

I felt pretty discouraged reading through the New England Journal of Medicine (NEJM) summary of the state of diabetes treatment and control in the U.S. from 1999-2018. We have stalled in improving diabetes outcomes in spite of exciting new therapies and dazzling technologies.
Based on this “Diabetes Report Card” for the U.S it seems pretty clear that changes in our care delivery system are urgently needed. First, let me share the data, then we consider how Diabetes Care Specialists (you and me) can drive the improvement arrow in the right direction.
The data summarized below is extracted from the National Health and Nutrition Examination Survey (NHANES) which assesses national trends in diabetes care and outcomes for the past decade.
Summary of the major findings of the Diabetes ABC’s. A1C, Blood Pressure and Cholesterol.
Data is compared from the 2007 -2010 period to the 2015-2018 time period.
Reaching A1c Target of less than 7%?
- The percentage of people with diabetes and an A1c of less than 7%, declined from:
- 57.4% in 2007-2010 to
- 50.5% in 2015 to 2018
Coach Bev’s Report Card Comment: Blood glucose levels trended up. GRADE C-
Reaching LDL target of less than 130 mg/dL?
- The percentage of people with diabetes and an LDL of less than 130 leveled off, with slight movement in the right direction.
- 52.3% in 2007-2010 to
- 55.7% in 2015 to 2018
Coach Bev’s Report Card Comment: Lipid levels improved slightly. GRADE B-
Reaching blood pressure goal of less than 140/90 mm Hg?
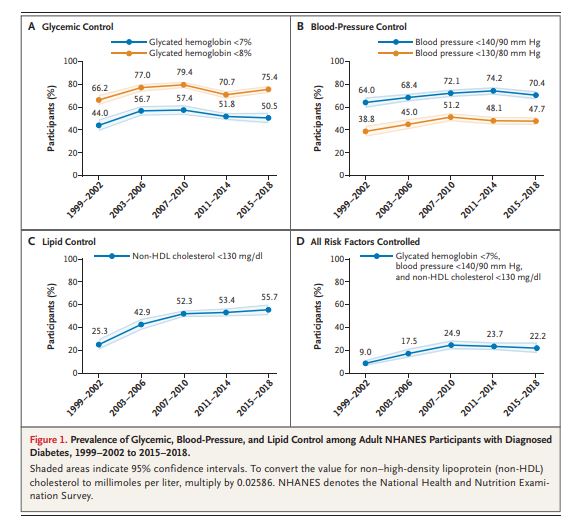
- The percentage of people with diabetes and blood pressure below the target of 140/90 worsened.
- 74.2% in 2007-2010 to
- 70.4% in 2015 to 2018
Coach Bev’s Report Card Comment: Blood pressure control achievement dropped slightly. GRADE C-
The percent of participants who achieved all 3 targets of A1C, BP, and lipids?
- The percentage of people who reached all 3 targets declined slightly.
- 24.9 % in 2007-2010 to
- 22.2% in 2015 to 2018
Coach Bev’s Report Card Comment: ABC’s of diabetes control dropped slightly. GRADE C-
Data and Graph from Trends in Diabetes Treatment and Control in U.S. Adults, 1999–2018 | NEJM
What are the barriers and how can Diabetes Care and Education Specialists help improve the grade?
The year 1999 got off to a good start with improved diabetes control but stalled and declined as the decade moved forward. There are several possible reasons as cited by the authors.
Sluggish initiation of first-line therapies. In 2015–2018, only 56.3% of adults with diabetes were using statins, 59.5% were using metformin, and 60.3% were using an ACE inhibitor or ARB.
These results are consistent with those of previous studies and point to clinical inertia as a potential culprit.
In addition, achieving glycemic and blood-pressure control often entails the use of multiple agents. However, the study found that only 60.6% of participants with an A1C level of 7% or higher and 52.8% of those with a blood pressure of 140/90 mm Hg or higher were treated with more than one glucose-lowering or blood-pressure-lowering medication, respectively.
Coach Beverly suggested action: Diabetes Care and Education Specialists can continue to raise awareness of the ADA Standards of Care for Diabetes and advocate for initiating first-line and add-on therapies in their work settings. Plus, we can encourage a streamlined referral process to facilitate participant access to DSMES and to RD/RDN for initial and ongoing lifestyle and nutrition counseling.
Care Gaps for Young People, Ethnic Groups and Uninsured Populations
The study found that younger people, Mexican Americans, and persons without health insurance were more likely to be untreated when risk-factor targets were not achieved. These gaps are especially magnified in under-resourced areas.
In addition, given that the rates of diabetes-related complications are higher in people of color and uninsured populations and that type 2 diabetes discovered in young adulthood have a more aggressive clinical course than diabetes, immediate action is required to improve outcomes.
Coach Beverly suggested action: Diabetes Care and Education Specialists continue to take a leadership role in intentional and unrelenting outreach to provide DSMES and MNT to under-resourced communities using novel and evidenced-based approaches. Since prediabetes rates are also higher in many of these communities, establishing easily accessed Diabetes Prevention Programs and networking with community health workers and leaders can contribute to improved health outcomes.
Medications are too expensive for many people
Even though we have a slew of new and highly effective classes of diabetes medications, they are out of the financial reach for many. As patents expire and the medications are available as generics, access and affordability will increase. In the meantime, a realistic approach to providing affordable diabetes treatment is needed.
Coach Beverly suggested action:
Diabetes Care and Education Specialists can help craft a medication plan that is realistic and affordable. For people with no insurance or large co-pays, consider using available generic diabetes medications. These medications often cost $10 or less for a 3-month prescription. They include: metformin, sulfonylureas, and pioglitazone. In addition, Walmart offers Reli-On insulins including Regular, NPH, and 70/30 insulin for $25 a vial. There are also online resources like GoodRx.com that help people find discounts on their usual medications and the different pharmaceutical companies also offer discount programs based on need.
See Insulin Cost Savings Guide for an abundance of resources and useful links.
In conclusion, Diabetes Care and Specialists are perfectly positioned to influence health delivery systems and advocate for best clinical practices. We can be catalysts for establishing DPP and DSMES programs in under-resourced communities and advocate for access to affordable medications and technologies to help participants reach their targets for A1C, Blood Pressure, and Cholesterol while improving quality of life.
With a concentrated effort, maybe our next report card will be a little bit better!
With hope, Coach Beverly
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.