
Written by Monique Jackson, MSN, CFNP, WHCNP, CDCES
A new study finds that hemoglobinopathies may distort A1C accuracy for people of African descent living with diabetes.
African Americans at risk for falsely low A1cs due to Hemoglobin Variants
Hemoglobin variants don’t increase the risk for diabetes, but it can affect the results of A1C tests. African Americans Heterozygous for the common hemoglobin variant HbS may have, for any given level of mean glycemia, lower A1C by about 0.3% then those without the trait. Another genetic variant, X-linked glucose-6-phosphate dehydrogenase G202A, carried by 11% of African Americans, was associated with a decrease in A1C of about 0.8% in homozygous men and 0.7% in homozygous women compared with those without the variant (American Diabetes Association, Standards of Care in Diabetes-2021; 16).
Health care professionals often use A1C test results to guide decisions about diabetes care, such as changes to medication, meal plan, or physical activity routine to manage diabetes. In those with certain hemoglobin variants, A1C is not accurate for diagnosing and managing diabetes. Different tests that accurately reflect long term glucose levels are needed for early diagnosis and to provide needed medical management that prevents complications.
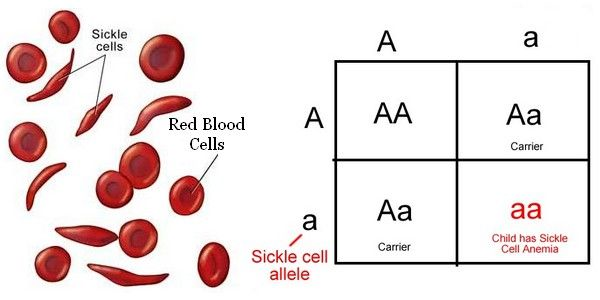
Mismatch between Glucose and A1c – My Clinical Finding
At my clinic, where I work as a Diabetes Nurse Specialist, an African American individual arrived with a high random glucose and mildly abnormal A1C. Reviewing their lab work, I noticed that the random blood glucose was 300 mg/dl and the A1C was at approximately 7.0%. When I converted the A1C to average blood glucose and compared with the elevated reading in the logs, the numbers did not match up. I realized that this individual had one of the hemoglobin variants (Sickle Cell anemia) HbS. I ended up starting them on Metformin for blood sugar, Atorvastatin because of the guidelines that everyone with Diabetes should be on a statin, Aspirin to prevent heart attack, and Lisinopril for blood pressure control.
Without this clinical finding that the elevated blood sugars were not reflected in the A1c, this individual might not have been started on diabetes treatment, because of the false low A1C.
A1C reflects glucose concentration from the past 2-3 months, but this relationship may differ between those with nutritional deficiencies, anemia, or genetic hemoglobinopathies, including the Sickle cell trait.
Since A1C measures the percentage of glycosylated hemoglobin, individuals who possess variants of hemoglobin can exhibit falsely low readings.
Fructosamine testing, which evaluates albumin glycosylation for the past 2-3 weeks, may be a better measure to help people with diabetes monitor and manage their blood glucose levels in cases where the A1C test cannot be used and/or a short-term monitoring window is desired.
Summary and Notes for the Future
It is important to consider the results of the A1C, fasting blood glucose, two-hour glucose tolerance test, random blood glucose, and or fructosamine when you are screening someone with diabetes who is diagnosed with a Hemoglobin variant.
A1C testing on two different occasions to diagnose diabetes for those with Hbs variants is not recommended, because it will yield false low results. To diagnose a person with diabetes and Hbs variants, the ADA recommends only plasma blood glucose criteria be used to diagnose diabetes.
More research is needed on the diagnoses of diabetes utilizing the A1C in populations with increased prevalence of Hbs variants. In addition, we need research aimed toward providing more accurate tests for the diagnosis and management of conditions associated with increased red blood cells turnover, such as sickle cell disease, hemoglobinopathy variants, pregnancy (second and third trimester).
Welcome, Monique Jackson, MSN, CFNP, WHCNP, CDCES, our new Blog Content Writer!
We are so excited to introduce our newest DiabetesEd Specialist Blog Contributor, Monique Jackson, MSN, CFNP, WHNP, CDCES.
Monique is a Board-Certified Family Nurse Practitioner licensed in the State of California and a member of the California Nurse Practitioner Association and a member of the American Association of Nurse Practitioners. Monique resides in Los Angeles, California. She enjoys gardening, sewing, reading, learning new things, fine dining in her spare time and spending time with her family.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.