Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
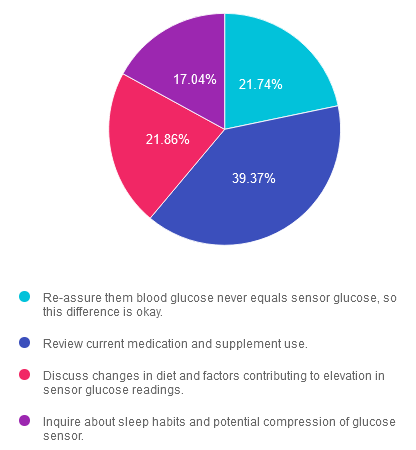
Rationale of the Week | Why are CGM readings higher than BG readings?
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST

Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
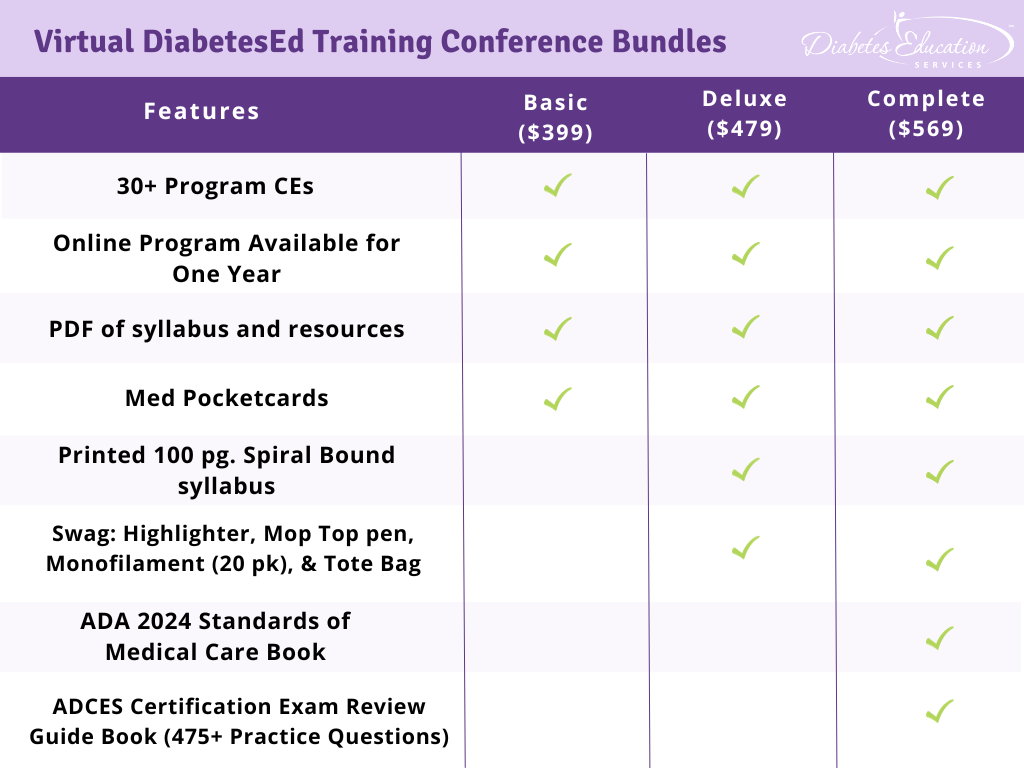
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Rationale of the Week | Which statement is accurate regarding treatment of steatosis?
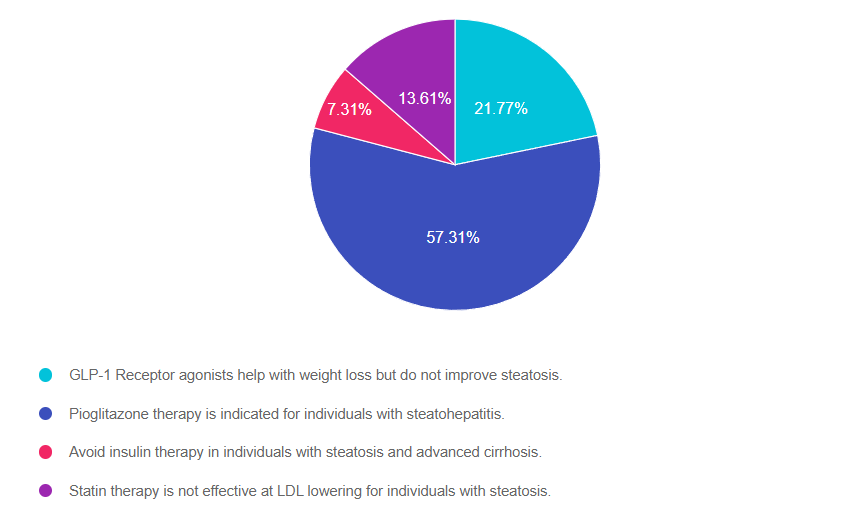
Answer 1 is incorrect. 21.77% chose this answer. “GLP-1 Receptor agonists help with weight loss but do not improve steatosis.” This juicy answer is tempting, but it is not the best answer. GLP-! RA’s, lower blood glucose levels and they also promote significant weight loss. This results in less glucose toxicity and a decrease in hepatic fat storage. Plus, they decrease the risk of cardiovascular disease which is co-associated with steatosis. See our Meds for Liver Disease Blog for more info.
Answer 2 is correct. 57.31% of you chose this answer. “Pioglitazone therapy is indicated for individuals with steatohepatitis.” Yes, this is the best answer. Pioglitazone (Actos) reduces blood glucose, and several studies demonstrate it is an effective treatment for steatosis and steatohepatitis. It also reduces the progression of fibrosis and cardiovascular risk. Since pioglitazone can cause fluid retention and weight gain, avoid using it in those with heart failure. See our Meds for Liver Disease Blog for more info.
Answer 3 is incorrect. About 7.31% of respondents chose this. “Avoid insulin therapy in individuals with steatosis and advanced cirrhosis.” With advanced cirrhosis, many of the oral medications may not be safe to use. The ADA recommends using insulin therapy, since it is safe and effective for people experiencing cirrhosis. Since people with cirrhosis are at higher risk of hypoglycemia, close monitoring of glucose levels is recommended. See our Meds for Liver Disease Blog for more info.
Finally, Answer 4 is incorrect. 13.61% chose this answer. “Statin therapy is not effective at LDL lowering for individuals with steatosis.” Lipid-lowering and antihypertensive meds need to be prescribed in people with steatosis as indicated. Statins are safe in individuals with steatohepatitis but avoid their use in those with decompensated cirrhosis. See our Meds for Liver Disease Blog for more info.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
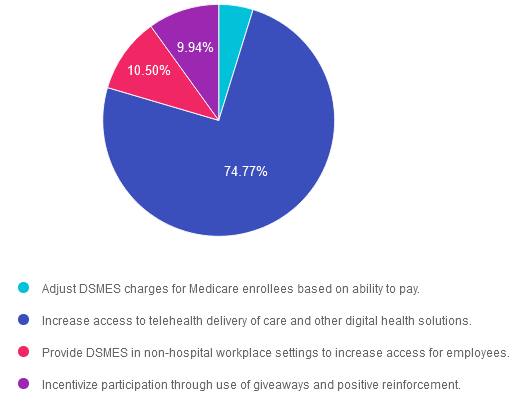
Rationale of the Week | How to Increase Participation in DSMES?
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Rationale of the Week | Assessing for Food Insecurity with Diabetes
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Rationale of the Week | Best approach for Religious Fasting?
For last week’s practice question, we quizzed participants on what is the best approach for religious fasting. 75% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: The 2024 Standards of Care reported individuals who fast have an increased risk for hypoglycemia, dehydration, hyperglycemia, and ketoacidosis.
Which of the following is an accurate health care statement regarding recommendations for religious fasting?
Answer Choices:
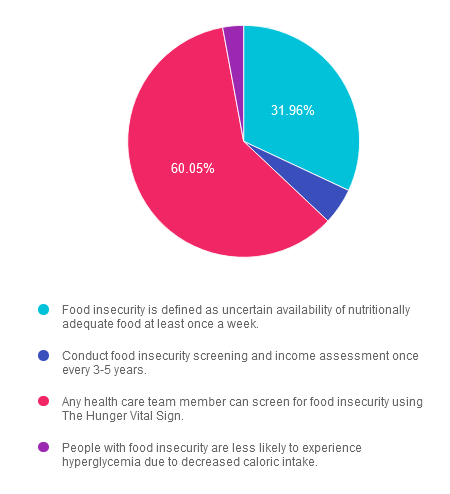
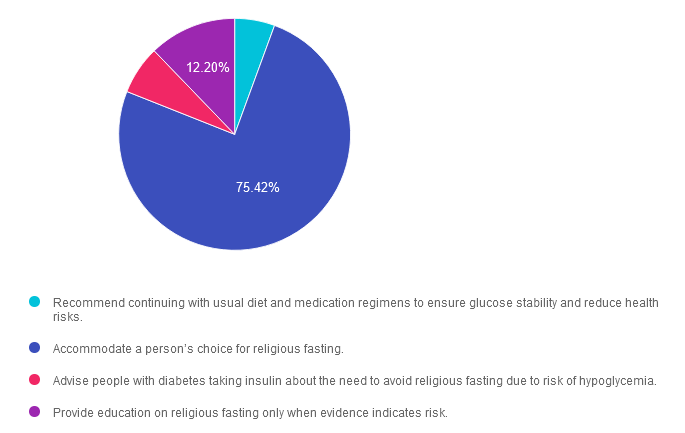
- Recommend continuing with usual diet and medication regimens to ensure glucose stability and reduce health risks.
- Accommodate a person’s choice for religious fasting.
- Advise people with diabetes taking insulin about the need to avoid religious fasting due to risk of hypoglycemia.
- Provide education on religious fasting only when evidence indicates risk.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 5.59% chose this answer. “Recommend continuing with usual diet and medication regimens to ensure glucose stability and reduce health risks.” Although religious fasting does change a person’s usual diet, sleep, and potentially medication regimen, evidence has shown that with education, most people with diabetes can safely complete a religious fast.
Answer 2 is correct. 75.42% of you chose this answer. “Accommodate a person’s choice for religious fasting.” Based on the 2024 Standards of Care, healthcare providers should accommodate a person’s choice for religious fasting.
Answer 3 is incorrect. About 6.78% of respondents chose this. “Advise people with diabetes taking insulin about the need to avoid religious fasting due to risk of hypoglycemia.” Although risk assessment is essential to review with each person with diabetes, the use of insulin is not a singular determinant of risk. Often, dose adjustments can reduce risk. The article “Diabetes and Ramadan: Practical Guidelines 2021”, referenced in the 2024 Standards of Care, includes a detailed description of how to stratify individual risk.
Finally, Answer 4 is incorrect. 12.20% chose this answer. “Provide education on religious fasting only when evidence indicates risk.” Healthcare providers should inquire about religious fasting and provide proactive education on monitoring glucose and how to modify medications, meal choices pre/post fast, fluid consumption, and activity planning.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Best action to address sudden Hyperglycemia due to Cellulitis?
For last week’s practice question, we quizzed participants on addressing sudden hyperglycemia due to cellulitis. 66% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: RL is 83, has Latent Autoimmune Diabetes, and takes degludec 17 units every morning along with metformin 500 XR twice daily. RL tells you that their left leg was suddenly swollen and red, so they went to urgent care and were started on a course of antibiotics. In the meantime, their CGM is showing elevated blood sugars in the 200 to 350 range during the day but often less than 100 at night. RL weighs 70kg, with a BMI of 23.4.
Based on this information, what action do you suggest?
Answer Choices:
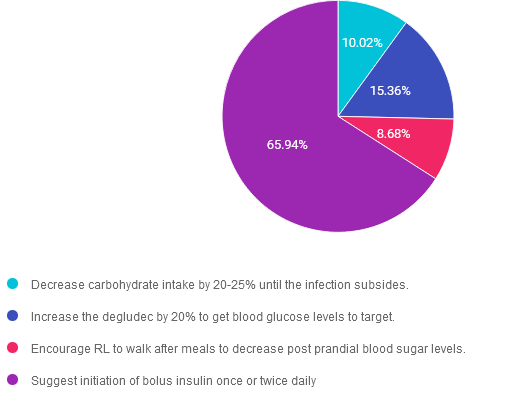
- Decrease carbohydrate intake by 20-25% until the infection subsides.
- Increase the degludec by 20% to get blood glucose levels to target.
- Encourage RL to walk after meals to decrease post prandial blood sugar levels.
- Suggest initiation of bolus insulin once or twice daily.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 10.02% chose this answer. “Decrease carbohydrate intake by 20-25% until the infection subsides.” Since RL has elevated glucose levels due to infection, drastically decreasing carbohydrate intake is not the best approach to manage glucose levels. We want to ensure RL has adequate nutrition given her infection and age.
Answer 2 is incorrect. 15.36% of you chose this answer. “Increase the degludec by 20% to get blood glucose levels to target.” It seems that RL needs more insulin to lower daytime glucose levels. However, RL is experiencing glucose levels less than 100 overnight, which puts them at risk of nocturnal hypoglycemia. If we increase basal insulin by 20%, this dramatic increase could cause a dangerous drop in overnight glucose levels and is not recommended.
Answer 3 is incorrect. About 8.68% of respondents chose this. “Encourage RL to walk after meals to decrease post prandial blood sugar levels.” Keeping active is always a good idea, but with blood sugars running 200-350 during the day, walking after meals won’t be enough to get glucose levels to target. Plus, it may not be safe to promote walking since they have an infection and a leg that is swollen and red.
Finally, Answer 4 is correct. 65.94% chose this answer. “Suggest initiation of bolus insulin once or twice daily.” YES, this the best answer. Counterregulatory hormones are released during periods of infection that contribute to insulin resistance and hyperglycemia. To get blood glucose levels to target, RL will need daytime bolus insulin to manage the hyperglycemia, which will promote healing. Of course, treatment with antibiotics will also help to lower glucose levels.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | RS Doesn’t Want to Get Weighed
For last week’s practice question, we quizzed participants on how to approach a person who does not want to be weighed during a quarterly diabetes appointment. 60% of respondents chose the best answer. If you are interested in learning more about the importance of providing weight inclusive care, this practice test question will set you up for success.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it here: Answer Question
Question:
RS arrives at their quarterly diabetes provider appointment and the medical assistant walks them to the scale, in the clinic hallway, to get their weight. RS politely explains that they feel uncomfortable being weighed but they are happy to share their stated weight. The medical assistant once again encourages RS to get on the scale and reassures RS that they don’t need to look at or know their weight. RS sighs, takes off their shoes and reluctantly gets on the scale to be weighed.
Which of the following best describes the end result of this situation?
Answer Choices:
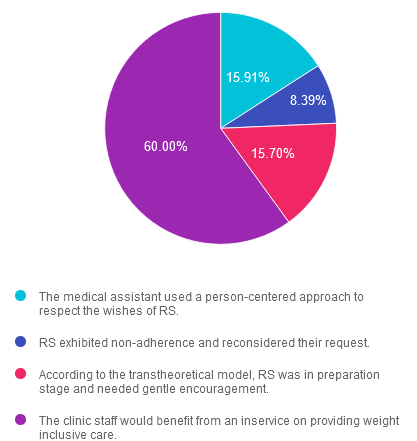
- The medical assistant used a person-centered approach to respect the wishes of RS.
- RS exhibited non-adherence and reconsidered their request.
- According to the transtheoretical model, RS was in preparation stage and needed gentle encouragement.
- The clinic staff would benefit from an inservice on providing weight inclusive care.
Getting to the Best Answer
If you are interested in providing weight inclusive care, this practice test question will set you up for success. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 15.91% chose this answer. “The medical assistant used a person-centered approach to respect the wishes of RS.” Instead of honoring the request to not be weighed, the medical assistant insisted RS step on the scale. A person centered, weight inclusive approach would respect RS’s request not to be weighed and accepted their stated weight.
Answer 2 is incorrect. 8.39% of you chose this answer. “RS exhibited non-adherence and reconsidered their request.” People with diabetes have the right to be weighed in a private space and they also have the right to decline to be weighed. In this situation, RS’s weight is not required to provide safe and effective medical care.RS is not “non-adherent”, they are simply expressing their need not to step on the scale.
Answer 3 is incorrect. About 15.70% of respondents chose this. “According to the transtheoretical model, RS was in preparation stage and needed gentle encouragement.” This juicy answer does not reflect the situation in the medical office at the scale. RS did not state that they were working on being comfortable with being weighed or that it would be helpful to be weighed. Instead RS told the MA twice that they don’t want to be weighed, but their request was not honored.
Finally, Answer 4 is correct. 60% chose this answer. “The clinic staff would benefit from an inservice on providing weight inclusive care.” YES, this is the best answer. If the staff were informed about weight inclusive care and reducing weight stigma, they would have honored RS’s request not to be weighed and documented their stated weight. This inclusive approach would help RS feel seen, heard and respected. RS would gain a positive association with their medical team and be more likely to return for future appointments.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this important learning activity!
Want to learn more about Weight Stigma?
 Enjoy our blog – Untangling Weight Stigma at Medical Visits.
Enjoy our blog – Untangling Weight Stigma at Medical Visits.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | What medication changes do you recommend?
For last week’s practice question, we quizzed participants on medication recommendations. 61% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
RL was newly diagnosed 43 with type 2 diabetes 6 months ago with an initial A1C of 10.1%. They have no cardiovascular disease and their renal function is within normal limits. At a recent office visit, you notice RL’s A1C has dropped to 7.3, their BP is 112/78 and the LDL cholesterol is 103mg/dL. RL’s current medication regimen includes, rosuvastatin 10mg, empagliflozin 25mg, metformin 1000 BID, glargine 12 units and aspirin 81mg.
Based on this information, what changes to RL’s medication plan do you recommend to the provider?
Answer Choices:
-
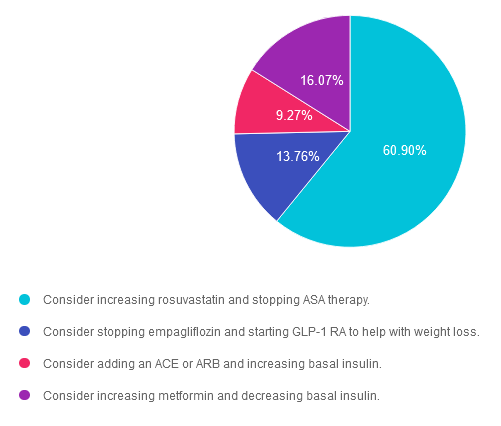
- Consider increasing rosuvastatin and stopping ASA therapy.
- Consider stopping empagliflozin and starting GLP-1 RA to help with weight loss.
- Consider adding an ACE or ARB and increasing basal insulin.
- Consider increasing metformin and decreasing basal insulin.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is correct. 60.90% chose this answer. “Consider increasing rosuvastatin and stopping ASA therapy.” – YES, this is the best answer. GREAT JOB. According to the ADA Standards of Care, the goal is to reduce the LDL by 50% and less than 70mg/dL. The max dose of rosuvastatin is 40mg and RL is only on 10mg. Increasing the dose of rosuvastatin will help decrease LDL levels. Aspirin therapy is indicated for people 55 years and older with an elevated CV risk. For those under 55, aspirin therapy is based on their CV risk profile. Since RL has no CV disease, aspirin therapy is not indicated.
Answer 2 is incorrect. 13.76% of you chose this answer. “Consider stopping empagliflozin and starting GLP-1 RA to help with weight loss.” This is not the best answer since there is no reason to stop empagliflozin when starting a GLP-1 RA. In addition, there is no mention in the vignette that RL has weight loss as a goal, so switching from an SGLT-2 to a GLP-1 is not indicated at this time.
Answer 3 is incorrect. About 9.27% of respondents chose this. “Consider adding an ACE or ARB and increasing basal insulin.” This is not the best answer, since the first part of the response isn’t correct. RL has great renal function and their BP is below the target of 130/80, so an ACE or ARB is not indicated at this time.
Finally, Answer 4 is incorrect. 16.07% chose this answer. “Consider increasing metformin and decreasing basal insulin.” This is not the best answer, since the metformin is already very close to the maximum dose of 2,550 mg day and we need more information about the fasting blood glucose levels before increasing the basal insulin. Most importantly, the first answer is a better answer.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
-
- Dates: April 17-19th, 2024
-
- Registration Fee: $399-$569 (see more about reg. options below)
-
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
-
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
-
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.