Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
As we enter fire and storm season, it’s always a good idea to think ahead and be prepared for disaster. In addition to the items listed below, make sure to pack hand sanitizer, wipes, and masks due to the current pandemic. Also, bring your own pillow and bedding in case you need to spend time in a shelter.
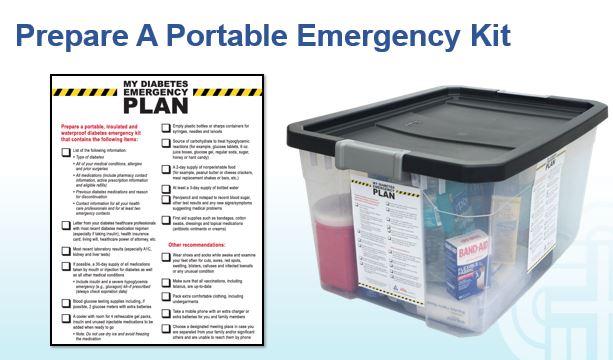
For any emergency scenario, it’s important to have an emergency preparedness plan. For people living with diabetes, a “diabetes kit” is an important part of emergency preparedness. Diabetes Disaster Response Coalition (DDRC) has put together great resources to help people with diabetes be prepared so that no one is caught unaware without medication.
DDRC’s Diabetes Kit checklist includes needed supplies, but more importantly, information that should be written down and kept in a waterproof container for emergency situations where a health care provider could find it and make informed emergency treatment decisions.
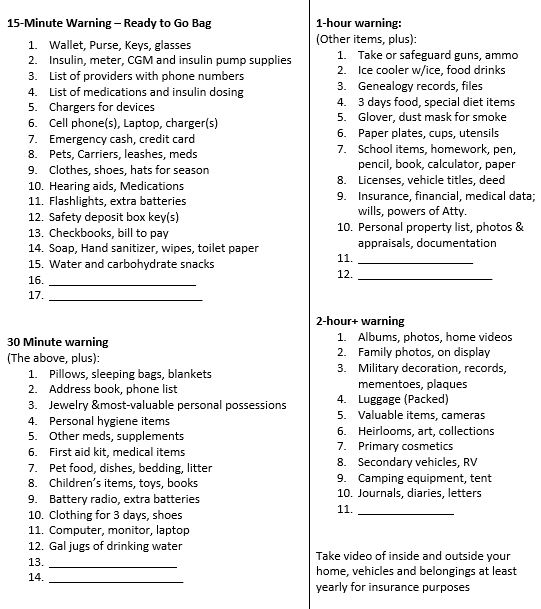
Emergency Evacuation-Items to Gather for People with Diabetes
We thought this list was a helpful way to prioritize what items to grab given different time frame limitations. We found it online, and customized it for people with diabetes. It is available in Word or PDF. Thank you for sharing with your colleagues and community.
1-800-DIABETES (800-342-2383) is an excellent referral resource for people with diabetes to call toll free for updates on accessing medical support during an emergency.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]

On my 40th birthday, I was gifted a Mission Fig tree that was no taller than my 5″ 7″ self.
The tree loved her new home and grew quickly, spreading out her limbs and gifting us with buckets of sweet fig fruit within a few years.
She is a strong and sturdy tree. My teenagers do pull-ups on her limbs and she has survived all kinds of weather events.
She rebounded after an intense wind storm, where her largest limb snapped off. Overburdened with figs, her trunk broke in half one season. We worried she wouldn’t make it, but that summer she produced even more figs.
When we were planning to build my office eight years ago, the architects told us our fig tree would need to be cut down to make room.
We altered our building plan and moved the location of my office to make room our beloved fig tree.
As a gesture of gratitude, our tree has blessed us with fig “over-abundance” year after year.
With my office doors open in the summer, I hear the birds fighting for the juiciest figs that thrive on her crown. During work breaks, we go outside, stand in her shade and search for the plumpest and biggest figs to eat on the spot and later to bake and top with a dab of goat cheese.
To extend our fig enjoyment through winter and beyond, we collected over 7 lbs of figs and made 9 jars of buttery fig jam.
With virtual coaching from my Aunt Hedy in Canada, I cut up 7 pounds of figs, added some sugar, fresh lemon juice and a generous cup of brandy. I cooked on low for at least four hours to blend flavors and reduce the jam to the perfect thickness. The brandy adds a smokey, caramel flavor to the jam, that my family loves. However, it also tastes great without it.
Here is the recipe for fig jam that I modified by cutting the sugar by one – half and then adding it back as needed for thickening.
Drunken Fig Jam (Coach Beverly’s modified recipe)
You can easily google a recipe with more detailed instructions, but here is the basic idea.
Put all of the above into a thick pot and mix. Let sit for an hour, stirring occasionally. Then put on a low heat and let simmer for 4-6 hours to reduce to desired thickness. You may need to add a little more sugar for thickening and lemon juice for the right balance of sweet and “lemonyness”.
Then put into sterilized jars and follow usual canning procedures. I always save one jar as a refrigerator jam that we can start enjoying right away.
With all that is going on in the world, I wanted to write a post that is life affirming and voices my gratefulness for the generosity of nature and my fig tree in particular.
Coach Beverly
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our August 4th Question quizzed test takers on CV Disease risk management and diabetes. Although 49% of respondents chose the correct answer, 51% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: RJ is 67 years old with a 40+ year history of type 1 diabetes. GFR is 62, UACR is < 30, A1c is 6.7%, B/P is 132/72, LDL cholesterol is 98, RJs BMI is 28.6. RJ uses multiple daily injections and CGM to manage RJs diabetes.
RJ’s other medications include: Levothyroxine 100mcg daily, atorvastatin 40mg daily, Aspirin 81 mg daily and a multivitamin.
Based on your assessment, which of the following interventions would improve RJs outcome?
Answer Choices:
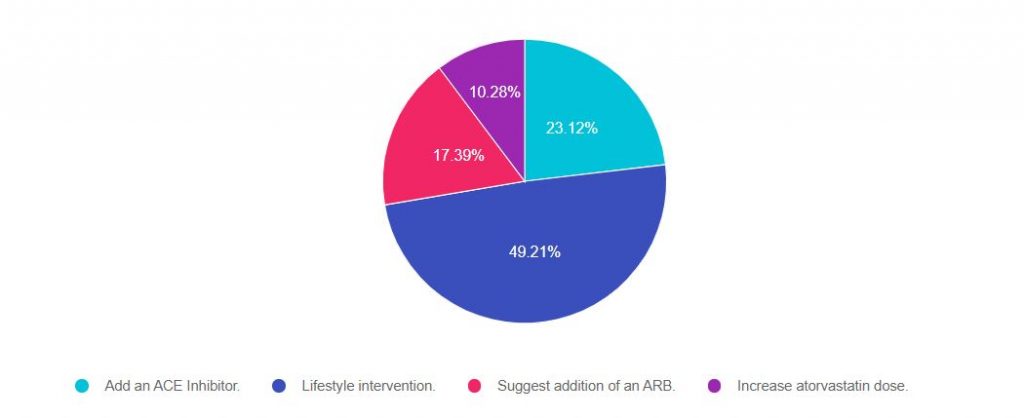
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers will ask about the guidelines for specific ADA Standards of Care. This question is pulled from section 10 of the Standards on CV Disease and Risk Management. To purchase your own ADA Standards, visit our store.
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
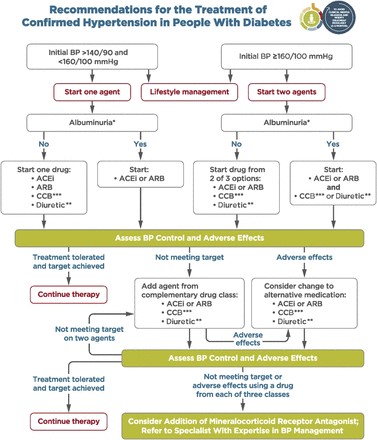
Answer 1 is incorrect. 23% chose this answer. “Add an ACE Inhibitor.”
Many people chose this juicy answer. It is true that in the past, people with type 1 would be automatically started on an ACE Inhibitor because it was thought starting an ACE would offer renal protection. However, based on extensive research, the American Diabetes Association stopped recommending adding an ACE for people with type 1 without the diagnosis of hypertension a few years back.
The current blood pressure goal for people with diabetes is 140/90.
If a person with type 1 diabetes has hypertension, defined as either systolic greater than 140 or diastolic more than 80, repeated on 2 different occasions, initiate blood pressure therapy.
Lower blood pressure goal of 130/80? It is recommended to do a cardiovascular risk assessment using the CV Risk Calculator on all people with diabetes. If the 10 year risk of having a CV event is greater than 15%, the blood pressure goal is 130/80 may be appropriate, if it can be safely attained. The choice of blood pressure therapy is further refined by presence or absence of microalbuminuria.
We don’t have enough information to calculate his CV Risk, so based on the information we have, adding an ACE Inhibitor is not indicated at this time. And of course, since we only have one blood pressure, we need to collect more data before taking action.
Answer 2 is correct. 49% of you chose this answer. “Lifestyle intervention.”
This is the best answer. Looking at this profile, we can see that RJ’s BMI is above 25 and LDL is slightly elevated. Let’s refer RJ to a Registered Dietitian. By coaching RJ on healthy food choices, increased whole foods and fiber, and taking a look at animal protein consumption, there is an opportunity to improve not only RJs blood pressure but also RJs LDL cholesterol. In addition, we can evaluate RJs activity level and encourage 150 mins a week of activity plus strengthening that would contribute to his overall health.
Answer 3 is incorrect. About 17% of you chose this answer. “Suggest addition of an ARB.” See rationale under answer 1.
Finally, Answer 4 is incorrect. 10% of you chose this answer. “Increase atorvastatin dose.” Currently, RJ is on high intensity statin therapy with RJs atorvastatin dose of 40mg. He does not present with any concerning CV risk factors or events that would kick RJ into high risk category. We could calculate RJs 10 year risk of CV disease and if it is more than 20% or if RJ doesn’t response to lifestyle changes, we could consider a further increase in the statin dosing. Based on the info we have at this moment, this is not the BEST answer (but it is a consideration : -).
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Click here to test your knowledge!

Join us Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
Many of you are curious about the steps involved in becoming a BC-ADM. Thank you for reaching out to us with your questions about eligibility and study strategies. Coach Beverly will be providing answers to your questions interwoven with her own journey to achieve her Board Certification in Advanced Diabetes Management (BC-ADM).
Becoming Board Certified in Advanced Diabetes Management (BC-ADM) is an excellent professional goal for diabetes specialists with an advanced degree in their field and a professional license as an advanced practice nurse, registered dietitian, or registered pharmacist or provider.
The person holding the BC-ADM credential skillfully manages complex patient needs and assists patients with their therapeutic problem-solving. Within their scope of practice, healthcare professionals who hold the BC-ADM certification:
The scope of advanced diabetes practice includes clinical management skills such as medication adjustment, medical nutrition therapy, exercise planning, counseling for behavior management, and psycho-social issues. There is a focus on research, national standards, medical management of diabetes, and co-conditions, with a person-centered care approach.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Join us Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
Many of you are curious about the steps involved in becoming a BC-ADM. Thank you for reaching out to us with your questions about eligibility and study strategies. Coach Beverly will be providing answers to your questions interwoven with her own journey to achieve her Board Certification in Advanced Diabetes Management (BC-ADM).
Becoming Board Certified in Advanced Diabetes Management (BC-ADM) is an excellent professional goal for diabetes specialists with an advanced degree in their field and a professional license as an advanced practice nurse, registered dietitian, or registered pharmacist or provider.
The person holding the BC-ADM credential skillfully manages complex patient needs and assists patients with their therapeutic problem-solving. Within their scope of practice, healthcare professionals who hold the BC-ADM certification:
The scope of advanced diabetes practice includes clinical management skills such as medication adjustment, medical nutrition therapy, exercise planning, counseling for behavior management, and psycho-social issues. There is a focus on research, national standards, medical management of diabetes, and co-conditions, with a person-centered care approach.

This free webinar will review BC-ADM requirements for the current year.
Coach Beverly will discuss:
She will also review sample test questions and reasoning behind choosing the right answers. We hope you can join us.
Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
**To satisfy the requirement for renewal of certification by continuing education for the Certification Board for Diabetes Care & Education (CBDCE), continuing education activities must be applicable to diabetes and approved by a provider on the CBDCE List of Recognized Providers (www.ncbde.org). CBDCE does not approve of continuing education. Diabetes Education Services is accredited/approved by the Commission of Dietetic Registration which is on the list of CBDCE Recognized Providers.”
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
We are off to College!

Good morning everyone, Beverly won’t be at work today. She will be taking the next step in moving her son toward independence.
In 2002, Beverly brought her firstborn into the world.
Now she is bringing him to college.
After surviving the first 18 years of motherhood (barely), Coach Beverly is ready to kick (gently) her oldest little fledgling, Robert, out of her nest and into the much bigger nest of the collegiate world.
Robert shows all the signs of readiness to leave his home of origin behind and move to the dorms to start college at SMU (Go Mustangs) in Texas.
Robert’s signs of readiness to move out and move on include:
These are all signs that we have succeeded at our job as parents. Now with a mixture of joy and a twinge of longing, I will deliver him to the next stage of his journey.
Our prayers are with him. We will keep you posted!
How long does glulisine last in pumps? What insulins can people buy without a prescription? What is the longest lasting insulin? If you want to learn the answers to these questions an more, we are here to help!
With the pandemic and ongoing insulin pricing issues, many people are struggling to pay for their insulin. Armed with information, we can help people maximize their insulin use and optimize their choices.
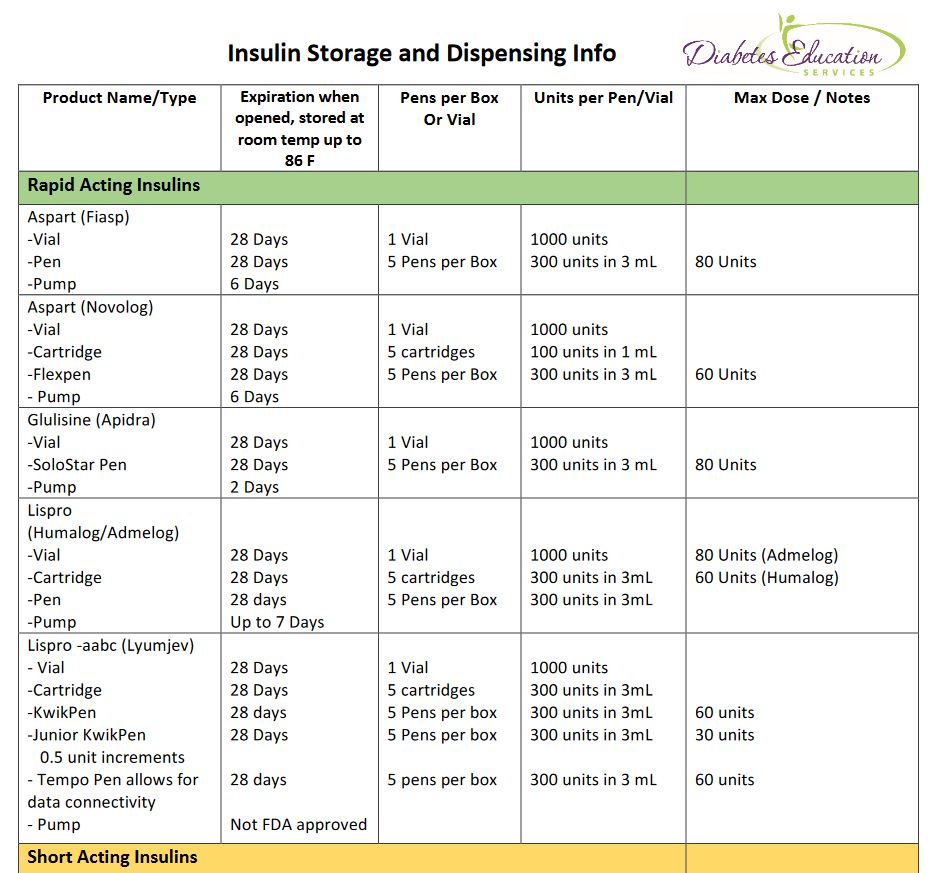
By knowing how long different insulin formulations last when kept at room temperature (temps up to 86 degrees), we can help people use their insulin as long as it is safe and recommended.
We usually say insulin is good for about 28 days. This is correct for many insulins, but not all.
For example, a vial of Human Regular insulin is good at room temp for 42 days. Degludec (Tresiba) is good for 56 days and Novolin 70/30 vial is good for 42 days. Glulisine (Apidra) expires after 2 days in an insulin pump, but lasts for 28 days in a vial.
See our new and exciting Insulin Storage Cheat Sheet for all kinds of important details on storage and more!
In addition, did you know that there are 3 insulins that do not require a prescription in most states? Regular, NPH and Regular/NPH combo insulins require no prescription.
A recent client ran out of their aspart insulin, was low on cash and out of town. They walked into a local Walmart, without a prescription, and paid $25 cash for a vial of regular insulin. This is incredibly important information to share with clients as a back up in case of emergency.
How many times have you launched into a google search or scoured insulin package inserts to find out the following questions or something like it?
Our Insulin Storage Cheat Sheet answers these questions and more!
Special thanks to Jackson Thomassian for compiling the first drafts of these sheets and to Diana Isaacs, PharmD for her inspiration.
Even though Coach Beverly has reviewed and edited these sheets dozens of times, she knows there is always room for improvement. Please let us know if you see content that needs updating. In appreciation, Beverly

AL was recently started on an insulin pump. AL’s insurance company will only cover glulisine (Apidra) insulin for the pump. Before starting pump therapy, AL thought they only needed to change the pump site every three days. AL is frustrated to find out that since they are using glulisine (Apidra), they will need to change the insulin cartridge and site every 2 days.
What is the best solution to AJ’s frustration?
Click here to test your knowledge!
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions, and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Enroll Now!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.