
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
This course integrates the ADA Standard of Care on elements of a comprehensive medical assessment (Standard 4) of the individual living with prediabetes, diabetes, or hyperglycemia. Through case studies and real-life situations, we discover often hidden causes of hyperglycemia and other complications, such as liver disease, sleep apnea, pancreatitis, autoimmune diseases, fractures, and more. We delve into therapy for complicated situations and discuss management strategies for other conditions associated with hyperglycemia such as Cystic Fibrosis, and Transplants. Join us for this unique and interesting approach to assessing and evaluating the hidden complications of diabetes.
Objectives:
This bundle is specifically designed for healthcare professionals who want to learn more about the ADA Standards of Diabetes Care for their clinical practice or for those who are studying for the BC-ADM or the CDCES certification exam.
Previously recorded
Upcoming Updates
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed test takers on calculating LR’s sensitivity factor. 76% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LR is a 30-year-old with type 1 diabetes. LS uses 25 units of basal insulin and 20 units of bolus insulin (about 6-7 units per meal) per day. Using the rule of 1700, what is LR’s insulin sensitivity factor?
Answer Choices:
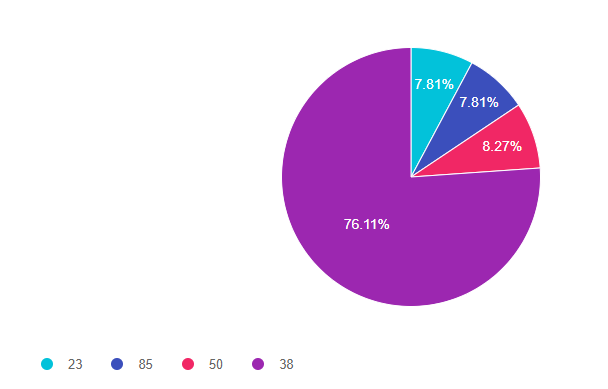
As shown above, the most common choice was option 4, the second most common answer was option 3, then a tie for options 1 and 2.
Answer 1 is incorrect. 7.81% chose this answer, “23.” To figure out the sensitivity factor, we first have to determine the Total Daily Dose (TDD) that LR is taking. LR is taking 25 units of basal insulin and 20 units of bolus insulin, which equals a TDD of 45 units. If we are using 1700 as our insulin sensitivity factor (ISF), we divide the 1700 divided by 45 or 1700/45 or 37.7 which we round up to 38. In other words, 1 unit of insulin will drop LR’s blood sugar by 38 points.
Answer 2 is incorrect. 7.81% of you chose this answer, “85.” People who chose this answer, probably only included the bolus insulin dose in the calculation or 1700/20. To get to the accurate answer, add the basal plus bolus to get the total dose of 45, the divide as follows 1700/45 equals or 37.7 which we round up to 38. In other words, 1 unit of insulin will drop LR’s blood sugar by 38 points.
Answer 3 is incorrect. 8.27% of respondents chose this answer, “50.” To figure out the sensitivity factor, we first have to determine the Total Daily Dose (TDD) that LR is taking. LR is taking 25 units of basal insulin and 20 units of bolus insulin, which equals a TDD of 45 units. If we are using 1700 as our insulin sensitivity factor (ISF), we divide the 1700 divided by 45 or 1700/45 or 37.7 which we round up to 38. In other words, 1 unit of insulin will drop LR’s blood sugar by 38 points.
Finally, Answer 4 is correct. 76.11% chose this answer, “38.” YES, most of you chose the BEST answer. To figure out the sensitivity factor, we first have to determine the Total Daily Dose (TDD) that LR is taking. LR is taking 25 units of basal insulin and 20 units of bolus insulin, which equals a TDD of 45 units. If we are using 1700 as our insulin sensitivity factor (ISF), we divide the 1700 divided by 45 or 1700/45 or 37.7 which we round up to 38. In other words, 1 unit of insulin will drop LR’s blood sugar by 38 points.
Extra Credit info. What sensitivity factor should we use?
We use 1700 or 1800 insulin sensitivity factor (ISF) for people on insulin analogs and the 1500 ISF for people on regular insulin. But also, as you can see with the math below, a higher ISF number means less insulin. So, if we are working with a leaner more frail individual, we might choose to be more conservative and start with and ISF of 1800.
Example- A person’s Total Daily Dose (TDD) is 30 units a day. To figure out how much correction insulin they need to correct their hyperglycemia, we would consider the following options depending on their presentation.
1800/30 = 1 unit for every 60 points above target
1700/30 = 1 unit for every 56
1500 / 30 = 1 unit for every 50
We hope you appreciate this week’s rationale!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Download Course Schedule | Download Course Flyer
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Diabetes medications are not just about glucose management anymore
In the past, to determine the right medication for an individual, the primary focus was placed on the glucose-lowering impact. However, with the introduction of the SGLT-2 Inhibitors and GLP-1 RA’s, there has been a tremendous leap forward and expansion of expectations for the co-benefits of diabetes medications.
The SGLT2s and GLP1’s, are both associated with weight loss without the fear of hypoglycemia. They decrease the risk of cardiovascular events and also offer renal protection. In addition, the SGLT-2s are so effective at treating heart failure (HF), that they are now being used for people with HF without diabetes.
Keeping close tabs on UACR and GFR
A big shift in determining the optimal diabetes treatment now includes thoughtful evaluation of Urinary Albumin Creatine Ratio (UACR) and GFR.
In the past, we collected UACR and GFR yearly to monitor kidney function. Now we use the results of these tests to determine not only kidney function but the risk of heart disease and the best therapy for diabetes, kidney health, and hypertension.
Now, more than ever, we are compelled to evaluate urinary labs to determine the albumin to creatinine ratio and keep a close eye on GFR to determine best practices to not only extend lifespan but improve healthspan.
For more info on UACR and GFR, see our blog post, “From Dipsticks to GFR – How to evaluate kidney function“.
Our updated Medication PocketCards reflect these shifts
In this latest version available for download and purchase, we have expanded and clarified the SGLT-2 considerations to reflect the changes in the 2022 ADA Standards of Care. We recognize that SGLT2 Inhibitors may be used as first-line therapy due to their additional benefits, “Along with metformin, SGLT-2s may be considered at first line diabetes therapy, especially for those with heart and kidney failure.” Since this class also slows the progression of chronic kidney disease, we also added, “for renal protection, use SGLT-2 Therapy if eGFR greater than or equal to 25 and UACR greater than or equal to 300.”
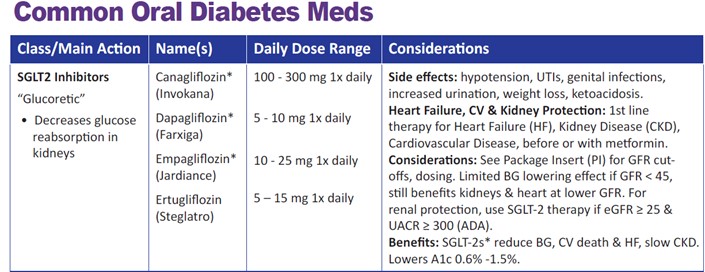
Since the GFR cut-offs for this med class are changing frequently, we removed the GFR guidelines for individual SGLT2’s and encourage users to review the package insert for the most recent recommendations.
Over the past twenty years, there has been tremendous expansion in the availability of diabetes medications that not only lower glucose but help decrease the progression of common diabetes co-comorbidities. In this evolving medication landscape, our Medication PocketCards capture the critical and current information you need for your clinical practice and certification exams.
Coach Beverly will highlight the key elements of the latest Medication Guidelines by AACE and ADA. We will explore clinical factors to consider when determining the best strategy to improve glucose management in people with type 2 diabetes and other co-conditions. There will be a special focus on cardiovascular risk reduction and renal protection.
Objectives:
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Download Course Schedule | Download Course Flyer
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Diabetes is associated with an increased risk of oral disease. Which of the following statements is true regarding people living with diabetes and hyperglycemia?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Schedule | Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
If you want to get fired up about providing Diabetes Self-Management Education and Support (DSMES), I highly recommend reading the updated Standards for DSMES. If you don’t have time to read the complete document, we have provided our top 9 takeaways to get you started.
This new version of the DSMES Standards, authored by a collaboration of education specialists, offers a fresh outlook and a simplified six standards with the clear goal of increasing inclusivity and breaking down barriers.
In addition, we explore the expanding clinical applications of the SGLT-2 Inhibitor class.
Clearly, the newer diabetes medications are impacting more than glucose levels, they can also boast about co-benefits including cardiovascular and renal protection. We have updated our Med Pocket Cards to reflect this new perspective and considerations.
Our last two articles take a look at the concerning findings of increased risk of future diabetes post-COVID-19 infection. Large, controlled trials are saying the same thing, about 25-40% of people one year after experiencing COVID-19 are being diagnosed with new type 2 diabetes.
Lastly, to celebrate EARTH DAY, we pause, take a deep breath and notice the wonderment and gift of our beautiful planet. Research shows that planet health improves human health and decreases chronic diseases. Maybe we can each start with one action toward caring for our planet. We provide some great getting started resources on growing native plants in your backyard, patio, or veranda. All of our actions matter.
Beverly, Bryanna, Jackson, and Amanda
Featured Articles
Upcoming Webinars
Featured Items
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Schedule | Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed test takers on which medications are needed. you all did great, since 81% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LS is 43 with type 2 diabetes, with an A1C of 8.8%, UACR is 32 mg/g, GFR is 48, and blood pressure is 146/84 or greater on 2 different occasions. Current medications include metformin 1000mg BID, lovastatin 20mg, glipizide 20mg.
Based on the ADA standards of care, in addition to lifestyle encouragement, adding which medications would most improve outcomes?
Answer Choices:
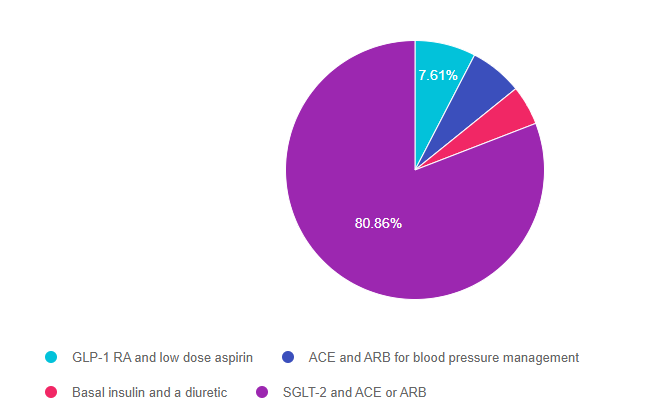
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and then finally option 3.
Answer 1 is incorrect. 7.61% chose this answer, “GLP-1 RA and low dose aspirin.” Since LS is under the age of 50 and their CV risk status isn’t revealed in this case study, we don’t have enough information to start LS on aspirin. We could consider adding a GLP-1 RA, since it is known to lower glucose, decrease CV risk and offer some renal protection. However, since one part of the answer is wrong, the whole answer is wrong, even though adding a GLP-1 to LS’s plan would be helpful.
Answer 2 is incorrect. 6.58% of you chose this answer, “ACE and ARB for blood pressure management.” LS does have hypertension and elevated albumin levels and is not taking any medication for blood pressure. Given those two risk factors, LS needs to take EITHER an ACE Inhibitor or ARB for blood pressure management, but NOT both. We would recommend starting LS on an ACE or ARB first and adjusting the dose based on home blood pressure reading. If LS needs an additional blood pressure medication, we could add a diuretic, calcium channel blocker or beta-blocker, or another agent. See our Hypertension & Lipids, Cheat Sheet for more info.
Answer 3 is incorrect. 4.94% of respondents chose this answer, “Basal insulin and a diuretic.” With an A1c of 8.8%, LS isn’t quite ready for insulin since there are 2 other medications we could try first (SGLT-2 or GLP-1) to get glucose to goal. The ADS Standards recommend trying a GLP-1 before basal insulin if possible to avoid the risk of hypoglycemia and to decrease weight gain. In addition, because LS has hypertension and albuminuria, a diuretic would not be the medication of choice to lower blood pressure. The preferred medications for blood pressure in the presence of albuminuria include either an ACE or ARB.
Finally, Answer 4 is correct. 80.86% chose this answer, “SGLT-2 and ACE or ARB.” GREAT JOB! Most of you chose this BEST answer. In the presence of hyperglycemia, albuminuria, and diminishing renal function, adding a SGLT-2 Inhibitor is the best choice based on ADA Standards. SGLT-2s have been shown to not only lower glucose and protect kidneys, they can also lower blood pressure due to their “glucoretic” properties. To manage LS’s hypertension, the preferred medications for blood pressure in the presence of albuminuria include either an ACE or ARB.
We hope you appreciate this week’s rationale! For more information on this topic, check out the ADA Standards of Care. Or, join our 3 day DiabetesEd Specialist Virtual Conference next week. It’s not to late to register!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Download Course Schedule | Download Course Flyer
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
If you want to get fired up about providing Diabetes Self Management and Education Support (DSMES), the newly updated Standards for DSMES is highly recommended reading. If you don’t have time to read the complete document, we have provided our top 9 takeaways to get you started.
Every 5 years, a committee of diabetes education specialists and advocates gets together to update this roadmap for the provision of DSMES. In the last version of this document, there were ten standards and lots of complicated rules and regulations required to set up a recognized DSMES Program.
In this new version, the collaborative of authors possesses a fresh outlook and clear vision that resulted in six simplified standards with the goal of inclusivity and breaking down barriers.
To address inequities, a candid discussion of racial disparities and social determinants of health is included. In addition, there is recognition that participation in DSMES has lost momentum during the pandemic with stagnant or decreasing enrollment. We need to innovate and make access and participation a top priority to make sure all people have the opportunity to benefit from this knowledge and life-saving information.
2. DSMES makes a difference! – Lowers A1c by at least 0.6% with greater A1c reductions when engaging in DSMES of 10 hours or more. In addition, DSMES has a positive effect on clinical, psychosocial, and behavioral aspects while improving quality of life and coping skills. Individuals who participate are more likely to engage in self-care through behavior change, including eating healthier eating and regular exercise.
3. Breaking down barriers through recognition of Social Determinants of Health and addressing equity. The authors recognize the need for person-centered services that embrace cultural differences, social determinants of health, and ever-increasing technological engagement platforms and systems. The goal is to increase health equity through access to this critical service while focusing more on person-centered care and decreasing administrative complexities.
4. Recognition of the need for a thoughtful community needs assessment that looks at more than demographics. We still need to gain data from local and national resources to identify race, ethnicity, cultural background, sex, age, geographic location, tech access, and literacy. But just as important are the perceptions of risk associated with diabetes and barriers including socioeconomics, cultural factors, misaligned schedules, and health insurance shortfalls.
5. An important and often underappreciated barrier to DSMES includes perceived lack of need and limited encouragement from health care professionals to engage in DSMES. Plus, special attention needs to be payed to those who do not usually attend clinic appointments to discover their perceived and real barriers.
6. Diabetes Care Community Coordinators are needed to help build bridges between the medical community and the community we serve. These individuals include community health workers and health promoters who live in the community and have familiarity and understanding of the needs and cultural factors of the individuals we are seeking to serve. Diabetes care coordinators also include; dietetic technicians, medical assistants, peer educators, and leaders. They can instruct, reinforce self-management skills, support behavior change, facilitate group discussion and provide social support.
7. Keep the curriculum dynamic and practical. Research endorses the inclusion of practical, problem-solving approaches, collaborative care, consideration of psychosocial issues, and support of behavior change strategies to sustain self-management efforts. In addition, supplementing with resources and support materials can help individuals navigate the health care system and promote self-advocacy.
8. Strategies to increase DSMES participation through provider referrals. Keeping programs vibrant and active is no easy task and requires constant attention. I put together a list of strategies I have used to boost referrals by providers. Direct mail of DSMES flyers to providers, networking during community gatherings, lunch and learn CE activities, hallway conversations, welcome packet for new providers, delivery of referral forms and holiday gifts to offices, and shared participant testimonials.
9. Strategies to increase DSMES participation through self-referrals. We can directly appeal to our community members and then reach out to their providers to approve the referral f. Ideas to touch your community include; publishing articles on hot diabetes topics, sending out press releases, advertising in local papers and on social media, hosting events during National Diabetes Month, joining health fairs, providing community presentations to service organizations, and promoting word of mouth marketing with your graduates.
Diabetes Self-Management Education and Support is a critical components of comprehensive diabetes care. By addressing barriers and including community members in our outreach, we can break down the walls and increase participation and improve the quality of life for all people.
This course provides you with a succinct overview of the latest standards for Diabetes Self-Management Education (DSME) and Support Programs. If you are taking certification exams or considering setting up a DSME program, this program is designed for you. We highlight the newly revised and simplified 2022 Standards and provide strategies on program implementation. In addition, we discuss Medicare Reimbursement and covered benefits. This course provides insights into the exam philosophy and also highlights critical content areas.
Objectives:
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Download Course Schedule | Download Course Flyer
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LR is a 30-year-old with type 1 diabetes. LS uses 25 units of basal insulin and 20 units of bolus insulin (about 6-7 units per meal) per day. Using the rule of 1700, what is LR’s insulin sensitivity factor?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Schedule | Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.