
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

A three-year long study showed real time continuous glucose monitoring (rtCGM) was associated with lower A1c levels in people with type 1 diabetes, whether the participants used pumps or multiple daily injections.
In the study, participants checked glucose levels using CGM or fingersticks four times per day.
Only the real time CGM group had improvements in time-in-range and reduced time below range, regardless of whether they used an insulin pump or injections.
Also, fewer participants using real time CGM experienced severe hypoglycemia.
This three-year study came from the Comparison of Different Treatment Modalities for Type 1 Diabetes Including Sensor-Augmented Insulin Regimens (COMISAIR). The group still advocates for individualization of treatment, but emphasizes what an important difference incorporating real time CGM makes.
Jan Soupal presented the study findings at the European Association for the Study of Diabetes 2019 Annual Meeting in the Czech Republic. Soupal noted that CGM can be coupled with multiple daily injections for those who prefer to only have one device on their body or worry about accessibility and affordability.
Read the full study details here.

Want more valuable CGM info for the test?
Check out our Technology Toolkit! Two fantastic courses included for a total of 3 CEs:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Adverse Childhood Experiences (ACE) such as neglect, abuse, household dysfunction, etc. have been found to have a profound impact on health and disease throughout life.
Here is the the link to the ACE Screening Tools and more information.
The higher the ACE Score, the higher the risk of diabetes, cardiovascular disease, mental health issues, earlier mortality and more.

Nadine Burke Harris, MD and California’s newly appointed Surgeon General, pushed for ACE scores to be more seriously considered and to increase routine screening, early detection, and early intervention.
Funding has been put forward to reimburse providers for screenings, and towards after school education and safety programs in preschool, early learning, and childcare.
Dr. Harris corrects the assumption that every person who scores positive for ACE needs mental health services: “most patients don’t” she says, and it’s important to know proper next-steps after a positive screening.
The best thing health care providers can do after a positive screening is to educate individuals on which symptoms could be related to a history of adversity, and give them tools they can use to manage and improve outcomes. These are tools like sleep, exercise, nutrition, mindfulness, mental health, and healthy relationships. Most of these tools don’t require a lot of extra resources as some health care professionals may fear.
Read Dr. Harris’ full interview on the Chronicle of Social Change.
For more info, here is the link to an excellent ACE Resource Page
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Our Diabetes Detective Team scans the diabetes news to discover the most relevant info that Diabetes Educators need in their daily practice. We post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Canagliflozin (Invokana), an SGLT-2 Inhibitor, just received a new Food and Drug Administration (FDA) indication.
Adults with type 2 diabetes and diabetes kidney disease who take canagliflozin (Invokana) experience a reduction of:

This new indication is based on the results of the CREDENCE Trial, which was designed to see if canagliflozin had a renal vascular protective effect.
The trial enrolled over 4, 400 people with type 2 diabetes and GFRs between 30 and 90. The results clearly indicated several benefits.
Researchers observed a 32% risk reduction of end stage renal disease among patients who took canagliflozin (HR = 0.68), as well as a 28% risk reduction for starting dialysis, having a kidney transplant or experiencing renal death.
In a sub-group of the CREDENCE Trial, cardiovascular death for type 2 diabetes dropped by over 30% and in the CANVAS Study, there was a 33% drop in risk of hospitalization for heart failure.
Please see Oral Meds Pocketcard for side effects and precautions of canagliflozin and SGLT-2 Medications. In the most recent ADA Standards, two SGLT-2 Inhibitors, empagliflozin and canagliflozin are indicated for individuals with heart failure, chronic kidney disease and an elevated CV risk profile.
The use of these SGLT-2 Inhibitors offer hope and a new strategy to protect renal function and decrease heart disease risk in those living with diabetes.
For more information see this Helio Article on the new FDA indication for Canagliflozin.
Please see our GLP-1 Receptor Agonists and Injectibles Pocketcard for new oral GLP-1 tablet.
Download FREE Medication PocketCards on our website.
Purchase PocketCards – Updated physical PocketCards will ship out no later than October 18, 2019.
Download our FREE CDCES Coach App
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]For Question of the week, test takers usually choose the correct answer 70-80% of the time. However, for this Tuesday’s question of the week, only about 23% of respondents chose the correct answer.
So, we thought this would be a perfect opportunity for another answer rationale. We’ll explore this question and the best answer in more detail and throw in some test-taking tips along the way.
Question of the week on October 8:
The American Diabetes Association recommends which of the following interventions to decrease risk of cardiovascular disease?
Answer Options:
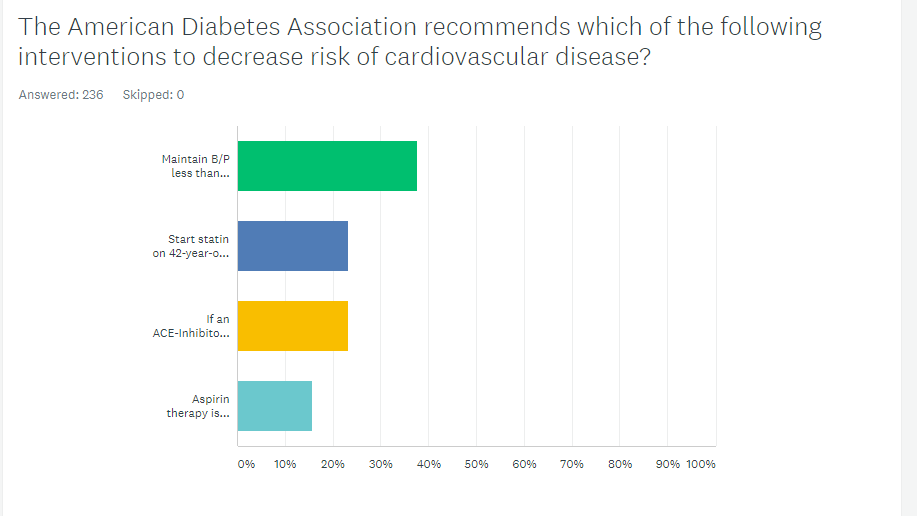
As shown above, the most common choice was option 1, the second most common answer was option 3, then option 2, and finally option 4.
For this question, a key consideration is what “The American Diabetes Association recommends.” This focus helps test takers hone in on ADA Standards.
Option 1 is juicy but incorrect. The ADA standard for individuals without cardiovascular disease risk or history is to maintain a B/P of less than 140/90. The blood pressure target in Option 1 of 130/80, is the B/P target for individuals with cardiovascular disease or a 10 year CVD risk of 15% or greater. The general goal for people with diabetes is to keep B/P less than 140/80. However, for those with a higher risk of CV events, the target is 130/80. Blood pressure targets are based on the individual assessment of risk.
Option 3 is incorrect because ACE-Inhibitor and Angiotensin Receptor Blockers should not be paired together. Option 3 says “add a Angiotensin Receptor Blocker” not switch to. Giving an ACE and and ARB together is not recommended due to potential renal issues.
Option 4 is incorrect because aspirin therapy is recommended for individuals over the age of 50 with CV risk factors.
Option 2 is the best answer. The standard for people with diabetes who are over the age of 40 is to start a statin to reduce the risk of cardiovascular disease. No CVD history is required to initiate statin therapy in this standard for people over the age of 40 with either type 1 or type 2.
For more info, here is a link to ADA’s Standard Ten. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2019
Our DiabetesEd Online University also offers courses on Standards of Care and Cardiovascular Disease. Check it out here!
We hope you appreciate this week’s rationale and keep studying hard! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Multiple studies have examined metformin for its potential tumor and cancer fighting ability. The National Center for Biotechnology Information (NCBI) published such a study in 2016. Researchers found substantial pre-clinical evidence suggesting anti-cancer properties of metformin based on in-vitro and in-vivo analysis. Their analysis suggested metformin could be used as a radiation sensitizer or immunotherapy drug, besides its direct anti-proliferative properties .
In mice with lung cancer, metformin was used and researchers saw a 72% reduction in tumor burden. Tumors are known to exhibit the Warburg effect, but metformin blunts this and consequently downregulates the growth of cancer stem cells.
Several observational studies showed a correlation between metformin use and lessened cancer incidence. The results demonstrated that metformin users have statistically significant reductions in liver, pancreatic, colorectal and breast cancers.
You can read more details on the study and enjoy their infographics and tables of data here.
Coach Beverly reports no conflict of interest for medication postings.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Our Diabetes Detective Team scans the diabetes news to discover the most relevant info that Diabetes Educators need in their daily practice. We post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The Journal of General Internal Medicine recently surveyed nearly 300 physicians, and the findings were alarming.
Their research suggests approximately 25% of all physicians misdiagnose people who have diabetes with prediabetes instead.
Additionally, the average provider didn’t know 33% of the risk factors for prediabetes, were unfamiliar with prevention or management of the condition, and generally under-screened for it.

Only 42% of the physicians knew the correct fasting A1c to diagnose prediabetes.
Researchers from John Hopkins University recommend providing physicians with better knowledge on diabetes prevention and for insurance to cover plans that help better diagnose and treat prediabetes.
The hope is these two strategies will help with more accurate screening and earlier intervention to avoid development and progression of type 2 which can lead to kidney failure, heart disease, or stroke. Read the full study and statistics here.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]