
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on the new ADA Standards for type 2 diabetes medication. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Based on the newly released 2024 American Diabetes Association (ADA) Standards of Care, which of the following statements is NOT accurate regarding treatment for hyperglycemia?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
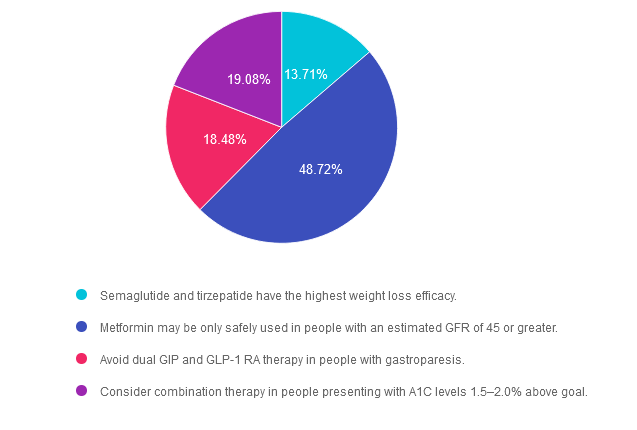
Answer 1 is incorrect. 13.71% chose this answer. “Semaglutide and tirzepatide have the highest weight loss efficacy.” This statement is accurate. These two incretin mimetics not only substantially lower A1C levels, they also are associated with the highest percentage of weight loss of all the diabetes medications. See Diabetes Med PocketCards for more information.
Answer 2 is correct. 48.72% of you chose this answer. “Metformin may be only safely used in people with an estimated GFR of 45 or greater.” YES, great job! This answer is FALSE (making it the best answer). If a person with diabetes is taking metformin and their GFR drops below 30, then we stop the medication. However, we can start or continue metformin therapy if the GFR is 45 or greater. In addition, metformin doesn’t harm the kidneys, it actually protects them by lowering blood glucose levels. See Diabetes Med PocketCards for more information.
Answer 3 is incorrect. About 18.48% of respondents chose this. “Avoid dual GIP and GLP-1 RA therapy in people with gastroparesis.” This answer is also accurate. Tirzepatide (Mounjaro) can substantially slow gastric emptying which could exacerbate gastroparesis. For that reason, it is not a recommended therapy for people with gastroparesis.
Finally, Answer 4 is incorrect. 19.08% chose this answer. “Consider combination therapy in people presenting with A1C levels 1.5–2.0% above goal.” This answer is also accurate. The ADA Standards of Care recommend more intensive pharmacologic intervention for those with substantially elevated A1C to improve and prolong pancreatic function.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Topics:
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Which of the following is an accurate new 2024 ADA Standard of Care?
The new ADA 2024 Standards of Care include dozens of updates to diabetes clinical practice. Which of the following statements has actually been added to the ADA 2024 Standards of Care?
Click Here to Test your Knowledge
Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with diabetes and preparing for the CDCES Certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
MR is frustrated that their morning glucose is almost always elevated. Since you have heard about the impact of “chronotype” on glucose, you ask them about eating patterns and explore whether they are early birds or night owls.
The 2024 American Diabetes Association (ADA) Standards of Care introduced the field of chrononutrition, the science of how our body’s 24-hour cycle (circadian rhythm), nutrition, and health interact. Growing evidence shows that factors, including when and type of food is eaten, hormones, genetics, exercise, sleep cycles, and a person’s daily light exposure, influence health and risk for metabolic disease.

When we consider a person’s chronotype, we realize that it’s not just “what” individuals eat that impacts metabolic health. Could “when” they eat and their chronotype be just as crucial for glucose regulation? Can we leverage this information to suggest modifications in the type of nutrients consumed throughout the day to support improved glycemia?
We have learned the association between circadian rhythm disruptions and metabolic disorders from people who perform shift work. Working in shift work and having type 2 diabetes is associated with increased A1c, neuropathy, and decreased psychological well-being.1 Glucose metabolism and tolerance follow a circadian rhythm throughout the day. Hormones, such as insulin and cortisol, cycle daily and regulate insulin sensitivity and glucose metabolism changes. Research suggests when food intake is out of sync with the daily cycle, this can reduce glucose tolerance and increase the risk of metabolic diseases such as type 2 diabetes, obesity, and cardiovascular disease.
“Meal timing and food nutrient components (chrononutrition) play an important role in regulating the circadian clock, enhancing metabolic health, and reducing the risk of type 2 diabetes.” 2
Post-prandial glucose response is affected by what and how much we eat and can vary based on the time of day the meal is consumed. Meal timing can affect type 2 diabetes, so it is important to consider timing in addition to composition alone. In a 2020 review article by Henry et al., they reported several different studies completed in individuals with type 2 diabetes and healthy subjects. These studies suggested both morning and late-night eating can contribute to the greatest glucose excursions. Eating after 8 pm was independently associated with an increase in A1C levels. Consuming more than a third of daily calories late in the evening led to higher post-meal glucose excursions and reduced morning glucose tolerance compared to other times of day. And a study of individuals with type 2 diabetes showed higher post-meal glucose trends after morning meals verses identical meals consumed throughout the day. These small studies suggest that modifying when a meal is consumed could reduce glycemia and the risk of diabetes. However, more extensive studies are needed to support causation and associate it with a person’s genetics and true chronotype.
Macronutrient meal composition and the time of day consumed may also play a role in chrononutrition. Whether it is a variation of calories consumed or manipulating different macronutrients from meal to meal, the relationship between food type and timing could affect glucose metabolism. Changes in insulin sensitivity throughout the day can affect post-meal glucose in response to varying carbohydrate quantity, quality, and rate of digestion. Davis et. Al, 2019 found that increased protein and lower carbohydrates at dinner meals reduce night post-prandial glucose compared to standard meals.
The key nutrition recommendations from the 2024 ADA Standards of Care are focused on individualizing eating patterns, meal plans, and dietary approaches. Research continues to evolve in this field, and there is much more to understand and validate. Most of the articles regarding chrononutrition referenced in the ADA Standards of Care are specific for type 2 diabetes, but we know circadian cycles and metabolism also play a role in type 1 diabetes. More research is needed to improve our understanding of why nutrients consumed at different times of day have differing effects, how this relates to the individual’s circadian biomarkers and genetics, and how it interplays with psychological factors that drive sleep cycles.
There is much to learn, but are there practical approaches we could consider implementing now? Yes! We can start by:
Blog contributed by nutrition expert Christine Craig, MS, RDN, CDCES
References:
Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
For last week’s practice question, we quizzed participants on what is the best approach for people with low literacy skills. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
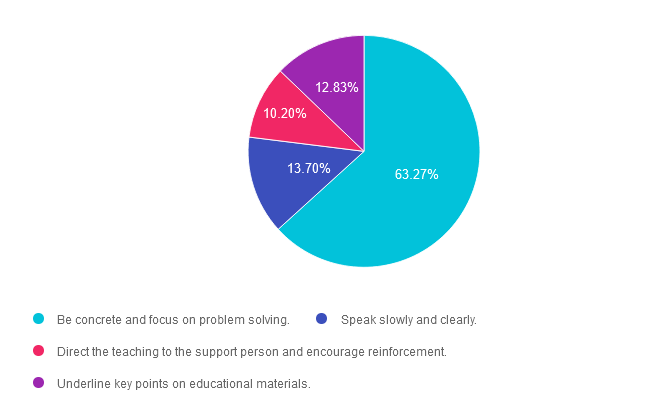
Question: Which of the following strategies is most effective when working with someone with low literacy skills?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is correct. 63.27% chose this answer. “Be concrete and focus on problem solving.” Yes, this is the best answer. Since a person with low literacy can’t take notes or read information later, they will need to commit new information to memory. By providing concrete examples and engaging in collaborative problem solving, a person with low literacy can more effectively retain the information.
Answer 2 is incorrect. 13.70% of you chose this answer. “Speak slowly and clearly.” Just because a person hast low literacy doesn’t mean they have an intellectual disability. Maybe they didn’t have a chance to complete their education or experienced some other impediment to learning how to read and write. We can use a usual conversational pace and annunciation with this individual.
Answer 3 is incorrect. About 10.20% of respondents chose this. “Direct the teaching to the support person and encourage reinforcement.” A general rule of effective communication is to direct the teaching and education to the person with diabetes, while including the support person.
Finally, Answer 4 is incorrect. 12.83% chose this answer. “Underline key points on educational materials.” Since people with low literacy have limited ability to read and write, using print materials with words would not be an effective method to provide education. Use of pictures and infographics, videos, podcasts or other educational strategies that don’t require literacy, would be excellent alternatives.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Topics:
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

We had such a great time celebrating 25 years with all of you.
The first highlight of the year was connecting with colleagues at ADCES in Houston. It was like attending a family reunion with thousands of like-minded individuals. So many enthusiastic colleagues stopped me mid-stride to share the news of passing their CDCES or BC-ADM after attending our courses. Many hugs were shared, and there were plenty of tears of joy, too! As a diabetes education veteran, it was a special honor to present one of my passion topics, Revitalizing Your Diabetes Program. As part of my legacy education topics, this presentation is culled from my 30 years of working in the field and braving new approaches, sometimes failing but always moving forward with a clear focus on improving the care received by people with diabetes. Nothing is like the profound connection made with others in a shared community.
We also celebrated our 25th company anniversary for the entire year. Activities included lots of free webinars, new swag, and great sales.

I started Diabetes Education Services in May of 1998, just after the World Wide Web was introduced, and sending messages through something called “email” was possible. At first, my one-person company only offered live courses at hospitals and meeting sites nationwide. My administrative space consisted of a 10×12 foot room in our home, where I juggled writing my monthly newsletter and updating slides while raising two busy toddlers. In 2010, I took a leap of faith and decided to try offering courses online.
Fast forward to today. Our business has grown to include a fantastic team and a newsletter reaching over 40,000 online subscribers. Our Online University includes over 50 CE courses that we update yearly, plus we offer a CDCES Coach app, blogs, an 8-sided PocketCard, keynote presentations, and more. This year, we held our three day DiabetesEd Course in San Diego and celebrated with a beautiful ocean view, special friends and delicious carrot cake topped with a 25 year candle.
Family celebrations.

My husband and I became empty nesters this year. Our oldest son is a senior at SMU and will graduate with his finance degree in May. Our youngest son is kicking off his chemistry degree at UC Berkeley. I miss the daily bustle and commotion of having my boys around, but I am overjoyed that they have found their place in this world and are boldly moving into adulthood. Of course, I can’t wait till they come home for the holidays so we can play cards, tell stories, and hang out together.
We also celebrated 25 years of marriage. My husband, Kristapor, continues his work as a critical care pharmacist at our local community hospital saving lives and advocating for best care at every turn. At the risk of sounding corny, my husband has been the wind beneath my wings. Having him as my partner throughout this life journey has given me a foundation of trust and love to take risks and live my dream. I am forever grateful that I commented on his cute tie when we worked together at Stanford hospital in 1996. The rest is history.
The truth is, we couldn’t have done any of this without all of YOU, our community.
I am forever grateful for your willingness to support and believe in a young Diabetes Specialist who had the vision to create a company that uplifted people with diabetes through a blend of science and compassion.
Thanks to our dedicated community of diabetes educators and advocates for celebrating our 25th Anniversary with us. Stay tuned. We can’t wait to see what the future holds!
This series is designed for healthcare professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
See Full Free Resource Catalog
AR is 15 years old and uses an automated insulin delivery (AID) system to manage their diabetes.
They tell you they feel so guilty about all the food and sweets they ate during the holidays and have been trying to get back on track. What is the best response?
Click Here to Test your Knowledge
Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with diabetes and preparing for the CDCES Certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
You are invited to join our upcoming FREE Webinars!
This year was an exciting one at the Cat Bakery, filled with lots of love, joy, and a bit of magic.
Last year I shared our newest addition to the Cat Bakery, Muffin, and the sibling rivalry with her new sister, Biscuit.
I am happy to report their relationship has grown immensely over the past year and while they still fight like sisters do, they have shared many sweet moments taking naps or playing with each other.
This year we sent family holiday cards for Halloween and will be sending more for the winter holidays to our loved ones.
Since we love all of you, we wanted to share these pictures with you of our holiday photoshoots.



Sending lots of love this Holiday Season!
Biscuit, Muffin & Bryanna (Director of Operations & Customer Happiness)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.