
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Unsure about updates for this mastery level 2021 exam?
Join us to get ready to succeed at the BC-ADM Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness.
This free webinar will review BC-ADM requirements for the current year.
She will also review sample test questions and the reasoning behind choosing the right answers. We hope you can join us.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 6 times and first earned her BC-ADM credential 20 years ago. She is a nationally recognized diabetes expert for over 25 years.
Beverly has custom designed this course bundle to prepare you for your BC-ADM Exam. Including Level 2 (Standards of Care Intensive), Level 3 (Boot Camp), and Level 4, you can start studying now with 29 On-Demand webinars and practice tests to build your diabetes education foundation and prepare for the BC-ADM Exam.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For our January 26th Question of the Week, over 70% of respondents chose the best answer!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: RJ is 52 with type 1 diabetes and a minor stroke last year. RJ takes an ACE Inhibitor, insulin, and a statin.
According to ADA Standards of Care 2021, what is the blood pressure target for RJ?
Answer Choices:
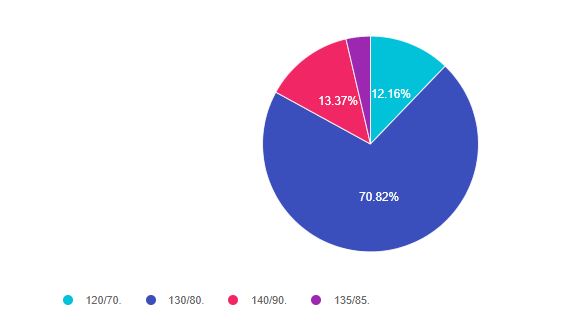
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 1, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success.
Answer 1 is incorrect 12.16% chose this answer. “120/70”. The ADA Standards suggest that we provide information on healthy eating and the importance of activity, coupled with a referral to a RD and DSMES, when blood pressure levels are greater than 120/70. But, this is not the blood pressure management goal.
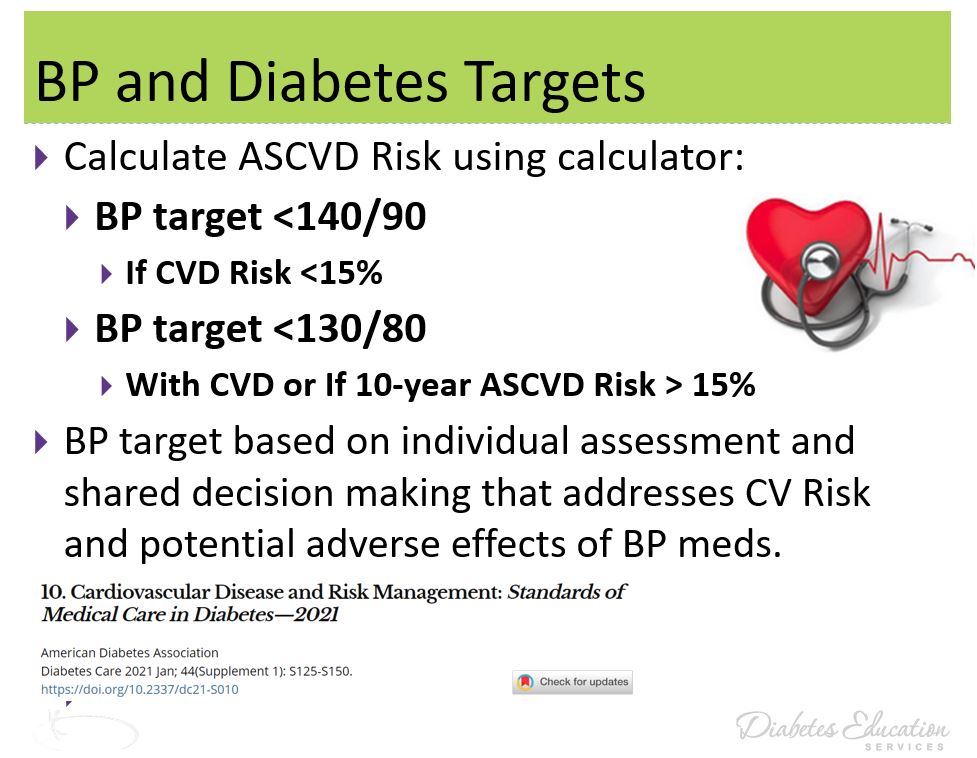
Answer 2 is correct 70.82% of you chose this answer. “130/80”. This is the best answer. Since RJ had a stroke, they walk through the door with an existing CV event, which identifies them as higher risk for a future event. The standards state that if the person has experienced a CV event or has a 10 year risk of 15% or greater (using the ASCVD Risk Calculator), the blood pressure target is 130/80.
Answer 3 is incorrect 13.37% of you chose this answer “140/90” The ADA Standards state that the blood pressure target is 140/90 if the 10 year risk of a CV event is less than 15% or the person has not experienced a previous CV event. Since RJ had experienced a minor stroke, the target is 130/80. Of course, this goal is individualized based on individual factors and a risk/benefit analysis.
Answer 4 is incorrect 3.65% of you chose this answer. “135/85” The standards state that if the person has experienced a CV event or has a 10 year risk of 15% or greater (using the ASCVD Risk Calculator), the blood pressure target is 130/80.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
I started walking while working 7 years ago after reading research on how “sitting was the new smoking”. I purchased my treadmill desk in 2013 and since that time, I have been walking 7 miles a day, through a combination of my treadmill desk and outdoor strolls.
Over the past 7 years, I have accumulated almost 18,000 miles in an attempt to prevent heart disease, cancer, and a myriad of other chronic health problems. But it seems there is more to the story.
The Terry Gross interview with Daniel Lieberman, a professor at Harvard in the department of human evolutionary biology, put my beliefs into question. Dr. Lieberman recently penned a book called “Exercised”, which details his research finding and dispels some commonly held myths.
Besides being a super-smart paleoanthropologist and professor, Lieberman has also spent a lot of time with indigenous hunter-gatherers in Africa and Latin America. He has observed and cataloged how much time they spend walking, running, lifting, carrying, and sitting.
Based on current hunter-gathering behaviors, Dr. Lieberman calculates our ancestors walked about 5 miles a day or 10,000 steps. The average adult in America walks about half of that distance or 5,000 steps a day which equals 2.5 miles. This number might be even lower over the past year, given the pandemic and people working from home.
Even though we walk less than our ancestors, Lieberman is encouraging. He says if 10,000 steps feel out of reach, it’s okay to aim for less, as long as the person focuses on movement and engaging muscles to prevent atrophy. Any movement is better than no movement!
“The more we study physical activity, the more we realize that it doesn’t really matter what you do,” Lieberman says. “You don’t have to do incredible strength training … to get some benefits of physical activity. There’s all different kinds of physical activity, and it’s all good in different ways.”
Daniel lieberman
2. Hunter-gatherers sit a lot less than modern humans.
Not true. Surprisingly, research on hunter-gatherers reveals that they sit for 10 hours a day on average, which is the same amount of times the average American sits.
Humans are designed to conserve energy in case of a lack of adequate nutrition. Most hunter-gatherers Lieberman studied don’t have chairs, but they spent a great deal of time sitting. This lack of chairs is actually associated with better spine and back health (see more below)
3. Sitting is really that bad for us.
Interrupted sitting is a far better approach than nestling your body in a comfy chair for hours at a time.
Time spent sitting at work isn’t the major problem. It’s leisure time sitting for hours at a time that is associated with poor health outcomes like heart disease, cancer, or diabetes.
But regardless of sitting at work or home, just getting up every once in a while, every 10 minutes or so makes a big difference in health outcomes.
Try to intentionally get up frequently to go to the bathroom or pet the dog or make yourself a cup of tea. Even though you’re not spending a lot of energy, you’re turning on your muscles. Since muscles are the largest organ in your body, using them decreases inflammation and burns fat and glucose.
4. You can prevent back pain by getting lumbar support or a fancy chair.

Another myth.
Up until recently, only the upper class had chairs with a seatback. Most human beings usually sat on the ground, stools, or benches. The problem with chairs with backs is that sitting becomes more of a passive activity since you use fewer muscles to stabilize your upper body.
Using chairs with seat backs result in weaker back muscles that begin to atrophy due to disuse.
Chairs with lumbar support and lots of cushioning may encourage sitting for longer periods of time, which may further contribute to muscle loss.
5. Getting 8 hours of sleep a night is essential for well being
Based on Lieberman’s research of people who live in places where there is no electricity and computer screens, they don’t sleep more hours than the average American.
People in regions without electricity sleep on average 6.7 to 7.1 hours a night.
Lieberman says we need to stop sleep shaming.
It is true, that not getting enough sleep (4-5 hours a night) can be detrimental to health. But, if a person is getting 6 or 7 hours of sleep a night and they feel fine, that is what is most important.
Read the complete article here: Just Move: Scientist Author Debunks Myths About Exercise and Sleep
Please see our Exercise Resource Page for handouts to share
Save your spot for our
Virtual DiabetesEd Specialist Conference | April 15-17, 2021
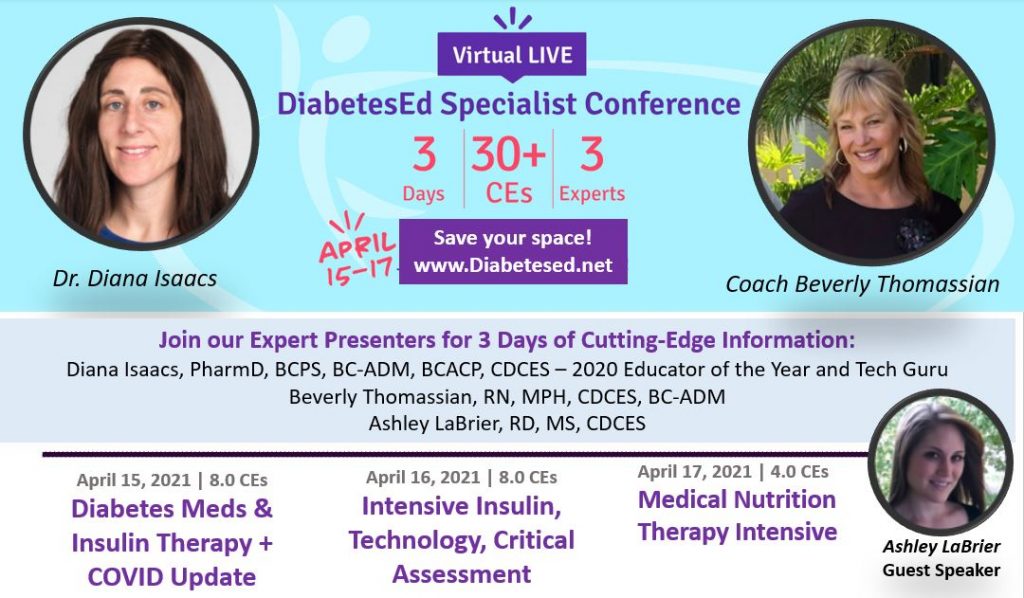
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice. If you are interested in taking the CDCES or BC-ADM exam or are seeking a state-of-the-art review of current diabetes care, this course is for you.
Entire Program Fee: $399
Dates: April 15-17, 2021
3 Expert Speakers
CEs: 30+ CE hours
Live Webinar Schedule: All webinars start and end times are in Pacific Standard Time
Come join our Virtual DiabetesEd Specialist Program.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.
This virtual program includes:
3 day live webinar courses from April 15th-17th (20 CEs) + enrollment in our Bonus Bundle (14.0+ CEs) from now through December 2021.
View full Conference Schedule and Faculty.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JL is 65 years old and has diabetes. JL tells you they had two different pneumonia vaccines in the past, but they are wondering what vaccinations they need this year.
What is the BEST answer?
Click here to test your knowledge!
This course is an essential review for anyone in the field of diabetes. This course summarizes the 2021 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for health care professionals involved in diabetes care and education.
Earn 2.0 CEs and get ready to lead the charge to implement best care practices for the New Year.
Topics Include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
World Diabetes Day is celebrated in honor of Dr. Fredrick Banting, whose leadership, tenacity, and belief led to the discovery of insulin.
The discovery of insulin has saved the lives of countless millions of people over the past hundred years and will continue to save millions of lives in the near future and beyond.
During a hot summer in 1921, Dr.Banting secured space to test out his theory at the University of Toronto. Along with his colleague, Charles Best, and a bare-bones lab, they conducted dozens of experiments on dogs, which ultimately led to the discovery of insulin.


Dr. Banting and Charles Best began their experiments ligating the pancreases of dogs, thinking this would prevent destruction by the digestive pancreatic juices, and then isolating the extract from the islet cells. They then processed the extract from the islet cells and injected this extract they called “insulin” into diabetic dogs. According to an audio interview with Dr. Best, by July 1921, they had 75 positive examples of insulin lowering blood glucose levels in dogs.

In February 1922, doctor Frederick Banting and biochemist John Macleod published their paper on the successful use of an alcohol-based pancreatic extract for normalizing blood glucose levels in a human patient.
Here are some photos of the first insulin bottles produced by the University of Toronto and Eli Lilly.
Soon, word of their discovery got out and the race was on to produce enough insulin to treat the flood of type 1 patients arriving in Toronto to receive this miracle injection.
But, as with any amazing discovery, there is always more to the story.
One of the biggest barriers to Banting was the simple fact that he was not involved in the field of diabetes research. The idea leading to the discovery of insulin came to him after preparing a lecture on the pancreas and diabetes, a subject he knew little about. He wasn’t a trained researcher and thus securing support for the project was initially difficult.
First Children to Receive Insulin
The first patient to receive insulin was a ‘welfare’ case at Toronto General Hospital – no clinical trial structure to say the least. People from Canada/US flooded into Toronto to receive treatment. Banting struggled with the lack of accessibility of insulin – volume needed issues of purification.
The earliest patients were “selected”, some youths from Canada/US, some soldiers with diabetes (probably because of Banting’s service in the First World War), and then later some select private patients. During this time they were working hard to increase the volume and continue to improve the purification process. Insulin was available for testing in the US, namely through Dr. Elliot Joslin in the late summer of 1922.
Takes a Team

While Best played a critical and important role, credit must also go to Professor Macleod, from the University of Toronto, who provided the lab space, showed Dr. Banting how to operate on dogs, provided his student Best and suggested they switch from saline to alcohol to purify the ‘extract’. Dr. Macleod also secured the support of JB Collip, the 4th man on the team, and the first person to purify insulin for human use. Best is also known for pushing Banting to return to the research during a particularly dark period of failure.
Dr. Banting – Fun and Interesting Facts
Want to Learn More About Dr. Banting?
Visit Banting House FaceBook Page
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]For our January 19th Question of the Week, over 77% of respondents chose the best answer!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question:
MT is 59 and her most recent A1c was 10.3%. The diabetes specialist suggested they add insulin to her other 3 oral diabetes medications to lower A1c. MT was not ready for insulin, so the specialist agreed that they would try adding on glipizide 5mg BID and evaluate the response for one month.
After 2 weeks, MT calls and is very upset about her frequent low blood sugars (66, 68, 69) that are happening between 3 pm and 6 pm a few times a week. MT works in the field starting at 5 am and gets her lunch break at 10 am and eats her dinner again at 6 pm.
Answer Choices:
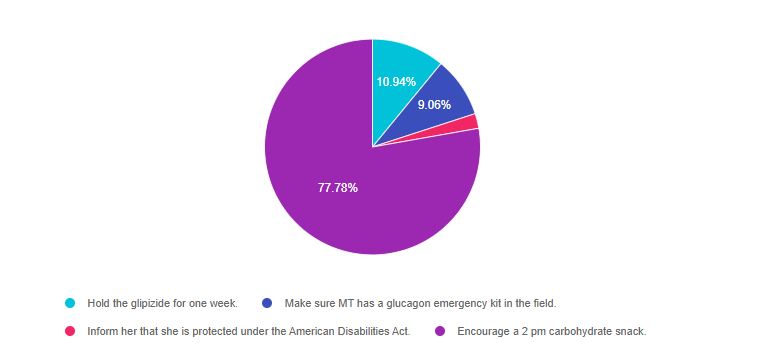
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally option 3.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success.
Answer 1 is incorrect 10.94% chose this answer. “Hold the glipizide for one week.” Since MT had a very elevated A1c of 10.3%, holding the glipizide for a week could lead to a dangerously elevated blood glucose. A more nuanced intervention is required.
Answer 2 is incorrect 9.06% of you chose this answer. “Make sure MT has a glucagon emergency kit in the field.” MT doesn’t need a glucagon emergency kit at this point. Since MT can detect the signs hypoglycemia, they just need instruction to eat a 15gm carb snack to treat these symptoms and avert a hypoglycemic emergency.
Answer 3 is incorrect 2.22% of you chose this answer “Inform her that she is protected under the American Disabilities Act (ADA).” It is important for people with diabetes to know that they are protected under the ADA. They have the right to monitor their blood glucose, take medications/insulin at work and take a break to treat hypoglycemia. However, this is not the best answer.
Answer 4 is correct 77.78% of you chose this answer. “Encourage a 2 pm carbohydrate snack.” Since MT is having is having low blood sugar consistently between 3pm and 6pm, we do some investigation and find out the MT is not eating for up to 8 hours. For people taking sulfonylureas, like glipizide, they need to eat every 4-5 hours to match the extra insulin the pancreas is producing in response to the glipizide. A 15 gm snack at 2pm would be a perfect solution to prevent hypoglycemia and allow MT to continue taking the glipizide to keep blood glucose levels on target.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Dawn Desoto RD, CDCES, celebrates the winter season with a collection of recipes that nourish and provide comfort.
Yield 2 servings

Directions
Simply pour all ingredients into a small saucepan, whisk to combine ingredients. Heat until hot to the touch but not boiling – about 4 minutes. Enjoy warm.

Directions
Combine is a small saucepan and whisk until the consistency is smooth and silky. Pour into mugs. Give thanks. Enjoy.

Directions
Toss whole mushrooms, olive oil, and salt and pepper to taste in a bowl. Spread on a baking dish and roast at 425 degrees F, stirring a few times, until tender and browned for 30 to 35 minutes. Cook thinly sliced garlic cloves and smoked paprika in butter until soft, toss with the mushrooms. Sprinkle with chopped parsley and salt. Enjoy.

Instructions
We hope you enjoy these delicious recipes!
Written by Dawn DeSoto RD, CDCES, our resident Nutrition Content Writer
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
RJ is 52 with type 1 diabetes and a minor stroke last year. RJ takes an ACE Inhibitor, insulin, and a statin.
According to ADA Standards of Care 2021, what is the blood pressure target for RJ?
Click here to test your knowledge!
This course is an essential review for anyone in the field of diabetes. This course summarizes the 2021 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for health care professionals involved in diabetes care and education.
Earn 2.0 CEs and get ready to lead the charge to implement best care practices for the New Year.
Topics Include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.