Standards of Care Section 8 – Approaches to Glycemic Treatment
Standards of Care Section 8 – Approaches to Glycemic Treatment
Insulin Therapy for Type 1
This updated version of Meds Management includes more detailed information on insulin therapy for Type 1s. They note that sensor-augmented insulin pump therapy with the threshold suspend feature reduced nocturnal hypoglycemia without increasing A1c (for type 1s in a 3 month randomized trial). The FDA approved the first hybrid closed-loop pump system, since the literature supports its safety and efficacy.
Investigational Agents for Type 1s
- Add on Metformin for Type 1 – In several trials, adding metformin to insulin for type 1s, reduced insulin requirements 6.6 units a day and led to small reductions in weight and LDL cholesterol. However, it did not significantly reduce A1c. Metformin in not FDA Approved for use in patients with type 1 diabetes.
- SGLT-2 Inhibitors – these “glucoretics” lower glucose by decreasing renal reabsorption of glucose in the proximal tubules. Since this class works independent of endogenous insulin, SGLT-2 Inhibitors may benefit patients with type 1 or type 2 (not FDA Approved for use in patients with type 1 diabetes). However, the FDA has issued a warning of the risk of ketoacidosis occurring in the absence of significant hyperglycemia. There are many reported cases of euglycemic ketoacidosis in patients with type 1 or type 2 diabetes. If patients are experiencing signs of ketosis, instruct them to immediately stop taking the SGLT-2 and seek immediate care.
Type 2 Management Strategies – Stepwise Approach to Pharmacologic Management of Type 2 Diabetes – 2018
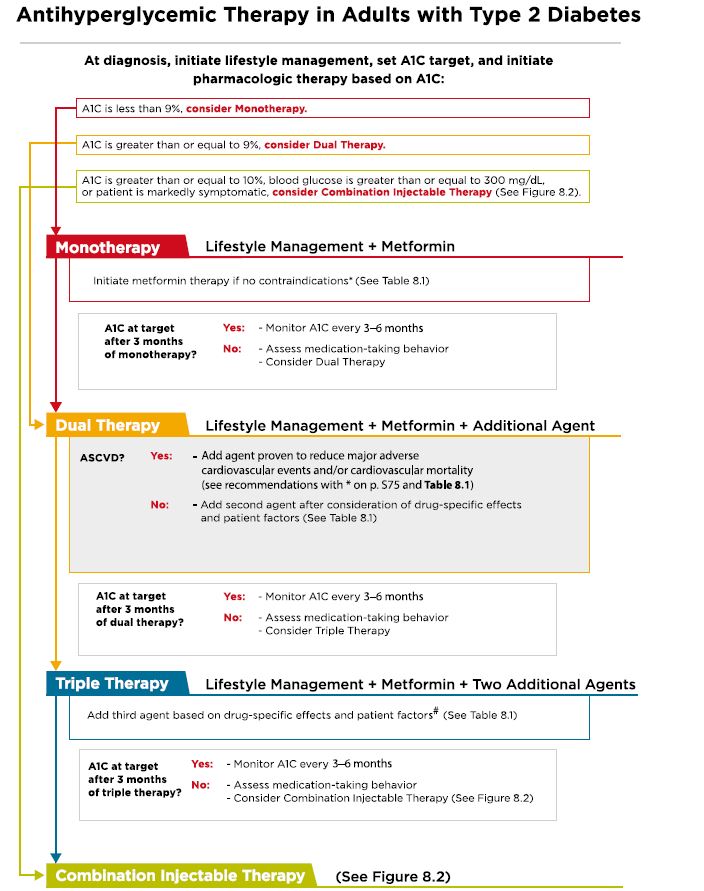 Pharmacologic Approaches to Glycemic Treatment 2018. This hyperglycemia road map details strategies to achieve glucose control for both Type 1 and Type 2 Diabetes. Section 8 of Standards of Care, Dec 2018.
Pharmacologic Approaches to Glycemic Treatment 2018. This hyperglycemia road map details strategies to achieve glucose control for both Type 1 and Type 2 Diabetes. Section 8 of Standards of Care, Dec 2018.
Step 1
According to the ADA 2018 Standards, section 8, Metformin therapy should be started along with lifestyle Management at diagnosis of type 2 Diabetes (unless contraindicated). Metformin is effective, safe, inexpensive and may reduce risk of CV events and death.
Step 2
If A1c target is not achieved after 3 months, consider metformin and any one of the six preferred treatment options based on drug specific effects and patient factors.
If A1c target is still not achieved after 3 months on metformin, and the patient has CV Disease, consider adding a second agent with evidence of cardiovascular risk reduction (based on drug specific effects and patient factors).
These include:
- SGLT-2 Inhibitors – empalgliflozin (Jardiance) and canagliflozin (Invokana)
- GLP-1 Receptor Agonist – liraglutide (Victoza)
Step 3
If A1c target is still not achieved after 3 months, combine metformin plus two other agents for a three-drug combination.
Step 4
If A1c target is still not achieved after 3 months, add combination injectable therapy to the three-drug combination.
For all steps, consider including medications with evidence of CV risk reduction, based on drug specific effects and patient factors.
Medication Therapy Based on A1c
- If A1c is less than 9%, consider monotherapy
- If A1c is greater than or equal to 9% consider dual therapy
- If A1c is greater or equal to 10%, or if BG 300 or more, or pt is markedly symptomatic, consider insulin and injectable therapy.
Want to learn more about this topic?
- Join our Standards of Care Webinar – Jan 19, 2018
- Download our FREE Medication PocketCards
- Join our Meds Update Webinar – Feb 19, 2018
- Download CDCES Coach App – FREE