
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
JR has type 2 diabetes and is trying to lose weight by eating less and moving more. JR asks your advice about drinking diet sodas.
Based on the recommendations in the ADA Standards of Care, what is the best response?
Click here to test your knowledge!
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Want to learn more about Hospitals & Hyperglycemia? Join us for our

Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control and outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest ADA Standards and provide links to resources and inpatient management templates.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For our July 13th Question of the Week, 80% of respondents chose the best answer. GREAT JOB! We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: JR is 78, lives alone, and manages their diabetes with bolus insulin at breakfast and dinner and basal insulin at night. For the past few months, JR has had trouble remembering to take insulin with meals and JR’s most recent A1c is above 9%.
Which of the following is most likely contributing to this change of behavior for JR?
Answer Choices:
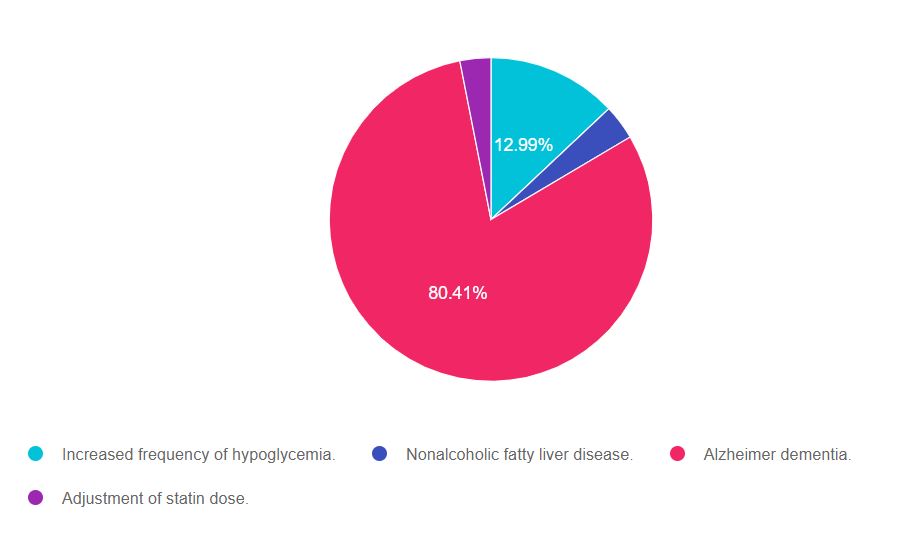
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Being familiar with the experiences and co-conditions that impact older people’s ability to self-manage diabetes will be helpful for the exams.
Answer 1 is incorrect, 12.99% chose this answer, “Increased frequency of hypoglycemia.” This is the juicy answer, but not the best one. Since JRs A1c is elevated, we don’t suspect hypoglycemia is causing the missed bolus doses of insulin. However, it is important to assess for hypoglycemic events for older individuals taking insulin.
Answer 2 is incorrect, 3.51% of you chose this answer, “Nonalcoholic fatty liver disease.” It is true that more people with diabetes are experiencing fatty liver disease. However, we get no indication from the question that JR has visceral adiposity, jaundice skin color or elevated liver enzymes. And fatty liver disease in the early stages is not commonly associated with forgetfulness.
Answer 3 is correct, 80.41% of you chose this answer, “Alzheimer dementia.” GREAT JOB, this is the best answer. People with diabetes and hyperglycemia are at higher risk of Alzheimer and vascular dementia. Dementia can decrease the ability to remember to take insulin and other medications which can then lead to hyperglycemia which can worsen dementia. If you suspect that someone is forgetting to take insulin due to dementia, reaching out to the referring provider for a cognitive assessment and evaluation is warranted. See screening tools here.
Answer 4 is incorrect, 3.09% of you chose this answer “Adjustment of statin dose.” A few years back, there was a social media buzz that statin therapy is associated with decreased cognition and memory loss. According to the ADA Standards of Care, multiple well designed studies have found no association between statins and memory loss.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our

We have updated this content based on the ADA 2021 Standards of Care.
We are living longer and more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering reduction of medication and insulin therapy intensity. The older population has unique issues and special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LS is 26 weeks pregnant and just discovered she has gestational diabetes. LS asks you what type of meal planning approach will help keep her and the baby healthy.
According to the ADA Standards of Care, what is the most accurate response?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our

People living with diabetes who are pregnant are confronted with a variety of issues that require special attention, education, and understanding.
This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Want to learn more about Pregnancy & Diabetes? Join us live for our
People living with diabetes who are pregnant are confronted with a variety of issues that require special attention, education, and understanding.
This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our July 6th Question of the Week, 80% of respondents chose the best answer. We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
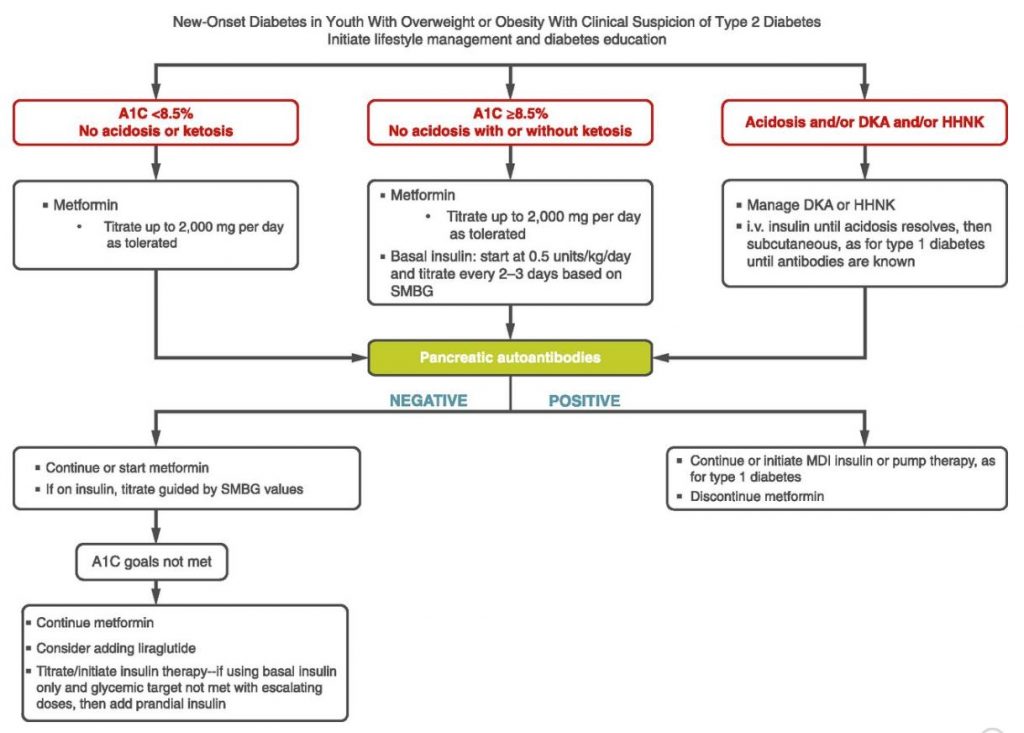
Question 1: JR is a 15-year-old with newly diagnosed type 2 diabetes, with an A1c of 8.3% and elevated lipids.
In addition to nutrition and activity coaching, which of the following medications are FDA approved for pediatrics?
Answer Choices:
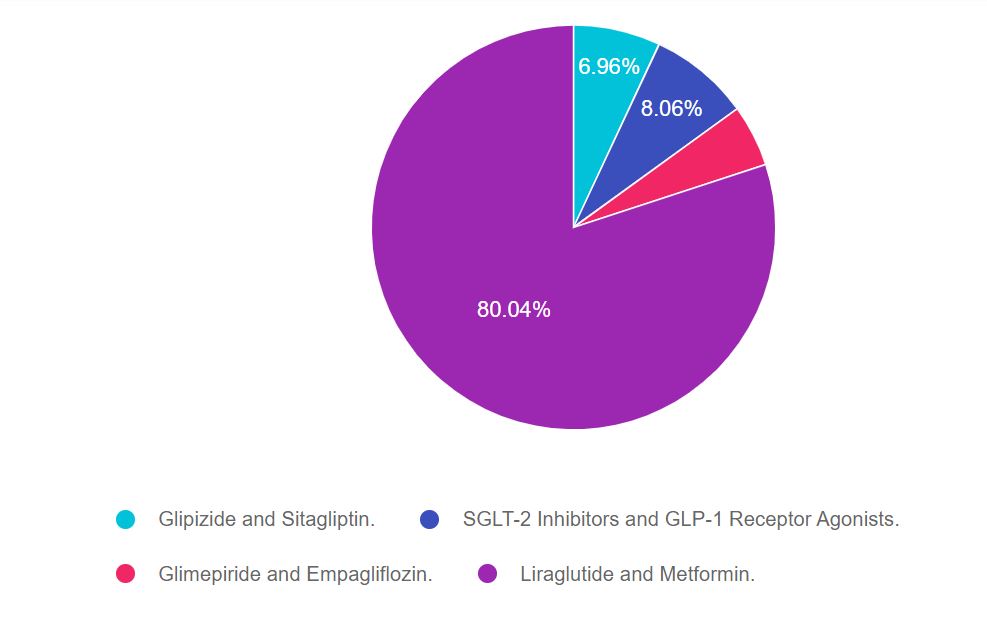
As shown above, the most common choice was option 4, the second most common answer was option 2, then option 1, and finally option 3.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to be familiar with knowledge of special populations like pediatrics, older folks and management of diabetes during pregnancy. According to the ADA Standards of Care, Section 13 of Children and Adolescents, here is the best answer.
Answer 1 is incorrect, 6.96% chose this answer, “Glipizide and Sitagliptin.” Although commonly used in adults, sulfonylureas, including glipizide and DPP-IV’s including Sitagliptin, are not FDA approved for people under the age of 18.
Answer 2 is incorrect, 8.06% of you chose this answer, “SGLT-2 Inhibitors and GLP-1 Receptor Agonists.” Although commonly used in adults, SGLT-2s are not FDA approved for people under the age of 18. There is one GLP-1 Receptor Agonists, liraglutide (Victoza) approved for use in pediatrics over the age of 10. However, none of the other GLP-1 RAs are FDA approved for pediatrics.
Answer 3 is incorrect, 4.95% of you chose this answer, “Glimepiride and Empagliflozin.” Although commonly used in adults, sulfonylureas, including glimepiride and SGLT-2 Inhibitors, including empagliflozin, are not FDA approved for people under the age of 18.
Answer 4 is Correct, 80.04% of you chose this answer “Liraglutide and Metformin.” Great Job! For children under the age of 18, the only FDA approved pharmacologic interventions include metformin, liraglutide and insulin.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our

This course includes updated goals and guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes and their families.
We discuss the clinical presentation of diabetes, goals of care, and normal growth and development through the early years through adolescence. Strategies to prevent acute and long term complications are included with an emphasis on positive coping for family and child with diabetes.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Delivering person-centered high quality diabetes care to high-risk individuals with diabetes is no easy task in our current complicated health environment. We are excited to share our interview with Dr. Avni Shah, Founder of Vayu Health, and her vision to provide equitable diabetes care delivery for our most vulnerable populations. Dr. Shah and her team are proposing a radical new equity focused-approach to diabetes care. To learn more, read our interview below.
“Our vision is to transform the lives of under served Medicaid members living with multiple chronic conditions, behavioral health needs, and social determinants of health (SDOH) through a team-based approach to care that places people at the center of decisions about their own health. We are passionately driven to improve health, equity, and experiences for every person we work with, while also lowering costs,” said Dr. Avni Shah.
Dr. Shah says their care model is rooted in trusting relationships with patients, and also with the providers, community partners and health plans that they work with. To sustain vibrant, patient-centered programs they are designing a payment model that rewards their care team for doing the right thing at the right time for these vulnerable populations.
They believe that a major shift is needed in the way care is delivered for under resourced people living with chronic conditions, especially sub optimally managed diabetes, and are currently looking to build out their clinical team, including a Certified Diabetes Care and Education Specialist (CDCES) and a Licensed Clinical Social Worker (LCSW).
1. What motivated you to leave a traditional work setting as a Peds Endo and take the risk to create a new health care model for Medicaid members living with diabetes?

2. What do you consider the biggest shortcomings in our current approach to providing diabetes care?
3. Describe your future vision and model of diabetes care provision.
We believe that it is past time for a seismic change in chronic care management, especially for diabetes. Our primary-care based model is what is needed right now for people with diabetes and will include the following key components:
4. Do you have a favorite quote?
I have many quotes I love, but none that are a favorite. So here are a few:
Vayu Health was started by physicians who work extensively with adults and children with not only diabetes, but other chronic conditions, behavioral health issues and social risk factors. Vayu’s team recognized that despite best efforts of providers and patients, of new drugs and technologies, and of increased spending, population health outcomes have not improved significantly over the last 20 years for individuals living with chronic conditions such as diabetes, especially for those with low incomes. COVID-19 has only intensified the call for change as it has disproportionately impacted individuals already marginalized by our healthcare system failures.
To address this urgent crisis, fundamental change in the healthcare system is needed and Vayu Health is poised to create this change.
Identifying System Failures and Building Solutions
To successfully build their model, Vayu first identified the healthcare system failures, cataloging the barriers to people with diabetes receiving the right care. They identified four key barriers that needed to be addressed:
Vayu Health’s Innovative Model
Vayu Health is taking on each of these systemic barriers, and addressing them in a cohesive, person-centered care model. As Medicaid members disproportionately experience care failures, Vayu is focusing on Medicaid managed care patients, living with diabetes and other chronic conditions.
They are collaborating with one of California’s largest Medicaid managed care health plans and a California community health center to develop and integrate Vayu Health’s unique systems approach, including a new value-based payment that will incentivize doing the right thing at the right time for patients. This collaboration is the first step in a systematic shift in the way community primary care providers and patients experience care and the way that Medicaid managed health plans cover the costs.
In addition to the best practice chronic condition care model, a healthcare ecosystem will be developed which will incorporate the following system elements:
Equity-focused start-up is looking for innovators to launch a new diabetes care model:
Vayu Health is a California non-profit set to launch a completely different care model for people with diabetes living in under served communities, and is looking for like-minded people passionate about equity, person-centered care, and reducing barriers to accessing high-caliber diabetes care.
If you love working in an innovative team environment, are excited by participating in creative programming for patients, and are an independent thinker and self-starter, this just might be the perfect opportunity for you.
The Vayu Team is looking for a CDCES and LCSW
The team is made up of people that are excited about building something new, and every team member regardless of role has a voice in creating the company. Vayu believes passionately in reducing barriers to care for vulnerable populations, and has a strong focus on equity. The care team includes local community coaches, certified diabetes educators, licensed clinical social workers, and community clinic physicians. With this multidisciplinary team, care delivery will be a combination of coordinated, proactive in-person and virtual care, delivered when and where the patient needs it.
Vayu has the commitment of the community clinic and Medicaid healthcare plan, as well as national experts in diabetes care, Medicaid managed care healthcare payment reform, and chronic care system design and optimization.
CORE TEAM:
This is an incredible opportunity to join a dynamic mission-driven company with visionary leadership and a bold and inclusive culture. Interested people should directly contact Margie ([email protected] or 415-225-4787).
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 78, lives alone and manages their diabetes with bolus insulin at breakfast and dinner and basal insulin at night. For the past few months, JR has had trouble remembering to take insulin with meals and JR’s most recent A1c is above 9%.
Which of the following is most likely contributing to this change of behavior for JR?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our
We have updated this content based on the ADA 2021 Standards of Care.
We are living longer and more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering reduction of medication and insulin therapy intensity. The older population has unique issues and special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.