

“I’ve managed my diabetes for years, but ever since starting cancer treatment, my blood glucose has been all over the place. I don’t know what I am doing wrong.”
As diabetes health professionals, our job is to support people through both complex clinical situations and the emotional challenges of living with cancer and diabetes. Having the knowledge to address both can improve engagement, lead to better outcomes, and strengthen relationships with the people we work with.
Diabetes and cancer are no longer just parallel health crises sharing a person’s chart; they are deeply entangled pathologies where hyperglycemia, inflammation and the risk of cancer development are interrelated. For diabetes healthcare professionals, mastering this bidirectional threat no longer falls under the rare case scenario.
As a diabetes professional, you have an important role in detecting sudden hyperglycemia as a result of chemotherapeutic agents, like checkpoint inhibitors and PI3k inhibitors. In addition, you can encourage people with diabetes to engage in regular cancer screenings and be aware of reportable symptoms. This is an immediate, high-stakes clinical mandate that can improve prompt treatment and detect cancer earlier.
The shared risk factors between type 2 diabetes and cancer (older age, elevated body weight, and lack of physical activity) increase this bidirectional association, but diabetes-related factors such as underlying disease physiology or diabetes treatments may also increase this cancer-diabetes connection.
Link Between Hyperglycemia and Specific Cancers
One of the most clinically actionable areas of recent research highlights the relationship between a new diabetes diagnosis and pancreatic and other cancers.
People with type 2 diabetes face about twice the risk of developing pancreatic cancer compared to those without the condition, while an older adult (over 50) with new-onset diabetes experiences a sharper increase in risk within the first few years.
New onset of atypical diabetes (lean body habitus and negative family history) in a middle-aged or older person may precede the diagnosis of pancreatic adenocarcinoma. Additionally, in a nationwide cancer registry in New Zealand, post pancreatitis diabetes mellitus was associated with significantly higher risk (2.4-fold) of pancreatic cancer compared with pancreatitis after type 2 diabetes. (ADA).
What about other types of Cancers?
Diabetes is associated with increased risk of cancers of the liver, pancreas, endometrium, colon and rectum, breast, and bladder.
Large-scale cohort analyses reveal that individuals with diabetes face a roughly doubled risk of developing
- pancreatic,
- liver, and
- endometrial cancers.
There are also notable 1.2- to 1.5-fold increases in:
- colorectal,
- breast, and
- bladder cancers.
Take action Today to Prevent and Detect Cancer
People with diabetes are encouraged to schedule recommended age-and sex-appropriate cancer screenings, coordinated with their primary health care professional. As diabetes professionals, you can encourage individuals to take action and to reduce their modifiable cancer risk factors. Actions that help with diabetes management also reduce risk of cancer including:
- Healthy eating, high fiber, low processed foods
- Increase activity
- Decrease alcohol intake and quit smoking.
The link between Chemotherapy and Hyperglycemia
Cancer Therapies as Beta-Cell Disruptors
The cancer frontier of oncology has been revolutionized by precision therapies, but these life-saving advancements can come with steep glucose elevations due to beta cell disruption.
Hyperglycemia due to chemotherapy may either be transient (improving upon treatment cessation) or represent permanent diabetes.
Checkpoint Inhibitors
Immune checkpoint inhibitors are used to treat many types of cancer, such as melanoma, non-small cell lung cancer, bladder cancer, renal cell carcinoma, breast cancer, and Hodgkin lymphoma.
Common immune checkpoint inhibitors include: pembrolizumab (Keytruda), nivolumab (Opdivo), ipilimumab (Yervoy), durvalumab (Imfinzi), atezolizumab (Tecentriq).
- Immune checkpoint inhibitors (ICIs) impair the function of the immune system, allowing for immunogenic response against cancer cells. This impairment can result in autoimmune toxicities, including an autoimmune form of diabetes that results in β-cell destruction in less than 1% of people receiving ICI therapy.
The most likely Immune checkpoint inhibitors that rigger rapid, autoimmune-mediated destruction of beta cells include:
- anti-PD-1 (i.e., nivolumab and pembrolizumab) and
- those that target programmed cell death protein ligand 1 (PD-L1) (i.e., durvalumab and avelumab).
- Hyperglycemia as a result of ICIs can occur at any time after the initiation of therapy—as quickly as 1 week after the first dose to up to 12 months after.
Treatment for Hyperglycemia secondary to Checkpoint Inhibitors
Insulin therapy is the cornerstone of management, as individuals typically present with rapid-onset, severe hyperglycemia or DKA. Many will initially need an insulin drip, followed by the implementation of basal bolus insulin therapy along with continuous glucose monitoring.
PI3K Inhibitors
PI3K inhibitors are used primarily to treat advanced breast cancer (specifically HR+/HER2- tumors with PIK3CA mutations) and blood cancers (such as lymphomas, leukemias, and follicular lymphoma).
Phosphatidylinositol 3-kinase (PI3K) inhibitors are small molecules designed to disrupt intracellular signaling pathways, thereby inhibiting cancer cell growth and survival. Within this class, targeted inhibition of the alpha isoform (PI3Kα) disrupts downstream insulin receptor signaling, frequently resulting in profound, on-target hyperglycemia and acute insulin resistance.
Which PI3K medications are associated with glucose elevations?
- Specific PI3Kα inhibitors include alpelisib and inavolisib.
These two types of PI3Kα inhibitors have a 60% incidence of causing hyperglycemia, typically appearing within the first 2 weeks of therapy.
People at increased risk of hyperglycemia from PI3K inhibitor therapy include those with:
- preexisting prediabetes
- BMI >25
- age >65 years
- being treated with glucocorticoid.
Glucose management is crucial since significant hyperglycemia can lead to discontinuation and/or reduction in PI3K medication dose, which can decrease therapy efficacy.
Treatment for Hyperglycemia secondary to PI3K Inhibitors
- Metformin is the first-line oral agent to treat PI3K inhibitor–induced hyperglycemia. According to the ADA Standards, proactive use of metformin may also be beneficial in preventing hyperglycemia in individuals receivingz PI3Kα inhibitors (alpelisib and inavolisib). However, it is important to consider potential adverse effects of metformin therapy, particularly diarrhea, which is also a frequent adverse effect of PI3Kα therapy.
- Pioglitazone is also an option as monotherapy or in combination with metformin, but its slow onset of action can limit its effectiveness.
- SGLT2 inhibitors have also shown efficacy, but close monitoring is needed, as ketoacidosis has been reported.
- Insulin and sulfonylureas should be considered only as a last resort, as increased insulin levels may reactivate the PI3K pathway, counteracting the antitumor effects of PI3K inhibition.
- Avoid using GLP-1 RAs with PI3K inhibitors- Treatment is not recommended at this time due to their uncertain effect on PI3K inhibitor efficacy (based on their increase in insulin secretion) and the potential to cause nausea and vomiting.
- Download our Diabetes PocketCards Here
Steroid Induced Hyperglycemia
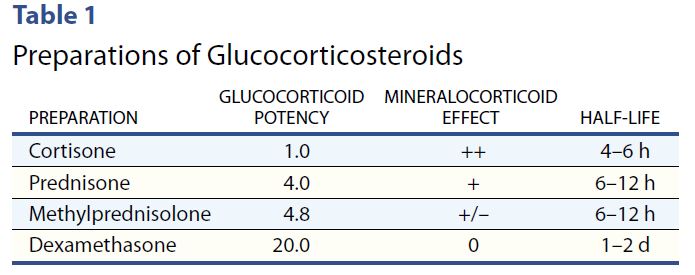
Cancer treatment often includes concurrent steroid therapy to enhance efficacy. However, steroid therapy can induce or worsen hyperglycemia.
Steroids have their highest potency at 4-12 hours, with the exception of the very potent dexamethasone, which has a half life of 1-2 days.
With morning steroids, including dexamethasone, people will experience elevated glucose values after breakfast, lunch, dinner, and at bedtime but will have a significant drop toward normal glucose overnight.
Therefore, hyperglycemia is greatest 1–2 hours after a meal, with persistent elevation until the following meal, followed by a return to normal overnight.
To treat steroid induced hyperglycemia, NPH. Neutral Protamine Hagedorn (NPH) insulin is an effective treatment choice since it is an intermediate acting basal insulin. NPH insulin is cloudy and has an onset of 1–4 hours. Its peak is 6–10 hours and its duration is about 10–16 hours. Download our Insulin PocketCards.
For individuals on once daily steroids, morning NPH with some bolus insulin can effectively target daytime hyperglycemia. For those taking steroids twice daily, an additional dose of NPH plus bolus as needed, is added at dinnertime.
Join Coach Beverly July 21 at 11:30am to learn more during our Cancer and Diabetes Webinar.
Advancing Clinical Practice: Integrating Cancer Care into Diabetes Care
As diabetes professionals, we are stepping into a vital new role at the intersection of metabolic health and oncology. Modern cancer therapies like checkpoint inhibitors and PI3K inhibitors are absolute game-changers for oncology, but they often trigger sudden, severe hyperglycemia that catches patients and healthcare professionals off guard.
That is where our expertise becomes a literal lifesaver. By actively monitoring for sudden hyperglycemia and aggressively championing routine cancer screenings, we are doing so much more than just managing a chronic disease. We are taking on an urgent, high-stakes clinical mandate that ensures patients get immediate treatment when they need it most and catches cancer at its earliest, most treatable stages.
Ultimately, our vigilance bridges the gap between effective cancer therapy and safe metabolic health, directly shaping better, life-saving outcomes for the people in our care.
References
- American Diabetes Association Professional Practice Committee for Diabetes*; 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes—2026. Diabetes Care 1 January 2026; 49 (Supplement_1): S61–S88. https://doi.org/10.2337/dc26-S004
- American Diabetes Association Professional Practice Committee for Diabetes*; 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026. Diabetes Care 1 January 2026; 49 (Supplement_1): S183–S215. https://doi.org/10.2337/dc26-S009
- American Diabetes Association Professional Practice Committee for Diabetes*; 3. Prevention or Delay of Diabetes and Associated Comorbidities: Standards of Care in Diabetes—2026. Diabetes Care 1 January 2026; 49 (Supplement_1): S50–S60. https://doi.org/10.2337/dc26-S003
- How to Manage Stroid Diabetes in the Patient With Cancer
Join Coach Bev on July 21st for our
Level 5 | Cancer & Diabetes Webinar | 1.5 CEs
Explore the unexpected link between cancer and diabetes — and master glucose management strategies for people with diabetes undergoing treatment.
Individuals with cancer often experience hyperglycemia secondary to treatment, which can increase the risk of infection and other complications. Recent research has also identified a significant link between diabetes and cancer. This course uses a case study approach to explore this connection and provide practical strategies for managing steroid-induced hyperglycemia and improving quality of life for people navigating both conditions.
Course Topics:
- Discuss the relationship between cancer, hyperglycemia, and insulin resistance
- State 3 benefits of normalizing glucose levels during chemotherapy
- Using a case study approach, discuss strategies to improve glucose levels and quality of life