
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
The InPen smartpen, by Companian Medical, is now FDA approved for all ages!
The Inpen is a reusable battery-powered insulin pen that uses insulin cartridges. It is approved for use with three different insulins; Novolog, Humalog, and Fiasp. It can deliver insulin in half-unit doses plus it monitors insulin temperature. The battery lasts for a year and requires no charging.
“We are excited that we can help younger children and even more parents navigate the challenges associated with Type 1 diabetes. Now anyone can safely use InPen to help make decisions around insulin dosing, no matter what their age,”
Sean Saint, CEO and co-founder of Companion Medical.
In addition to all these features, the InPen Bluetooth enabled software allows users to connect to a FREE app on their Apple iOS or Android mobile device to track and share insulin dosing and glucose levels.
New users enter their insulin to carb ratios and insulin sensitivity along with target glucose into the app settings. Based on that data, the software helps to calculate the insulin dose needed and alerts users to insulin on board to prevent stacking (which can help reduce hypoglycemia.)
People can use Inpen in combination with CGM or traditional glucose monitoring and reports can be shared with providers and caretakers
Here is what InPen users can track on the app dashboard:
The InPen requires a prescription and is covered by many insurance companies in the United States. Most InPen users pay a $35 copay. Companion Medical has a co-pay assistance program for people without insurance coverage – more info here.
As a Diabetes Specialist, I am excited to share information on these new and emerging options to deliver insulin therapy that reduce the burden of diabetes self-management and improve connections to caregivers and providers.
Thanks for reading our Tech Thursday Blog! More info on InPen Here .
Can cinnamon help maintain glucose in those with prediabetes?

There have been several studies over the past decade to determine the efficacy of using cinnamon supplements to regulate blood sugars. Most of the studies found either no significant change or slight changes.
For example, a 2013 study of 70 different participants found that those who took 1 gram of cinnamon daily showed no significant changes over 30 or 60 days.
However, a recent study found that cinnamon supplements may be beneficial over time for improving glucose homeostasis in prediabetes.
This study, conducted by Giulio R. Romeo, MD, from the Joslin Diabetes Center in Boston, and Dr. Romeo’s colleagues spanned over 12 weeks across 45 participants who met the criteria for prediabetes. These participants, who were not taking a placebo, took 500mg of cinnamon supplements a day to see the impact on glucose control.
From a similar baseline, FPG rose after 12 weeks with placebo but remained stable with cinnamon, leading to a mean between-group difference of 5 mg/dL (P<0.05). When compared to the respective baseline, cinnamon, but not placebo, resulted in a significant decrease of the AUC PG (P<0.001) and of the 2-hr PG of the OGTT (P<0.05). There were no serious adverse events in either study group.
Their study found that fasting plasma glucose (FPG) rose for those who took the placebo. For those who took cinnamon supplements, their area over the curve (AUC) plasma glucose (PG) decreased along with their 2 hour PG by oral glucose tolerance test (OGTT).
The results suggest that over time, a cinnamon supplement of 500mg a day may help blood glucose levels for those with prediabetes.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
RJ is 67 years old with a 40+ year history of type 1 diabetes. GFR is 62, UACR is < 30, A1c is 6.7%, B/P is 132/72, LDL cholesterol is 98, his BMI is 28.6. RJ uses multiple daily injections and CGM to manage his diabetes.
RJs other medications include: Levothyroxine 100mcg daily, atorvastatin 40mg daily, Aspirin 81 mg daily and a multivitamin.
Based on your assessment, which of the following interventions would improve RJs outcome?
Click here to test your knowledge!
Here at Diabetes Education Services, we are excited to celebrate World Breastfeeding Week!

Breastfeeding reduces the risk of future diabetes for mom and baby alike. Studies show that mothers who nursed babies for at least six months were 48 percent less likely to develop diabetes. Yet many mothers, who want to breastfeed, aren’t able to due to a variety of obstacles.
There are myriad benefits to breastfeeding, a fact that’s well-endorsed by upcoming World Breastfeeding Week. This event, which is sponsored by the World Alliance For Breastfeeding Action, focuses on promoting, protecting, and supporting breastfeeding around the globe.
“There could be greater health benefits for women from breastfeeding than previously recognized,” said lead study author Erica Gunderson of the Kaiser Permanente Division of Research in Oakland, California.
Each year, a new adjacent cause is championed; this year, the climate impact of formula feeding is central to the week-long event. Wisely, the organization makes a point to reflect on breastfeeding inequality as a series of obstacles that must be overcome in order to truly reap the ecological benefits of making this switch.
Below is an infographic that describes the critical issues surrounding breastfeeding inequalities that bring to light an often under-discussed issue. Blog also continues below.

Breastfeeding inequality refers to the disparity in breastfeeding rates that can be observed in socioeconomically disadvantaged areas. Even in developed countries like the United States, demographic areas that fall beneath the poverty line often reveal dismal statistics when it comes to breastfeeding. This visualization breaks down the impact of income, education, and other lifestyle factors on breastfeeding inequality:
For those who’ve simply been watching moms go back and forth online about choosing breast or bottle, learning that some mothers are at a legitimate disadvantage when it comes to breastfeeding can be shocking. Factors like income and partner support play a direct role in the home, but there are other reasons why breastfeeding rates in economically disadvantaged areas are low.
Optimum nourishment at no cost, improved parental bonds, and the possible prevention of future allergies, asthma, obesity, and type 2 diabetes are but a few of the reasons that breastfeeding equality is essential for all families. Though the fight is hard-fought, the health of a generation is a goal worth uniting for.
Written by Guest Writer, Neve Spicer, Founder & Director at Wetheparents.org
Resources

A committee of experts provides recommendations for healthy eating twice every decade. These final recommendations are sent to the US Department of Health and Human Services and the US Department of Agriculture, which use them to create the final 2020 dietary guidelines for Americans.
For the first time ever, the panel is including nutrition guidelines for infants 2 years and younger, with a pointed focus on reducing sugar consumption.
On average, infants consume a teaspoon of added sugar a day while toddlers consume about 6 teaspoons a day.
“Nutritional exposures during the first 1,000 days of life not only contribute to long-term health but also help shape taste preferences and food choices.”
2020 Dietary Guidelines Report
The committee also recommended further reductions in sugar intake for those age 2 and beyond. They also suggested less alcohol for men.
Read more about the 2020 Dietary Recommendations

Visit our Joy of Six Resource Page which has handouts and other helpful info on strategies to decrease sugar intake.
As a Diabetes Specialist in a rural clinic, you are asked to consult on a 49-year-old female with type 2 diabetes and a BMI of 27. Blood pressure is 132/74 with the following lab values; A1c of 7.6%, LDL of 97 mg/dl, triglycerides 138, and GFR of 69. Her medications include:
Metformin 850 mg three times a day, levothyroxine 100 mcg a day, and cetirizine 10mg daily.
According to the ADA Cardiovascular Standards of Care, what other medication therapy needs to be added?
Click here to test your knowledge!
My children have been a vital part of my company since before they were born. I remember providing all day lectures with puffy feet and the “waddle” with both of my pregnancies. When they were babies, my wonderful husband would travel with me and the boys to my lecture locations. We would pack up suitcases of supplies, so we could be together and I could breast feed during lecture breaks and in the evenings. I didn’t get much sleep in those days, but it was worth it!
When my boys were in elementary school, they helped assemble DiaBingo (now available for free) and stuff endless envelopes with PocketCards. They have listened to me share my ups and downs of running a business and have been some of my biggest supporters.

I am so proud that Robert and Jackson are official employees at Diabetes Education Services. They are significantly enhancing the services we are able to provide our wonderful community.
They have increased our presence on social media, improved website navigation and are contributing to many behind the scenes enhancements.
After working at the company for the past year, Robert is heading off to college. He spent the last month training Jackson to take over his role. He did a great job preparing his brother, but he also created a Training Manual that we will refer to for years to come. Robert will still be providing consultation on special projects and in case we get stuck in QuickBooks. I am one grateful Mama CEO.
Thank you, Robert, and Welcome Jackson!
Jackson is the newest member of our team. He is a rising sophomore and loves playing piano, video gaming with friends, and learning about science.
His job includes activities to make sure our operations run smoothly. He will be answering the phone, fulfilling orders, providing customer service, and completing a variety of quality improvement projects. He is also helping us update our CDCES Coach app with some new exciting features. Welcome, Jackson! We are thrilled to have you join us.

Robert has moved on to attend Southern Methodist University starting in August 2020. He aspires to obtain a Bachelor’s in Business. Robert gained many new skills ranging from social media engagement, to QuickBooks Online to formatting websites and fulfilling orders during his year at Diabetes Education Services. We wish him the very best as he pursues his college education in Texas and provides occasional consultation to our team. Thank you, Robert!
Meet our entire wonderful team here!
Perfect for those planning to take the CDCES / BC-ADM or for those who want to learn more about the technology used to manage diabetes.
If you want cutting edge information on diabetes technology, problem-solving, and using a formula to determine appropriate insulin dosing, we highly recommend this toolkit.
Can’t join us live? Recorded video and podcast versions are ready for On-Demand Viewing. All updates webinars are uploaded within 4 hours of the live show ending.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This question addressed the use of SGLT-2 Inhibitors in addition to insulin for MS, who is living with Type 1 Diabetes. MS is worried about weight gain and is on a low keto diet. It is safe for here to add an off-label medication?
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: MS has type 1 diabetes and is on a low carb diet to help her keep her weight on target. She has a BMI of 24.3. MS has a friend with type 1 who is taking an SGLT-2 in addition to insulin to help with weight management. MS wants to know if she could add on an SGLT-2 to her insulin treatment plan.
What is the Diabetes Specialist’s best response?
Answer Choices:
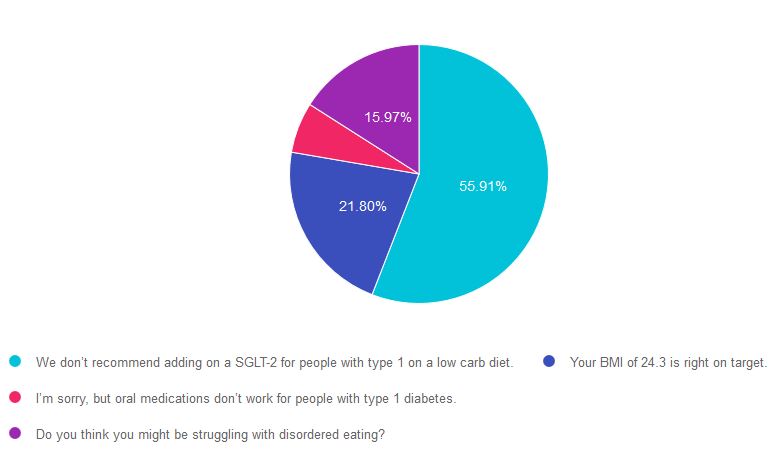
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 4, and finally option 3.
If you are thinking about taking a certification exam, this practice test question will set you up for success. The test writers will include warnings about medications and ask you to choose the best response. Your job is to weed through the particulars, pluck out the most important elements, eliminate at least two false answers to improve your odds of success to 50/50.
Answer 1 is correct! “We don’t recommend adding on an SGLT-2 for people with type 1 on a low carb diet.” Even though SGLT-2’s are sometimes prescribed to people with type 1 diabetes (in addition to insulin), they are not FDA approved in type 1 and are considered “off-label.” SGLT-2 also contains a warning of an increased risk of ketoacidosis. This risk is especially important to consider in type 1 diabetes, since people with type 1 using an SGLT-2 Inhibitor may decrease their daily insulin dose and increase the risk of ketoacidosis.
This risk might be exacerbated by a low carbohydrate diet. As outlined in the ADA Standard 5, “This [low carbohydrate] eating pattern is not recommended at this time for women who are pregnant or lactating, people with or at risk for disordered eating, or people who have renal disease, and it should be used with caution in patients taking sodium-glucose cotransporter 2 inhibitors due to the potential risk of ketoacidosis.”
Answer 2 is incorrect! “Your BMI of 24.3 is right on target.” This is a juicy answer because it is true. The BMI is below 25, but it does not address the key intent of the question.
Answer 3 is incorrect. “I’m sorry, but oral medications don’t work for people with type 1 diabetes.” This is tricky. No oral medications are FDA approved for type 1 diabetes, but some are prescribed (metformin, SGLT-2s) by diabetes providers in addition to insulin. Still not the best answer.
Finally, Answer 4 is incorrect. “Do you think you might be struggling with disordered eating?” Another tempting answer, but MS isn’t exhibiting any signs of under-eating or under-dosing insulin or disordered eating.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want more practice questions?
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions, and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

