chose this answer. “Basal insulin therapy alone.” Answer 2 is also true but is not the best answer. Hypoglycemia risk is highest in individuals treated with intensive insulin therapy followed by basal insulin and then sulfonylureas.1 Basal insulin therapy is a risk factor for hypoglycemia, and we may be tempted to select this answer alone. However, other considerations also impact LM’s risk for hypoglycemic events while on basal insulin therapy.
Answer 3 is incorrect. About 15.26% of respondents chose this. “Income status.” Answer 3 is also true but is not the best answer. Income status and food insecurity are considered risk factors for hypoglycemia and are associated with increased hospital admissions and ER visits. However, we must also consider this along with medication treatment. Food insecurity along with LM’s basal insulin therapy is a major risk factor for hypoglycemia.
Finally, Answer 4 is correct. 68.97% chose this answer. “All the above.” Answer D is the correct Answer. The 2024 Standards of Care recommends hypoglycemia assessment at every clinical visit. We can use validated tools to determine risk for hospital admission or an ER visit, but these do not consider every risk factor. It is important to consider not only clinical factors but also social, economic, and cultural factors. Risk stratification is for all individuals treated with insulin, sulfonylureas, or meglitinides. ° American Diabetes Association Professional Practice Committee; 6. Glycemic Goals and Hypoglycemia: Standards of Care in Diabetes—2024. Diabetes Care 1 January 2024; 47 (Supplement_1): S111–S125. https://doi.org/10.2337/dc24-S006
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to Learn more about recognizing and addressing Diabetes Distress?
Join us live on June 17th & June 24th, 2024 for our
ReViVE 5 Diabetes Training Program:
Unlocking Hidden Barriers to Diabetes Management

“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
The ReVive 5 program is built on sound research from the Embark Trial and will revolutionize your approach to diabetes self-management education.
We have reassembled the Embark training team and created a resource binder of fantastic tools that we are excited to share with you in our ReVive 5 Diabetes Training Program. You are invited to join us to learn a step-wise, proven approach to addressing hidden barriers to diabetes self-management and glucose management.
You don’t need to be mental health expert or diabetes technology wiz to join this training or to integrate these new strategies into your daily practice.
ReVive 5 uses an integrated, evidence-based approach that provides health care professionals with a realistic 5-step approach to addressing the whole person, starting with emotional distress and incorporating a unique, but integrated approach to problem-solving glucose management difficulties.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the CDCES or BC-ADM Certification Exams.
Can’t join live? That’s okay. Your registration guarantees you access to the recorded version of the series, along with podcasts and resources for one full year.
Accredited Training Program:
- 15+ CEs – Includes the 7-hour ReVive 5 Training Program, Certificate, and 5 FREE bonus courses to supplement content.
- A comprehensive set of assessment tools, educational materials, log sheets, and resources.
Join us to gain the confidence and learn the skills needed to support people with diabetes to move forward in their self-management and discover the expert within.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
- Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
- Susan Guzman, PhD
- Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Speakers Interviews – Learn more about the ReVive 5 Team
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | RD feels overwhelmed by all this sensor data. Best action?
For last week’s practice question, we quizzed participants on actions to help address stress during data monitoring. 87% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: RD is 82 years old, on basal insulin with bolus insulin at breakfast and dinner if need. RD just started using a sensor to track their daily blood sugars. After using the sensor for a few weeks, they share that they are feeling anxious and don’t know what to do with all this information. They even took extra bolus insulin yesterday to try and get blood sugars down. RD’s time in range is over 70%.
Which of the following is the most appropriate intervention?
Answer Choices:
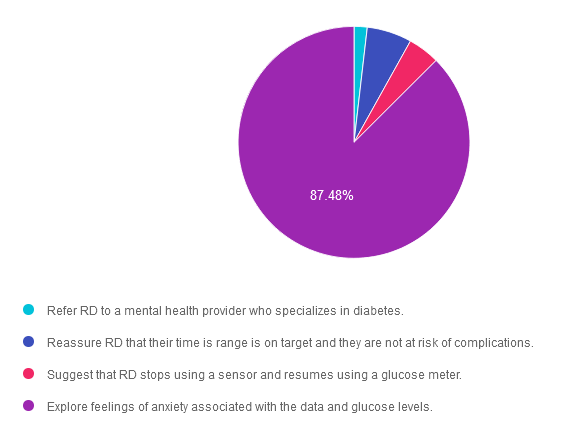
- Refer RD to a mental health provider who specializes in diabetes.
- Reassure RD that their time is range is on target and they are not at risk of complications.
- Suggest that RD stops using a sensor and resumes using a glucose meter.
- Explore feelings of anxiety associated with the data and glucose levels.
Getting to the Best Answer
Answer 1 is incorrect. 1.83% chose this answer. “Refer RD to a mental health provider who specializes in diabetes.” RD is having an understandable response to the abundance of info provided by their new CGM and is experiencing diabetes distress. Based on the information provided, their anxiety doesn’t warrant a referral to a mental health specialist.
Answer 2 is incorrect. 6.26% of you chose this answer. “Reassure RD that their time is range is on target and they are not at risk of complications.” Although it is important to reassure RD that they have a time in range greater than 70%, it is important to acknowledge their feelings and explore strategies to address to diabetes distress.
Answer 3 is incorrect. About 4.43% of respondents chose this. “Suggest that RD stops using a sensor and resumes using a glucose meter.” Since RD has only been using the sensor for a few weeks, we wouldn’t want to suggest giving it up just yet. In addition, we want to learn more about what RD is experiencing and the issues that are increasing their anxiety and help with problem solving.
Finally, Answer 4 is correct. 87.48% chose this answer. “Explore feelings of anxiety associated with the data and glucose levels.” YES. GREAT JOB! This is the best person-centered answer that encourages RD to share their feelings so we can help with problem solving and evaluate the best approach for this individual.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Unlock insights for managing diabetes distress with the experts!
Join us live on June 17 & 24, 2024 for our
ReVive 5 Diabetes Training Program:
The 2024 ADA Standards of Care now recommends annual screening for diabetes distress. If you are wondering how to screen for distress and tailor education based on the results, we encourage you to join this unique training program.
This two-session training provides the essential steps to address diabetes distress combined with an innovative approach to helping people make sense of their glucose data.
The first session is team-taught by experts in the field of diabetes distress and effective communication approaches. Dr. Larry Fisher kicks off the program by describing the difference between depression and distress and interpreting Diabetes Distress screening results. Dr. Susan Guzman uses a case study approach and step-by-step communication strategies to address responses from the Diabetes Distress screening tool. This session includes an abundance of evidence-based approaches that you can apply in your clinical setting.
Coach Beverly leads the second session. During this three-hour program, Beverly describes insulin dosing strategies, meter and sensor data interpretation, and common issues encountered by people using diabetes technology. Case studies include tools to help individuals discover what changes are needed to get glucose to target, coupled with the communication skills discussed in the first session. In conclusion, the team of instructors review a case study that pulls together all the ReVive 5 elements.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Can’t join live? That’s okay. Your registration guarantees you access to the recorded version of the series, along with podcasts and resources for one full year.
Accredited Training Program:
- 15+ CEs – Includes the 7-hour ReVive 5 Training Program, Certificate, and 5 FREE bonus courses to supplement content.
- A comprehensive set of assessment tools, educational materials, log sheets, and resources.
Join us to gain the confidence and learn the skills needed to support people with diabetes to move forward in their self-management and discover the expert within.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
- Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
- Susan Guzman, PhD
- Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Speakers Interviews – Learn more about the ReVive 5 Team
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Euglycemic DKA – What is Best Intervention?
For last week’s practice question, we quizzed participants on what is the best intervention for euglycemic DKA. 55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: KT is a 54-year-old, who presents to the emergency room with nausea and vomiting. KT weighs 58kg, has been feeling very tired and has diabetes and hypertension.
Meds include: losartan, metformin, and empagliflozin.
Labs: Na 140, K 4.0, Chloride 99, Bicarb 15, Glucose 189, Anion Gap 26, pH 7.1 and positive urine ketones
After infusing 2 liters of normal saline, what would be the best intervention for KT?
Answer Choices:
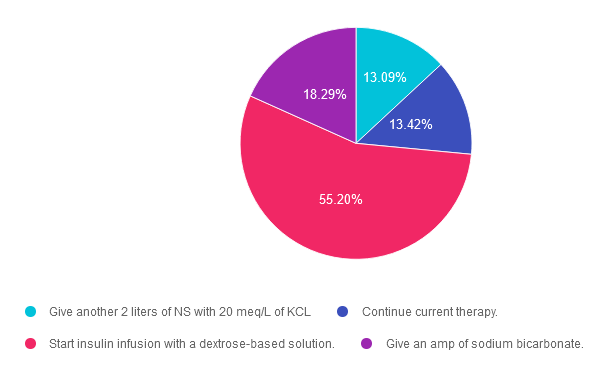
- Give another 2 liters of NS with 20 meq/L of KCL
- Continue current therapy.
- Start insulin infusion with a dextrose-based solution.
- Give an amp of sodium bicarbonate.
Getting to the Best Answer
Answer 1 is incorrect. 13% chose this answer. “Give another 2 liters of NS with 20 meq/L of KCL.” Since KT has already received 2 liters of normal saline for fluid resuscitation, the next step is to provide a solution with glucose, and possibly potassium depending on KT’s electrolyte levels. Even with euglycemic DKA, KT has depleted their glycogen stores and the cells are in desperate need of glucose for two reasons; to stop burning fat for fuel and to replete glycogen stores.
Answer 2 is incorrect. 13.42% of you chose this answer. “Continue current therapy.” While this answer is tempting, it does not provide a clear plan of action for KT. The only therapy this is currently being provided is an IV of normal saline. Even though KT’s blood glucose is less than 200mg/dL, in order to stop ketosis, we need to start IV insulin along with 5-10% dextrose to preserve blood glucose and replace glycogen stores.
Answer 3 is correct. About 55.20% of respondents chose this. “Start insulin infusion with a dextrose-based solution.” YES! This is the best answer. The next step is to provide an IV solution with 5-10% glucose, and possibly potassium depending on KT’s electrolyte levels. Even with euglycemic DKA, KT has depleted their glycogen stores and the cells are in desperate need of glucose for two reasons; to stop burning fat for fuel and to replete glycogen stores. In addition, in order to stop ketosis, we need to start IV insulin at a few units an hour!
Finally, Answer 4 is incorrect. 18.29% chose this answer. “Give an amp of sodium bicarbonate.” Since KT is in acidosis, this is a tempting answer. However, the acidosis will usually be corrected with administration of IV fluids and insulin. If not, and the pH is still below 7.0, bicarb administration may be considered.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Keynote Presentation on DKA & Euglycemic DKA at
16th Annual Conference
Expanding the Universe of Diabetes Care hosted by CA ADCES
May 3-4th at Universal City, CA

Beverly will be speaking on DKA and EDKA on Saturday – May 4, 2024 at 11:30 am
Below is Saturday’s schedule of topics and flyer for more information. We hope to see you there!
>>Register for the Conference
>>Flyer for Event
- Discover the secrets to a successful and sustainable Diabetes Education Program – Tony Song, MBA
- Exercise Success Part 3 & 4 – Jacqueline Thompson, MS, RD, CDCES, MES
- Dynamic Duo: Registered Dietitian & Pharmacist Co-Appointments in Diabetes Care – Christal Pham, PharmD, APh, CDCES, Melanie Barbee, MS, RDN, CDCES, DipACLM
- Advocacy Update: Breakdown the Barriers to Evidence-Based Diabetes Care – Teresa Martin MS RDN CDCES LD
- New criteria and treatment guidelines for DKA, Euglycemic DKA, and HHS – Beverly Thomassian, RN, MPH, CDCES, BC-ADM
- Exercise Success Part 4 – Jacqueline Thompson, MS, RD, CDCES, MES
- Diabetes Technology: Understanding the Differences in the Latest CGMs and Pumps – David Ahn, MD
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | ADA Standards for Gestational Diabetes
For last week’s practice question, we quizzed participants on ADA Standards for gestational diabetes. [%] of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LS has type 1 diabetes and is here for the first visit after confirmation of pregnancy. LS has been using non-adjunctive continuous glucose monitoring (CGM) along with insulin pump therapy to manage diabetes. Previous visits have focused on preconception counseling and last A1c was 6.4%.
According to the 2024 ADA Standards of Care, what do we recommend regarding glucose monitoring during pregnancy?
Answer Choices:
- Recommend continued CGM use with the addition of post-prandial glucose monitoring.
- LS can continue use of non-adjunctive CGM device approved for use during pregnancy.
- Recommend continued CGM with the addition of scheduled blood glucose monitoring.
- Recommend LS move to blood glucose monitoring and check fasting, pre-prandial and post-prandial glucose values.
Getting to the Best Answer
Answer 1 is incorrect. [%] chose this answer. “Recommend continued CGM use with the addition of post-prandial glucose monitoring.” Choice A is not the best answer. The 2024 ADA Standards of Care do recommend CGM use for individuals with type 1 diabetes during pregnancy but simply monitoring post-prandial glucose is insufficient. Keep reading below.
Answer 2 is incorrect. [%] of you chose this answer. “LS can continue use of non-adjunctive CGM device approved for use during pregnancy.” Choice B is not correct. We can continue use of CGM devices during pregnancy, but blood glucose monitoring is recommended in addition to CGM.
Answer 3 is correct. About [%] of respondents chose this. “Recommend continued CGM with the addition of scheduled blood glucose monitoring.” Answer C is correct. The 2024 Standards of Care recommends CGM for individuals with type 1 diabetes during pregnancy but also recommends that it not replace pre-prandial and post-prandial blood glucose monitoring. Fasting, pre-prandial and post-prandial blood glucose monitoring is recommended for individuals with diabetes in pregnancy.
Finally, Answer 4 is incorrect. [%] chose this answer. “Recommend LS move to blood glucose monitoring and check fasting, pre-prandial and post-prandial glucose values.” Response D is not the best answer. We will recommend LS add blood glucose monitoring, but LS does not need to transition off CGM therapy.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join us live on June 11th at 11:30 am PST for our
Pregnancy & Diabetes
Level 2 Standards of Care Intensive
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, & understanding. This course reviews those special needs while focusing on Gestational Diabetes & Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, & prevention of complications during pregnancy. This is a helpful review for Certification Exams & those who want more information on people who are pregnant & live with diabetes.
Objectives:
- List three issues that affect pregnancy with diabetes.
- Describe the unique attributes of pre-existing diabetes in pregnancy & gestational diabetes.
- State the diagnostic criteria & management goals for gestational diabetes.
- Potential short-term & long-term complications of fetal exposure to hypoglycemia.
- Prevention measures to keep mother & baby healthy.
Learning Outcome:
Participants will gain knowledge of special considerations, individualized goals, and standards for people experiencing diabetes during pregnancy to improve outcomes.
Target Audience:
This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs/RDNs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions. The practice areas for RDs/RDNs for CDR reporting are healthcare, preventative care, wellness, and, lifestyle along with, education and research.
CDR Performance Indicators:
- 9.6.7
- 9.6.8
- 10.3.1
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working diabetes specialist and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | JR is out of lispro (Humalog) insulin and is panicking.
For last week’s practice question, we quizzed participants on JR is out of lispro (Humalog) insulin and is panicking. 42% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question.
Question: JR is a 19-year-old, living with type 1 diabetes. They use lispro (Humalog) insulin in their insulin pump. They just heard from their pharmacy that lispro is in short supply and they don’t know when they will be getting in the next shipment. JR tells you they are almost done with their current lispro vial and is panicking, asking what they should do.
Answer Choices:
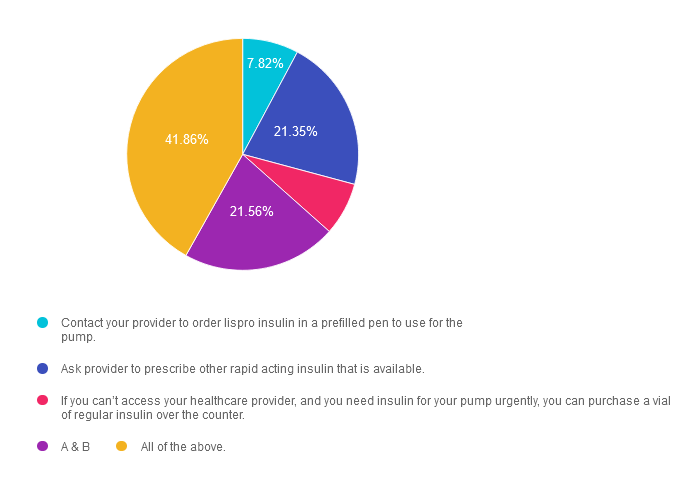
- Contact your provider to order lispro insulin in a prefilled pen to use for the pump.
- Ask provider to prescribe other rapid acting insulin that is available.
- If you can’t access your healthcare provider, and you need insulin for your pump urgently, you can purchase a vial of regular insulin over the counter.
- A & B
- All of the above.
Getting to the Best Answer
Answer 1 is incorrect. 7.8% chose this answer. “Contact your provider to order lispro insulin in a prefilled pen to use for the pump.” This answer is correct, but it is not the BEST answer. Since insulin pens are more readily available and it is the same insulin formulation and concentration, JR can use the insulin from a lispro insulin pen in their pump. However, there is a better answer, so, keep reading.
Answer 2 is incorrect. 21.35% of you chose this answer. “Ask provider to prescribe other rapid acting insulin that is available.” This answer is correct, but it is not the BEST answer. There are other rapid acting insulins such as NovoLog (insulin aspart) or the biosimilar insulin Admelog (insulin lispro injection) made by other manufacturers that are more readily available with the same insulin concentration. However, there is a better answer, so, keep reading.
Answer 3 is incorrect. About 7.4% of respondents chose this. “If you can’t access your healthcare provider, and you need insulin for your pump urgently, you can purchase a vial of regular insulin over the counter.” This answer is correct, but it is not the BEST answer. Regular insulin is available for purchase over-the-counter without the need for a prescription and is FDA approved for used in an insulin pump. However, there is a better answer, so, keep reading.
Answer 4 is incorrect. 21.6% chose this answer. “A & B”
Finally, Answer 5 is correct. 41.9% chose this answer. “All of the above.” YES, this is the best answer, all 3 options are correct. Of course, we encourage individuals to consult with their healthcare provider, since everyone responds differently to switching insulins. We wanted to raise awareness with this question, since many individuals with diabetes who use insulin lispro and Humalog vials for their insulin pumps have encountered shortages. We can reassure them that there are several options to get them by until lispro and Humalog insulin are back on the shelf. For more info, you can download our Insulin PocketCards.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this important learning activity!
Want to Learn more about recognizing and addressing Diabetes Distress?
Join us live on May 22nd & May 29th, 2024 for our
ReViVE 5 Diabetes Training Program:
Unlocking Hidden Barriers to Diabetes Management

“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
The ReVive 5 program is built on sound research from the Embark Trial and will revolutionize your approach to diabetes self-management education.
We have reassembled the Embark training team and created a resource binder of fantastic tools that we are excited to share with you in our ReVive 5 Diabetes Training Program. You are invited to join us to learn a step-wise, proven approach to addressing hidden barriers to diabetes self-management and glucose management.
You don’t need to be mental health expert or diabetes technology wiz to join this training or to integrate these new strategies into your daily practice.
ReVive 5 uses an integrated, evidence-based approach that provides health care professionals with a realistic 5-step approach to addressing the whole person, starting with emotional distress and incorporating a unique, but integrated approach to problem-solving glucose management difficulties.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the CDCES or BC-ADM Certification Exams.
Can’t join live? That’s okay. Your registration guarantees you access to the recorded version of the series, along with podcasts and resources for one full year.
Accredited Training Program:
- 15+ CEs – Includes the 7-hour ReVive 5 Training Program, Certificate, and 5 FREE bonus courses to supplement content.
- A comprehensive set of assessment tools, educational materials, log sheets, and resources.
Join us to gain the confidence and learn the skills needed to support people with diabetes to move forward in their self-management and discover the expert within.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
- Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
- Susan Guzman, PhD
- Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Speakers Interviews – Learn more about the ReVive 5 Team
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Weight-Inclusive Diabetes Care
- Honoring Excellence: Celebrating This Year’s Diabetes Education Scholarship Recipients
- Question of the Week | Who Benefits Most from Mindful Eating as a Primary Strategy? by Evgenia Evans, MS, RDN, CDCES
- Rationale of the Week | Triglyceride Management
- Fasting: Religion, Health, and Diabetes Care
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Diabetes Blog Bytes
Sign up now to receive the latest Blog Bytes in your inbox.
[yikes-mailchimp form="1"]