
For last week’s practice question, we quizzed participants on Lifestyle Therapy for MASLD and MASH. 83% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

PJ has had type 2 diabetes for 8 years and is here for a follow-up visit. Labs indicate A1c at 7.2%, lipids at target, eGFR of 78 mL/min/1.73m², and urine albumin-to-creatinine ratio (UACR) of 65 mg/dL. Blood pressure at the office visit today was 142/86, which is consistent with home monitored values. PJ confirms taking medications, metformin and simvastatin. PJ inquires about recently completed lab work.
According to the ADA Standards of Care, what would be an appropriate next step in the diabetes care plan?
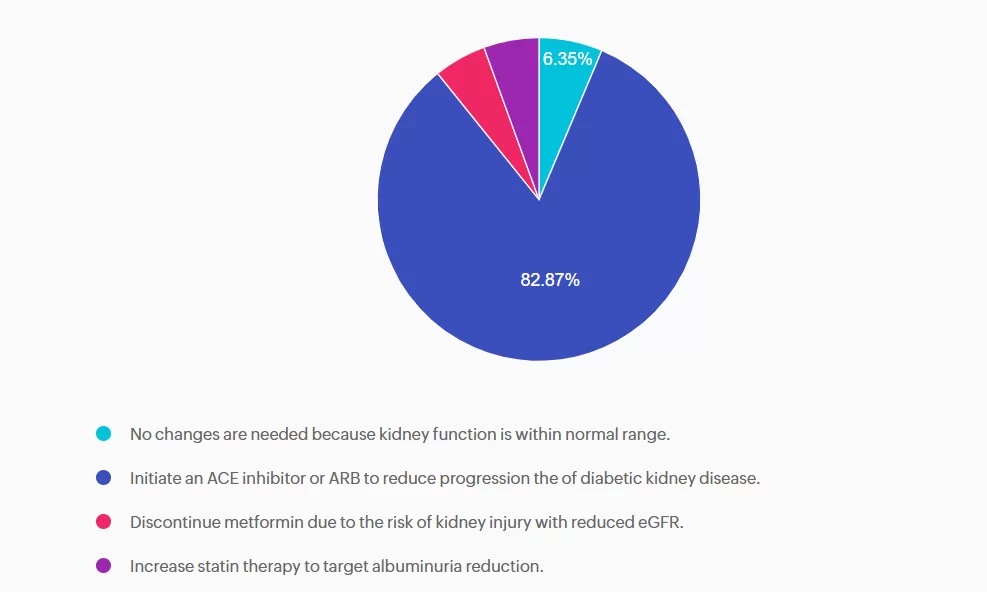
- No changes are needed because kidney function is within normal range.
- Initiate an ACE inhibitor or ARB to reduce progression the of diabetic kidney disease.
- Discontinue metformin due to the risk of kidney injury with reduced eGFR.
- Increase statin therapy to target albuminuria reduction.
Getting to the Best Answer
Answer A is incorrect: 6.35% chose this answer, “No changes are needed because kidney function is within normal range.” A is incorrect. Although eGFR indicates stage 2 kidney disease, the elevated UACR, ≥30 mg/g, confirms moderately increased risk and recommendation to treat. Additionally, PJ’s blood pressure is also above the target. Intervention is needed to protect kidney and cardiovascular health.
Answer B is correct: 83% chose this answer, “Initiate an ACE inhibitor or ARB to reduce progression the of diabetic kidney disease.” PJ has a mildly decreased eGFR, but UACR is elevated above 30 mg/g, indicating a recommendation to treat. Additionally, intervention is needed to optimize blood pressure. According to the ADA Standards of Care in Diabetes, individuals with diabetes, hypertension, and moderately increased albuminuria should be treated with an ACE inhibitor or angiotensin receptor blocker. The use of sodium-glucose cotransporter 2 (SGLT2) inhibitors or glucagon-like peptide 1 agonists (GLP1-RA), with demonstrated benefits, could also be considered to reduce CKD progression.
Answer C is incorrect: 5.25% chose this answer, “Discontinue metformin due to the risk of kidney injury with reduced eGFR.” Metformin is safe to continue unless eGFR falls below 30 30 mL/min/1.73m². PJ’s kidney function is adequate for continued use. However, consideration to add a change to SGLT2 or GLP1 with kidney benefit could also promote additional A1c reduction.
Answer D is incorrect: 5.52% chose this answer, “Increase statin therapy to target albuminuria reduction.” Statins are recommended for ASCVD prevention, but they do not reduce albuminuria. Lipids are within normal range, and albuminuria should be addressed with an ACE inhibitor/ARB or potentially a SGLT2 inhibitor or GLP-1 RA.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Enroll in our FREE Webinar
From the Gut to the Butt – Exploring the GI System

Explore the magnificent world of diabetes and the gut — from periodontal disease to the microbiome and everything in between.
Join Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM, for a fascinating journey through gastrointestinal health from top to bottom. This course covers fatty liver disease, gastroparesis, intestinal complications of diabetes, the gut microbiome, and more — giving you the knowledge to better support whole-body health.