

We quizzed test takers on hyperglycemic crisis. 61% of respondents, chose the best answer. We want to share this important info so you can pass it on to people living with diabetes and your colleagues and prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: People with type 1 or type 2 diabetes can experience hyperglycemic crises.
Which of the following is true about Diabetes Ketoacidosis (DKA)?
Answer Choices:
- People with Latent Autoimmune Diabetes (LADA) are not at risk of DKA.
- DKA is associated with hyperkalemia and elevated pH.
- DKA can be managed with IV or Sub-Q insulin therapy.
- People with type 1 on SGLT-2s have lower risk of DKA than those with type 2.
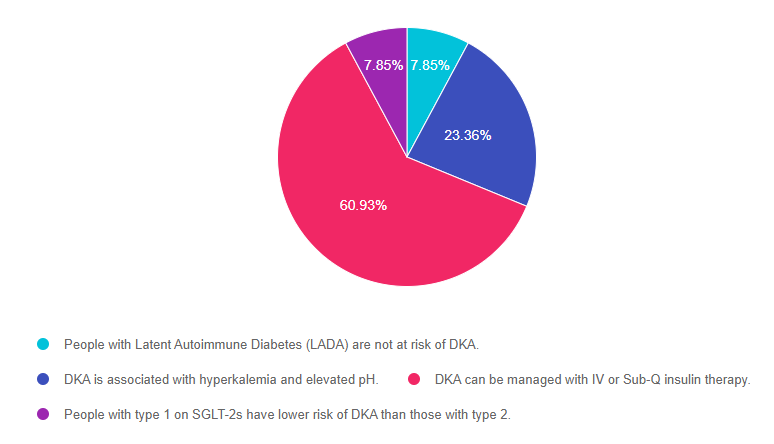
As shown above, the most common choice was option 3, the second most common answer was option 2, then a tie for option 1 and option 4.
Getting to the Best Answer
Answer 1 is incorrect. 7.85% chose this answer, “People with Latent Autoimmune Diabetes (LADA) are not at risk of DKA.” Any person with a substantial insulin deficiency (including type 1, type 2 and people with LADA) are at risk of ketoacidosis. The risk increases during periods of illness, inadequate calorie intake or when an individual is not injecting adequate insulin. Most individuals with LADA need insulin within 6 months of diagnosis to maintain glucose levels. Without insulin injections, people with LADA can’t use glucose for fuel and will start burning fat for energy, which leads to excess circulating ketones and potentially DKA.
Answer 2 is incorrect. 23.36% of you chose this answer, “DKA is associated with hyperkalemia and elevated pH.” Part of this answer is correct, which makes it a juicy answer. This common test taking pitfall is easy to fall into. It is true that people in DKA can become hyperkalemic, but they also always experience acidosis, which causes the pH to fall, not elevate.
Answer 3 is correct. 60.93% of respondents chose this answer, “DKA can be managed with IV or Sub-Q insulin therapy.” Yes, GREAT job, this is the BEST answer. Mild or moderate DKA can be treated using SubQ insulin and all levels of DKA can be treated with IV insulin. The treatment choice is based on health care setting, provider preference, and the patient’s presentation.
Finally, Answer 4 is incorrect. 7.85% chose this answer, “People with type 1 on SGLT-2s have lower risk of DKA than those with type 2.” Some people living with Type 1 may be started on an SGLT-2 (which is OFF-LABEL) by their provider to help with glucose management and lower insulin needs. People with type 2 diabetes, may also be started on an SLGT-2. Both groups are at increased risk for experiencing DKA on a SGLT-2. However, the person with type 1 is at HIGHER risk of experiencing DKA, because they have an absolute insulin deficiency and if they reduce their insulin dose too much, they might need to convert from using glucose for fuel to fat for fuel, leading to DKA.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this important learning activity!
Want to learn more? Join our Webinar on Hyperglycemic Crisis, which is ready for viewing!
Want to learn more about this topic?
Level 2 | Hyperglycemic Crises, DKA & HHS Standards | 1.0 CE
Annual Webinar Recorded on December 15th
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications and insulin deprivation. The difference and similarities between Diabetes Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Objectives:
- Common causes of hyperglycemic crises.
- The difference and similarities between DKA and HHS and treatment strategies
- Causes and treatment of hyperglycemic crises.
Intended Audience: A great course for healthcare professionals in the field of diabetes education looking for a straightforward explanation of identification and treatment of hyperglycemic crises.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
Enroll in our entire Level 2 – Standards of Care to join us for the below Annual Live Webinar Updates. All courses air at 11:30 a.m. (PST)
- December 15, 2021 – Hyperglycemic Crises, DKA & HHS Standards | 1.0 CE
- December 21, 2021 – Assessing and Promoting Well-Being: From Population Health to a Person-Centered Approach Standards | 1.5 CEs
- February 3, 2022 – ADA Standards of Care | 2.0 CEs
- March 24, 2022 – Meds Management for Type 2 – 1.5 CEs
- March 29, 2022 – Lower Extremity Assessment 1.5 CEs
- April 26, 2022 – Microvascular Complications, Eye, Kidney Nerve Disease 1.5 CEs
- April 28, 2022 – Critical Assessment of Diabetes Patient 2.0 CEs
- May 10, 2022 – Cardiovascular Disease and Diabetes Standards 1.5 CEs
- May 12, 2022 – Older Adults and DIabetes 1.5 CEs
- May 17, 2022 – Tots to Teens – Diabetes Standards 1.5 CEs
- May 19, 2022 – Pregnancy and Diabetes 1.5 CEs
- May 26, 2022 – Hospital and Hyperglycemia 1.5 CEs
- July 21, 2022 – Setting up a Successful Diabetes Program 1.5 CEs
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.