

For last week’s practice question, we quizzed test takers on the right amount of insulin for an 83 year old. Only 50% of respondents chose the best answer, which indicates that there was some confusion. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
MS is an 83-year-old admitted to the hospital for a broken hip. MS has a BMI of 22.4, A1C of 6.9% on metformin 500mg twice daily. UACR is less than 30 and GFR is 48. The MD writes to stop oral meds in prep for surgery and start on basal-bolus insulin therapy.
Based on MS’s profile, what would be the most accurate formula to calculate their total daily insulin dose?
Answer Choices:
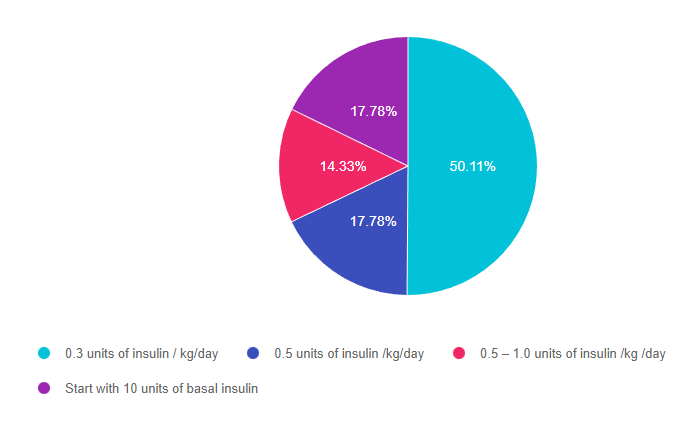
- 0.3 units of insulin / kg/day
- 0.5 units of insulin /kg/day
- 0.5 – 1.0 units of insulin /kg /day
- Start with 10 units of basal insulin
Getting to the Best Answer
Answer 1 is correct. 50.11% chose this answer, 0.3 units of insulin / kg/day.” YES, GREAT JOB. This is the best answer for several reasons. We can tell from the case study that MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting on a VERY conservative total daily insulin dose is the best and safest approach.
Answer 2 is incorrect. 17.78% of you chose this answer, “0.5 units of insulin /kg/day.” This is a juicy answer However MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting MS on 0.5 units/kg total daily insulin might be too much and might put MS at risk of hypoglycemia due to over insulinization.
Answer 3 is incorrect. 14.33% of respondents chose this answer, “0.5 – 1.0 units of insulin /kg /day.” This is another juicy answer However MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting MS on 0.5 – 1.0 units/kg total daily insulin might be too much and might put MS at risk of hypoglycemia due to over insulinization.
Finally, Answer 4 is incorrect. 17.78 chose this answer, “Start with 10 units of basal insulin.” This answer is appealing, since we often start people on 10 units of basal insulin. However, in this case study, we don’t have MS’s body weight to calculate their total daily insulin needs. Since we don’t have their weight in kgs, we don’t know what the right starting basal dose. For this reason, this is not the best answer.
Want to learn more about this question? Join us for our
Level 4 | Basal Bolus Therapy in Hospitals | 1.5 CEs
Recently updated and ready to watch!

Glucose control in the hospital matters! This course provides participants with a step-by-step approach to safely and effectively implement Basal Bolus Insulin Therapy in the inpatient setting. We discuss appropriate insulin dosing based on the patient’s clinical presentation and apply dosing strategies to a variety of case studies. Included are hard-to-manage situations that commonly occur in hospital settings and a discussion of solutions that will keep patients safe and get glucose levels to goal. In addition, sample basal/bolus and insulin drip guidelines plus lots of resource articles are included.
Objectives:
- Discussing appropriate insulin dosing based on the patient’s clinical presentation
- Applying dosing strategies to a variety of case studies
- Introduce hard-to-manage situations that commonly occur in hospital settings
- A discussion of solutions that will keep patients safe and get glucose levels to goal
- Sample basal/bolus and insulin drip guidelines plus lots of resource articles are included
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.