

For last week’s practice question, we quizzed test takers on DKA. Only 53% of respondents chose the best answer, which indicates that there was some uncertainty. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR, a 67-year-old with type 2 diabetes for seven years and an A1C of 9.7% was started on empagliflozin 10mg two weeks ago. Other labs include a GFR of 49 and a UACR of 34 mg/g. Other diabetes medications include glucotrol 10mg twice daily and sitagliptin 100mg daily. JR sometimes has a few shot’s of whiskey before bed, especially if they had a stressful day. JR’s partner calls you in a panic and says JR is admitted to the hospital in DKA.
What is the most likely explanation?
Answer Choices:
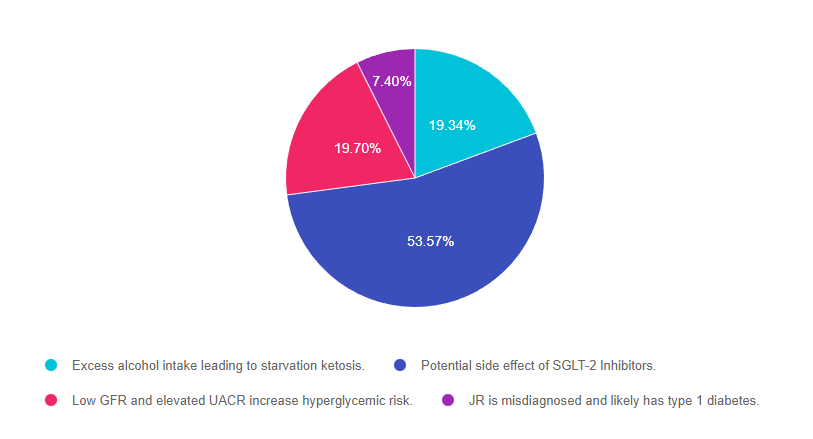
- Excess alcohol intake leading to starvation ketosis
- Potential side effect of SGLT-2 Inhibitors
- Low GFR and elevated UACR increase hyperglycemic risk
- JR is misdiagnosed and likely has type 1 diabetes
Getting to the Best Answer
Answer 1 is incorrect. 19.34% chose this answer, “Excess alcohol intake leading to starvation ketosis.” Although this answer is tempting, it is not the best answer. According to the vignette, “JR sometimes has a few shot’s of whiskey before bed, especially if they had a stressful day”. The American Diabetes Association states that women can have 1 drink a day and men can have up to 2 drinks a day. Given that JR only seems to drink a few shots when stressed out, this would not be considered excess alcohol intake associated with malnutrition.
Answer 2 is correct. 53.57% of you chose this answer, “Potential side effect of SGLT-2 Inhibitors.” YES, great job choosing the best answer. The SGLT’s have been associated with a rare but serious adverse drug effect called euglycemic diabetic ketoacidosis (DKA). This seems to be more likely if the person is on insulin and decreased their insulin dose in response to lower blood sugars from the addition of a SGLT-2. However, DKA can also happen to people started on SGLT-2s who are not taking insulin. People taking this class of medication need to be aware of the signs of DKA and appropriate action.
Answer 3 is incorrect. 19.70% of respondents chose this answer, “Low GFR and elevated UACR increase hyperglycemic risk.” With a GFR of 49 and a UACR of 34 mg/g, JR is a perfect candidate for the SGLT-2 Inhibitor class of medication. This class of medication preserves renal function while lowering A1C. JR’s GFR is well above the cut-off point and JR is not at increased risk of hyperglycemia.
Finally, Answer 4 is incorrect. 7.40% chose this answer, “JR is misdiagnosed and likely has type 1 diabetes.” Although it is possible that this is true, it is unlikely. JR has a 7 year history of type 2 with a moderately increased A1C on oral medications only. If JR had type 1 diabetes, the A1C would certainly be more elevated, since glucotrol 20mg and sitagliptin 100mg daily, would not be effective without a semi-functional pancreas. JR might have latent autoimmune diabetes in adults, so checking the GAD, ICA and IAA for autoimmunity could be enlightening.
For a listing of diabetes medications, side effects and considerations, please download our PocketCards
Want to learn more about this topic?
Dr. Diana Isaacs is providing a fantastic pharmacology update.
Virtual DiabetesEd Training Conference | 30+ CEs
Airs October 12-14th, 2022
Join us LIVE for this Virtual Training Conference and enjoy a sense of community!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
- Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES – Educator of the Year, 2020
- Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
- Ashley LaBrier, MS, RD, CDCES, Diabetes Program Coordinator
Two Registration Options
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.