
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
For last week’s practice question, we quizzed participants on ADCES 7 Self-Care Behaviors. 71% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.

When providing Diabetes Self-Management Education (DSME), which of the following list includes the ADCES 7 Self-Care Behaviors?

Answer A is incorrect. 8.94% chose this answer, “Healthy Eating, Being Active, Insulin Adjustment.” This answer is so close. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Insulin Adjustment is just one component of Taking Medication.
Answer B is correct. 71.95% of you chose this answer, “Monitoring, Problem Solving, Healthy Coping.” Great JOB! This answer is the best answer. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. This great info to be familiar with for any upcoming certification exam in your future!
Answer C is incorrect. About 10.57% of respondents chose this: “Reducing Risks, Being Active, Social Support.” This answer is so close. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Social Support falls under the category of Healthy Coping and is not it’s own category.
Finally, Answer D is incorrect. 8.54% chose this answer, “Problem Solving, Reducing Risk, Positive Self-Attitude.” Another juicy answer. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Positive Self-Attitude might fall under the category of Healthy Coping, but is not it’s own category.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
For last week’s practice question, we quizzed participants on LDL target for 2026. 55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.
RZ is 47 years old with type 2 diabetes and hypertension. RZ takes metformin 1000 mg BID, plus lisinopril 20mg daily. RZs LDL is 140 mg/dL.
Based on the most recent ADA Standards, what is the LDL Cholesterol target for RZ?
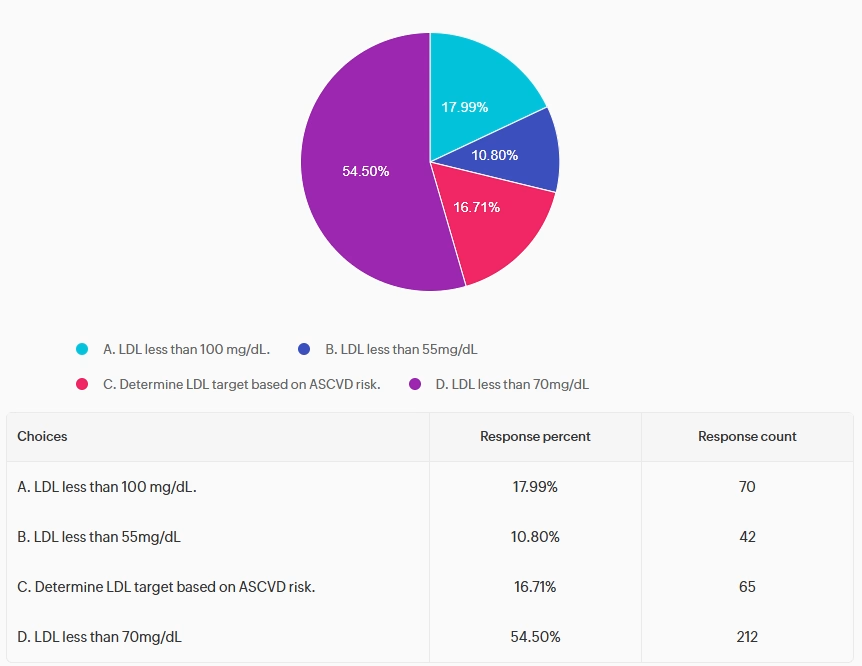
Answer A is incorrect. 17.99% chose this answer, “LDL less than 100 mg/dL.” This juicy answer was the previous goal for LDL.
But for the past few years, the ADA has established an LDL cholesterol goal of less than 70mg/dL (often using high-intensity statins) in diabetes. Reducing the LDL significantly decreases the risk of major cardiovascular events (heart attacks, strokes) by roughly 20% for every 39 mg/dL reduction. This target stabilizes plaque, slows atherosclerosis, and improves mortality, especially for high-risk individuals.
Answer B is incorrect. 10.80% of you chose this answer, “LDL less than 55 mg/dL.” This answer is tempting. The LDL goal off 55 mg/dL is recommended for individuals with diabetes with existing CV disease. Given that RZ has type 2 and hypertension and a LDL of 140 mg/dL, the ADA goal is to get LDL to half of the current value AND less than 70 mg/dL.
Answer C is incorrect. 16.71% chose this answer, “Determine LDL target based on ASCVD risk.” It might be helpful to calculate CV risk, but the ADA Standards make taking action simple and clear. If a person is 40 years or older, the LDL Goal is less than 70mg/dL and 50% reduction from their current LDL level. For people with diabetes with existing CV disease, the LDL goal is less than 55 mg/dL.
Finally, Answer D is correct. 54.50% of respondents chose this: “LDL less than 70mg/dL.” GREAT JOB! Based on the ADA 2026 guidelines, the LDL Goal is less than 70mg/dL and 50% reduction from their current LDL level, for people with diabetes over the age 40 with CV risk factors.
Reducing the LDL significantly decreases the risk of major cardiovascular events (heart attacks, strokes) by roughly 20% for every 39 mg/dL reduction. This target stabilizes plaque, slows atherosclerosis, and improves mortality, especially for high-risk individuals.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
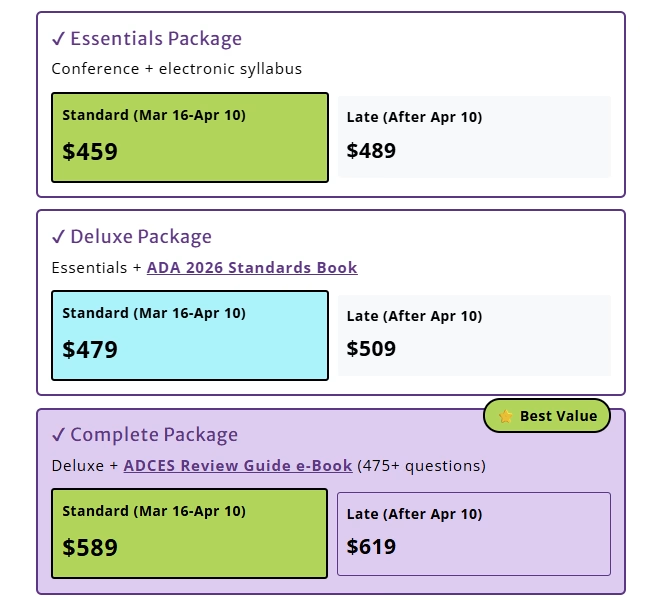
Save $75 thru April 30th
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
For last week’s practice question, we quizzed participants on the next steps after 12% weight loss. Over 85% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.
Question of the Week:
KC is a 62-year-old individual with type 2 diabetes who presents for follow-up after initiating a weight loss program 3 months ago. They report consuming approximately 1,000–1,100 kcal/day and have lost 12% of their body weight, with a current rate of weight loss averaging 5% in the last month.
Their diet excludes most grains and fruits, and they report occasional fatigue and constipation. Current medications include metformin, tirzepatide, and atorvastatin.
Based on current standards of care, what is the most appropriate response regarding nutrition and weight changes?
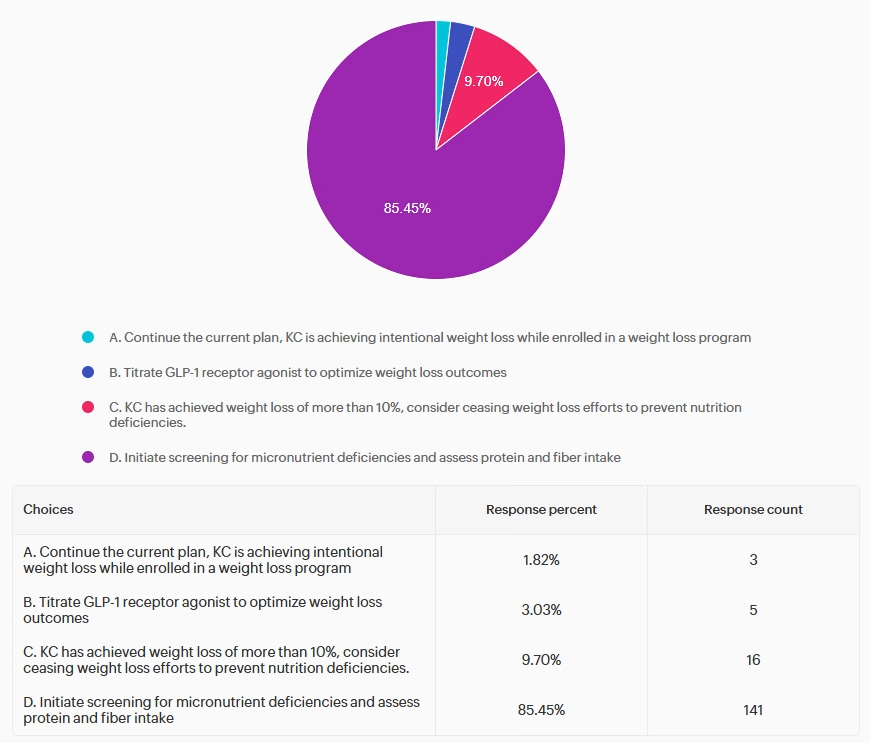
Answer 1 is incorrect. 1.82% chose this answer, “Continue the current plan, KC is achieving intentional weight loss while enrolled in a weight loss program.” Although KC is achieving clinically significant weight loss, they have multiple risk factors for nutrition deficiencies, including intake <1,200 kcal/day, rapid weight loss (>4% per month), age >50, and restriction of nutrient-dense food groups.1 These risk factors warrant further evaluation before continuation without modification.
Answer 2 is incorrect. 3.03% of you chose this answer, “Titrate GLP-1 receptor agonist to optimize weight loss outcomes.” While GLP-1 receptor agonists are effective for weight management, further intensification may not be appropriate in the setting of already rapid weight loss and inadequate intake. Additional assessment and individualization of outcome goals is recommended before intensification is initiated.
Answer 3 is incorrect. 9.7% chose this answer, “KC has achieved weight loss of more than 10%, consider ceasing weight loss efforts to prevent nutrition deficiencies.” While monitoring weight change is necessary, automatically discontinuing weight loss efforts may not be recommended. Instead, care should focus on optimizing nutritional adequacy, potentially incorporating supplementation, and adjusting the treatment plan to support safe, sustainable weight-loss goals while minimizing nutrition and medical risk.
Finally, Answer 4 is correct. 85.5% of respondents chose this: “Initiate screening for micronutrient deficiencies and assess protein and fiber intake” GREAT JOB! KC meets several high-risk criteria for nutrient deficiencies, including low caloric intake (<1200 calories per day), rapid weight loss (>4% per month), older age, and limited dietary variety. The current standards of care recommend screening for micronutrient deficiencies within these high risk groups. Screening is guided by clinical judgement but nutrients of concern include iron, calcium, magnesium, zinc, B1, B12, Vitamin C, and fat-soluble vitamins A, D, E, and K.1 It is also recommended to ensure adequate protein intake to preserve lean mass and ensure adequate fiber and fluid intake to address constipation in individuals consuming very low-calorie intake.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
For last week’s practice question, we quizzed participants on checkpoint inhibitors triggering hyperglycemia. 34% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.
Betty, a 60-year-old female, is receiving pembrolizumab, an immune checkpoint inhibitor, as treatment for melanoma. She is worried about the potential adverse effects. She is very concerned about the risk of developing diabetes. Her recent lab work shows normal fasting blood glucose and hemoglobin A1c.
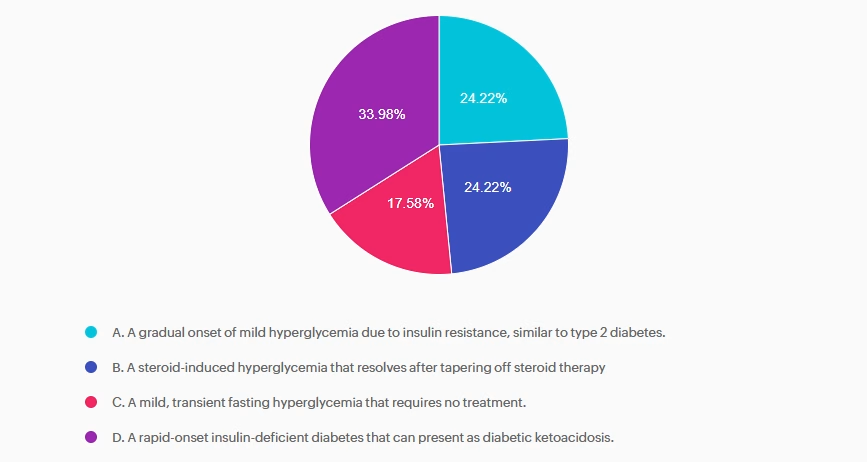
Answer 1 is incorrect. 24.22% chose this answer, “A gradual onset of mild hyperglycemia due to insulin resistance, similar to type 2 diabetes.” This answer is incorrect. Immune checkpoint inhibitor medications do not cause mild hyperglycemia but instead cause significant hyperglycemia and DKA similar to type 1 diabetes.
Answer 2 is incorrect. 24.22% of you chose this answer, “A steroid-induced hyperglycemia that resolves after tapering off steroid therapy.” This answer is incorrect. Though steroid treatment is often needed, hyperglycemia in immune checkpoint inhibitor-associated diabetes is not resolved after tapering off steroids.
Answer 3 is incorrect. About 17.58% of respondents chose this: “A mild, transient fasting hyperglycemia that requires no treatment.” This answer is incorrect. Though steroid treatment is often needed, hyperglycemia in immune checkpoint inhibitor-associated diabetes is not resolved after tapering off steroids.
Finally, Answer 4 is correct. 33.98% chose this answer, “A rapid-onset insulin-deficient diabetes that can present as diabetic ketoacidosis.” This answer is correct. Due to immune checkpoint inhibitor-induced immune system alterations, hyperglycemia and insulin deficiency can rapidly develop, often leading to DKA.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
In diabetes care, what is the reported percentage
of patients who have missed or not returned for follow-up care due to feelings of shame, blame, or judgment?
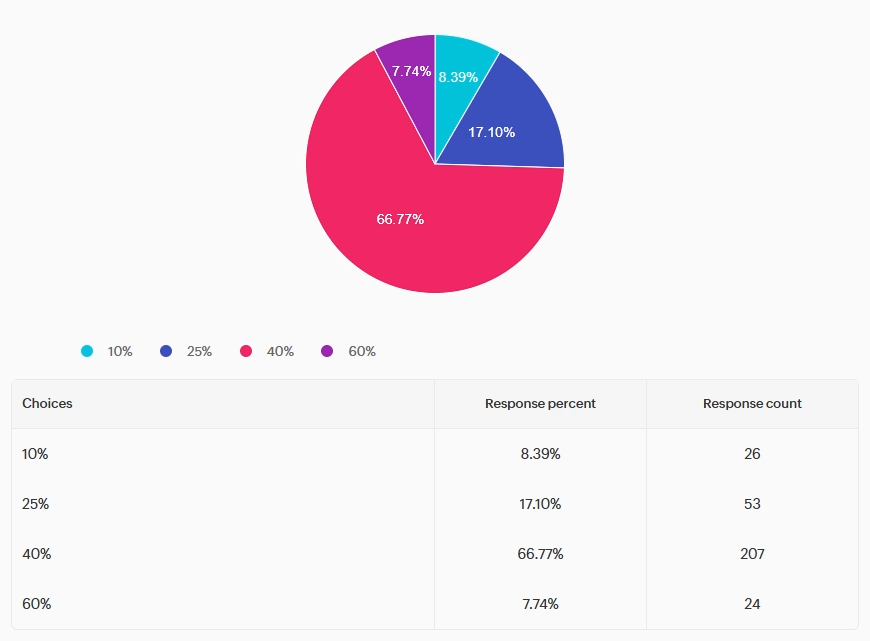
Answer A is incorrect: 8.39% chose this answer, “10%.” This answer underestimates the problem. Research indicates that approximately 40% of patients with diabetes may miss or avoid follow-up appointments because they experience feelings of shame, blame or judgment related to their condition or care. This highlights the importance of delivering diabetes care with stigma-free, supportive communication approaches as a means to improve engagement and outcomes
Answer B is incorrect: 17.10% chose this answer, “25%.” This answer underestimates the problem. Research indicates that approximately 40% of patients with diabetes may miss or avoid follow-up appointments because they experience feelings of shame, blame or judgment related to their condition or care. This highlights the importance of delivering diabetes care with stigma-free, supportive communication approaches as a means to improve engagement and outcomes.
Answer C is correct: 66.77% chose the correct answer, GREAT JOB. “40%.” Per the 2026 ADA Standards of Care, bone health needs to be assessed in men aged ≥50 years with type 2 diabetes and an A1c >8%. He is also on pioglitazone, a thiazolidinedione, which is another risk factor for low bone density.
Answer D is incorrect: 7.74% chose this answer, “60%.” This answer overestimates the problem. Research indicates that approximately 40% of patients with diabetes may miss or avoid follow-up appointments because they experience feelings of shame, blame or judgment related to their condition or care. This highlights the importance of delivering diabetes care with stigma-free, supportive communication approaches as a means to improve engagement and outcomes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on who needs to have a bone density evaluation according to the 2026 ADA Standards. 47% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below:
According to the 2026 ADA Standards of Care, what individuals should be recommended to have a bone density evaluation using dual-energy X-ray absorptiometry to evaluate for bone loss?
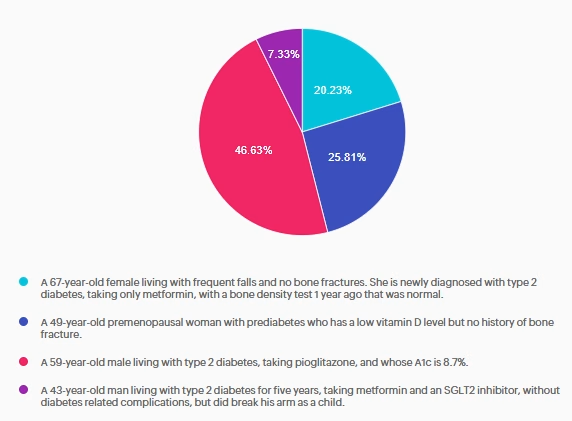
Answer A is incorrect: 20% chose this answer, “A 67-year-old female living with frequent falls and no bone fractures. She is newly diagnosed with type 2 diabetes, taking only metformin, with a bone density test 1 year ago that was normal.” This answer is tempting but incorrect. Per the 2026 ADA Standards of Care, she does meet criteria for assessing bone health due to her diagnosis of type 2 diabetes and risk factor of frequent falls, but she had a bone density test 1 year ago. Currently, the recommendation is to re-evaluate the bone density test in 2-3 years.
Answer B is incorrect: 26% chose this answer, “A 49-year-old premenopausal woman with prediabetes who has a low vitamin D level but no history of bone fracture.” This answer is incorrect. Per the 2026 ADA Standards of Care, it is recommended to assess bone health in postmenopausal women with other diabetes specific risk factors. This risk factor does not include low vitamin D levels.
Answer C is correct: 47% chose the correct answer, GREAT JOB. “A 59-year-old male living with type 2 diabetes, taking pioglitazone, and whose A1c is 8.7%.” Per the 2026 ADA Standards of Care, bone health needs to be assessed in men aged ≥50 years with type 2 diabetes and an A1c >8%. He is also on pioglitazone, a thiazolidinedione, which is another risk factor for low bone density.
Answer D is incorrect: 7% chose this answer, “A 43-year-old man living with type 2 diabetes for five years, taking metformin and an SGLT2 inhibitor, without diabetes related complications, but did break his arm as a child.” This answer is incorrect. Per the 2026 ADA Standards of Care, he has no diabetes-specific risk factors for bone loss. Diabetes duration is less than 10 years, he has no diabetes related complications such as peripheral or autonomic neuropathies, he is not on a high-risk medication for bone loss, and he has not had a bone fracture as an adult.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
For last week’s practice question, we quizzed participants on JR wanting treatment for pancreatic parasites, and what would be the best response. We share the scoop on pancreatic parasites below. 94.8% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
JR is hospitalized with influenza. They have a history of prediabetes but now have persistent glucose readings between 220–260 mg/dL and are started on basal-bolus insulin.
JR is upset and states: “I’ve been reading that pancreatic parasites can cause of diabetes. No one is treating my infection.”
What is the BEST response?
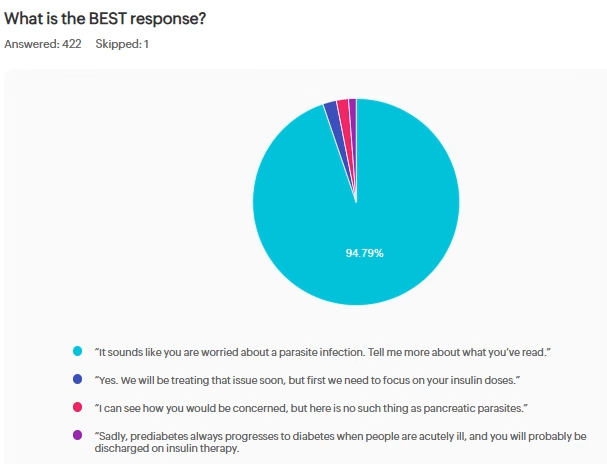
Answer A is correct: 94% chose this answer, “It sounds like you are worried about a parasite infection. Tell me more about what you’ve read.” Great job. A is the best answer because it uses person-centered, nonjudgmental communication, as recommended by the ADA. It avoids dismissive language and explores misinformation respectfully. It preserves the therapeutic alliance.
Since many of you mentioned that patients are asking about parasites causing diabetes – here is the scoop. This false rumor is based on a video from a scientist named Hulda Clark that has since been debunked. Clark falsely claimed that most diseases, including AIDS, Cancer and diabetes, were caused by different parasites and could be cured with an electric “zapper.” Authorities took action against Clark’s “zapper” and other examples of her unproven treatments that she claimed could “cure all diseases” both before and after her death. Read more here
John Buse, MD a professor at the University of North Carolina School of Medicine, said there is a long-standing theory that infection by certain viruses could trigger the body’s immune response that leads to type 1 diabetes, but that no link has been established between a parasitic infection and any type of diabetes. He also said there is no evidence that methanol (another proposed false claim) — a poison — would have any different effect on someone with diabetes than on a person without high blood sugar.
Answer B is incorrect: 3% chose this answer, “Yes. We will be treating that issue soon, but first we need to focus on your insulin doses.” Option B offers a false narrative saying that they are going to treat the parasitic infection then shifts focus to the blood glucose, without recognizing JR’s emotional distress.
Answer C is incorrect: 2% chose this answer, “I can see how you would be concerned, but here is no such thing as pancreatic parasites.” Option C does initially recognize the emotions but then ends with a dismissive tone, that may make JR feel defensive and unheard.
Answer D is incorrect: 1% chose this answer, “Sadly, prediabetes always progresses to diabetes when people are acutely ill, and you will probably be discharged on insulin therapy.” Option D completely ignores the emotional distress in addition to making assumptions that may not be true.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
For last week’s practice question, we quizzed participants on which of the following would NOT justify providing individual DSMES instead of group DSMES. 55.1% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
After the initial assessment JM is scheduled for an individual visit instead of a group DSMES class.
According to Medicare guidelines, which of the following would NOT justify providing individual DSMES instead of group DSMES?
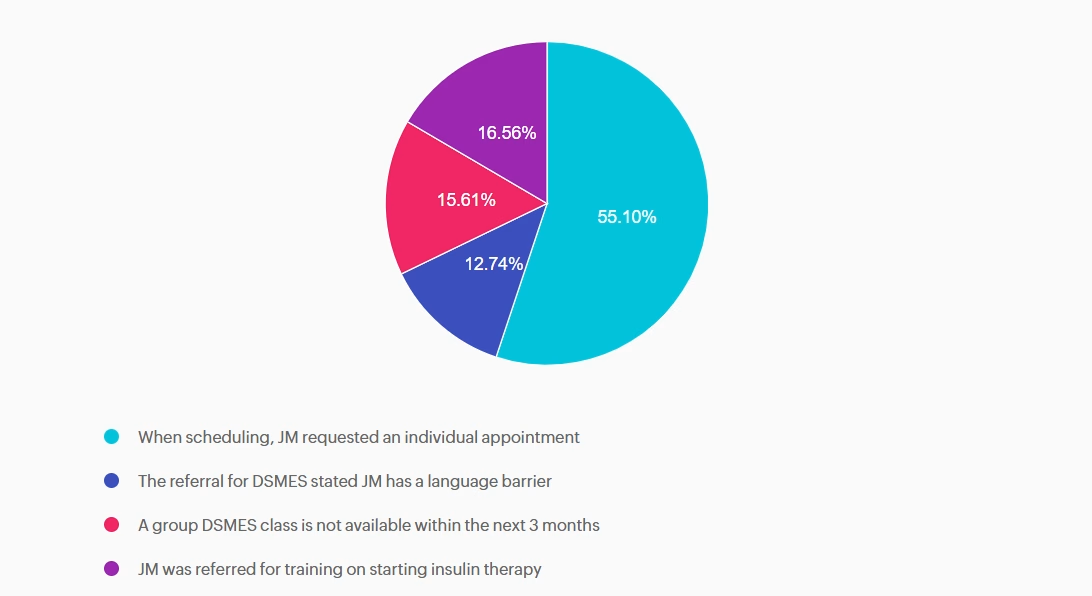
Answer A is correct: 55.1% chose this answer, “When scheduling, JM requested an individual appointment” Answer A is correct; it does NOT justify individual DSMES. Although diabetes care should be patient-centered, patient preference alone does not meet Medicare criteria for individual DSMES. Medicare requires the referring provider document justification of barriers to group learning which can include clinical, educational, or psychosocial need.
Answer B is incorrect: 12.74% chose this answer, “The referral for DSMES stated JM has a language barrier” Answer B is incorrect and does justify individual DSMES. Language barriers can significantly limit participation in group DSMES. Medicare recognizes a referral with stated language and communication needs as valid justification for an individual visit.
Answer C is incorrect: 15.61% chose this answer, “A group DSMES class is not available within the next 3 months” Answer C is incorrect and does justify individual DSMES. Medicare will approve individual DSMES if no group class is available for two months or longer from the date on the referral.
Answer D is incorrect: 16.56% chose this answer, “JM was referred for training on starting insulin therapy” Answer D is incorrect and does justify individual DSMES. A referral for initiation of insulin therapy requires individualized instruction. This can include injection technique, dose adjustment, hypoglycemia prevention, and problem-solving. Medicare considers this
an appropriate reason for individual DSMES.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.