
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Click here to read our entire April Newsletter

At a local hospital, a person in their mid-40s, with type 2 diabetes was admitted for treatment of COVID-19 and Diabetes Ketoacidosis (DKA). An insulin drip was started and their SGLT-2 Inhibitor was stopped. Why are people with type 2 and COVID-19 going into DKA and how is this impacting outcomes?
A person with type 1 diabetes calls into a rural health clinic and says they are running a temperature, having difficulty breathing and can’t get their blood sugars below 300. The diabetes specialist instructs them to go to the hospital. What supplies should they take in case they are admitted to the hospital?
How do we help prepare people with diabetes for the possibility of hospitalization and what are best practices to care for people with diabetes and COVID-19 in the hospital setting?
What instruction do we provide for people with diabetes if they get sick and are wondering if they need to go to the hospital?
In this newsletter, our goal is to answer these questions based on the opinions of experts in the field and the best information to date.
In addition, we are excited to share information on drone delivery of insulin, mask making and the opportunity to celebrate the AADE (ADCES) Educator of the Year, Dr. Diana Isaacs.
Lastly, please let CMS (Medicare) know that RNs and Pharmacists need to be considered as providers of DSME telehealth services. Now, more than ever, we need all hands on deck.
Thank you everyone. Take extra good care of yourselves.
Beverly
Click here to read our entire April Newsletter
Hopeful news.

DPP-4 inhibitors may contribute to a lowered risk and progression of acute respiratory complications for people with type 2 diabetes and COVID-19.
According to commentary in Diabetes Research and Clinical Practice, Endocrinologist Gianluca Iacobellis, MD, Ph.D. suggests that DPP-4 inhibitors could help decrease COVID-19-related immune overreaction in people with diabetes. This immune system calming is due to DPP-IVs anti-inflammatory effects.
All told, DPP-4 “may represent a potential target for preventing and reducing the risk and the progression of the acute respiratory complications that Type 2 diabetes may add to the COVID-19 infection,” Iacobellis wrote in his article.
Based on data from the Chinese city of Wuhan and Italy, people with type 2 diabetes are at higher risk of serious disease in the current pandemic. The data indicates that people with diabetes have accounted for a large proportion of intensive care admission and deaths related to COVID-19.
“The body is overreacting with this inflammatory response to the virus,” Dr. Iacobellis said in a statement. “This could be partially mediated by DPP-4. The virus binds to the enzyme and the enzymatic activity of DPP4 overexpresses inflammatory cytokines, exaggerating the inflammatory response.”
Read more FierceBiotech
The COVID Pandemic is taking a toll on people with diabetes. What is the critical information Diabetes Care and Education Specialists need as we navigate this pandemic? How can take a leadership role in providing sound recommendations while helping to manage the full range of diabetes issues, including hypertension, hyperlipidemia, and cardiovascular risk reduction?

Coach Beverly has created this four-session virtual course so that participants can delve deep into the topics that are most pressing for diabetes care now and in the future. We will focus on improving population health and then drill down to individual intervention through case studies. We will discuss implementing cardiovascular risk screening and treatment in the clinical setting and more!
Session 1 – Getting to the Heart of Care – 1.5 CEs – Airs April 23rd
Session 2 – Cardiovascular Risk Reduction Strategies – 1.5 CEs – Airs April 24th
Session 3 – Lower Extremity Assessment and Intervention – 1.5 CEs – Airs April 28th
Session 4 – Making meaningful Connections and a Vision for the Future – 1.5 CEs – Airs April 30th
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
During this pandemic, many people with diabetes are feeling extra stress. During telehealth visits, they are sharing feelings of discouragement and disappointment as they struggle with social distancing, limited food choices and big disruptions in their usual daily schedule. This disruption is reflected in blood sugars and shifts in body weight.
This moment of discouragement and despair provides an opportunity for diabetes specialist to listen compassionately and help with problem solving.
We can remind them that having diabetes is not their fault and no one can do it perfectly. By modeling kindness and understanding, we can encourage them to be a kinder self-coach from this day forward.
People with diabetes often feel judged by others, including providers, family, friends and even sometimes by members of the diabetes team.
When we provide the gift of “non-judgment” we can help open unexpected doors of insight and understanding. In my experience, people with diabetes are already hard enough on themselves. Meeting them in the field of understanding and compassion can provide them with the courage and belief that they can start rewriting their journey.
Join our Free webinar on Language and Diabetes to further explore this topic.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
The world’s first drone delivery of insulin may be a useful model in response to the COVID-19 pandemic.
For people in rural, remote and isolated urban areas, using a drone to deliver much-needed insulin supplies is an option under consideration. A test flight in Ireland used a drone to deliver insulin as a response to people who were stranded without insulin during Hurricane Ophelia and the post-winter storm Emma when people were snowed in.
“Drone delivery has endless possibilities and can help us connect with our patient communities even in the most remote areas during sentinel events such as hurricanes, earthquakes, and pandemics, which have unfortunately become more common,” Spyridoula Maraka, MD, MS told Healio/Endo.
Though drone delivery has endless possibilities, there are also significant regulatory challenges with “aviation, medication dispensing, pharmaceutical dispensing, and cold chain protocols,” that had to be accounted for during this test run. Markara explains that through each phase of the mission, they had to have backup procedures in place.
Even with the obstacles for drone delivery of insulin or life-saving medications, this is an innovative and exciting prospect for people living in remote or isolated areas.
During the current pandemic, endocrinologists and care providers encourage people that use insulin to have enough stores at home for prolonged “Stay At Home” orders. As stated in our recent Question of the Week people with diabetes are not necessarily at increased risk for contracting COVID-19, but are at risk for experiencing worse outcomes and series complications from the virus (click here to review ADA’s Treatment & Care Factsheet). People living with diabetes may also experience a compromised immune system if blood glucose levels are running above target for a prolonged amount of time.
For these reasons, it is of utmost importance to have the necessary supplies and insulin one needs for optimal glucose levels during periods of crisis, like a pandemic.
To read more, click here and here for more valuable information regarding staying prepared in the pandemic with your insulin and diabetes supplies.
Written by Catherine Cullinane RN, CDCES, our resident Tech Thursday Content Writer
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]BT has had type 1 diabetes for 12 years and is complaining of feeling full and sometimes nauseated after meals, especially after consuming salads.
Which of the following conditions is BT most likely experiencing?
Click here to test your knowledge!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Our April 31st Question of the week was a question about aerobics, hypothyroidism, cholesterol, and type 2 diabetes. Although 58% of respondents chose the correct answer, 42% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
You are working with KS, a 57-year-old with type 2 diabetes, who wants to join the water aerobics program at their local YMCA. KS has a history of hypothyroidism and has an LDL cholesterol of 98 mg/dl. KS’s medications include levothyroxine and metformin XR 1000 mg BID.
According to the ADA and the American College of Sports Medicine, what would be the best recommendation?
Answer Choices:
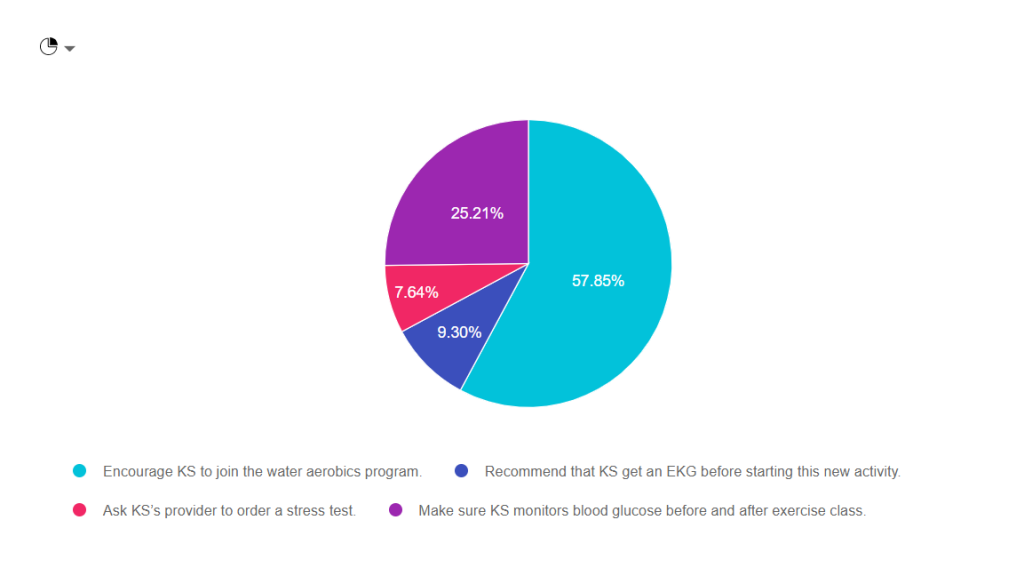
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.

Answer 1 is Correct! Encourage KS to join the water aerobics program. Based on the information provided, she would benefit from adding activity to her routine. Exercise decreases visceral adiposity, improves mood, lower glucose by enhancing insulin sensitivity. See our Exercise Resource Page for helpful info.
Answer 2 is incorrect. About 10% of respondents chose “Recommend that KS get an EKG before starting this new activity.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting an EKG for those with risk factors for cardiovascular events.
Answer 3 is also incorrect. About 10% of respondents chose “Ask KS’s provider to order a stress test.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting a stress test for those with risk factors or symptoms of cardiovascular events.
Finally, Answer 4 is incorrect. “Make sure KS monitors blood glucose before and after exercise class.” Having diabetes is a lot of work. As diabetes specialists, it is important that we don’t unnecessarily increase the burden of daily self-care. While KS may gain interesting information by checking BG levels before and after exercise, it is NOT necessary to monitor glucose before and after.
Why not? Since KS is not on any medication that causes hypoglycemia, her risk of low blood sugar is almost none. In addition, most people on oral medications are only allotted one strip a day to monitor blood sugars. Asking KS to check twice on water aerobics days may translate to extra out of pocket expenses that can also add to the financial burden of diabetes.
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
Pre-exercise Evaluation- 2020 Standards Of Care
The ADA consensus report “Screening for Coronary Artery Disease in Patients With Diabetes” (172) concluded that routine testing is not recommended. However, providers should perform a careful history, assess cardiovascular risk factors, and be aware of the atypical presentation of coronary artery disease in patients with diabetes. Certainly, high-risk patients should be encouraged to start with short periods of low-intensity exercise and slowly increase the intensity and duration as tolerated. Providers should assess patients for conditions that might contraindicate certain types of exercise or predispose to injury, such as uncontrolled hypertension, untreated proliferative retinopathy, autonomic neuropathy, peripheral neuropathy, and a history of foot ulcers or Charcot foot. The patient’s age and previous physical activity level should be considered. The provider should customize the exercise regimen to the individual’s needs. Those with complications may require a more thorough evaluation prior to beginning an exercise program (171).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Our March 31st Question of the week was a question about COVID-19, sick days and diabetes. Although 40% of respondents chose the correct answer, 60% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
JR is 27 with Type 1 diabetes and is very worried about getting COVID-19 since they work in a local grocery store. They ask you what they should do if they get COVID-19?
Which of the following statements is accurate regarding sick day management with COVID-19?
Answer Choices:
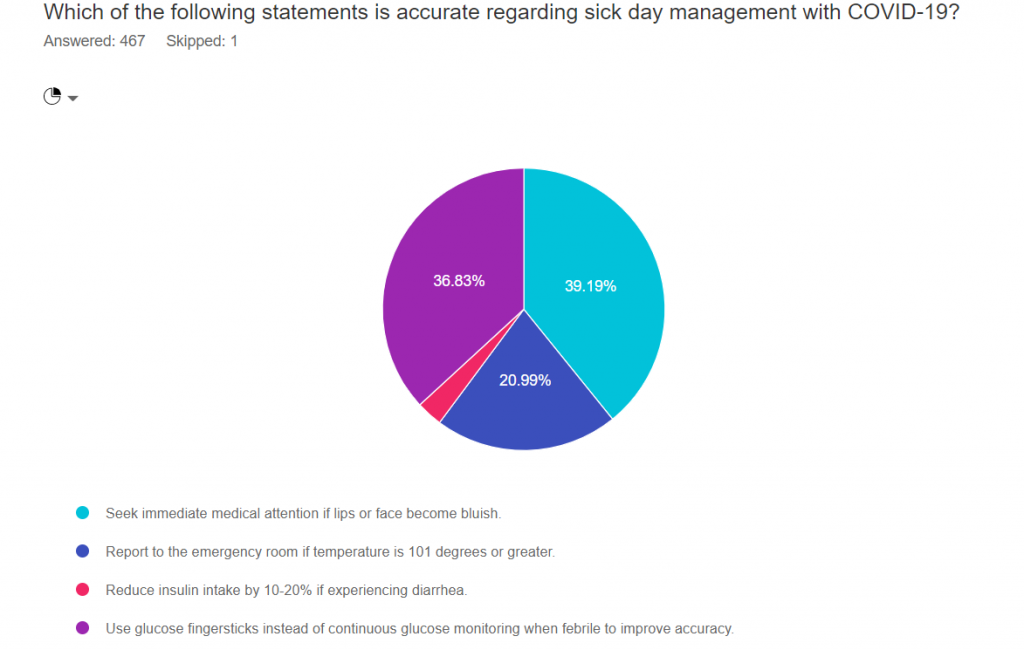
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.
Only 39% of participants chose the correct answer number 3, which means there is a learning opportunity!
Answer 1 is Correct! Seek immediate medical attention if lips or face become bluish. Bluish lips or face indicates hypoxia and signals urgent medical care is needed.
From ADA Sick Day Information. If develop emergency warning signs for COVID-19 get medical attention immediately.
In adults, emergency warning signs include:
Option 2 is incorrect. One-fifth of respondents chose ” Report to the emergency room if the temperature is 101 degrees or greater.” In the case of fever, the next step would to be to contact your provider to evaluate presence of cough, shortness of breath and other symptoms to determine if urgent care is required.
Option 3 is also incorrect. “Reduce insulin intake by 10-20% if experiencing diarrhea.” During periods of illness, inflammation leads to insulin resistance and hyperglycemia. Most people will need to increase insulin dose during illness, including GI distress.
Finally, Option 4 is incorrect. “Use glucose fingersticks instead of continuous glucose monitoring when febrile to improve accuracy.”
Fever by itself does not interfere with CGM accuracy. If a person is taking Tylenol, it can interfere with the accuracy certain CGMs. And, CGM use is not recommended in the Intensive Care setting. But, having a temperature by itself, does not interfere with CGM accuracy.
Here is a COVID and Sick Day Handout that you can share with your community. Thank you for helping us get the word out.
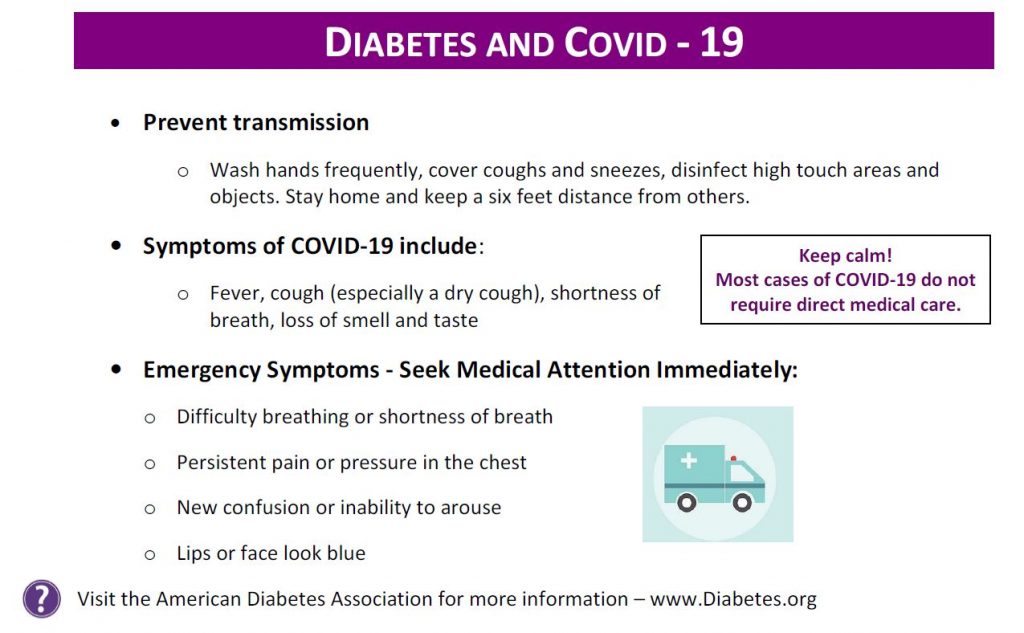
For more information on sick day management and when to seek medical care, please see this ADA Sick Day Information.
We hope you appreciate this week’s rationale and keep studying hard! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
A Belgian study shows that intermittently scanned CGMs (isCGM) can reduce episodes of hypoglycemia and diabetes-related hospital visits in people with type 1 diabetes which can improve or stabilize their quality of life.
In this study conducted by Pieter Gillard, MD, Ph.D., the assistant head of the clinic in the department of endocrinology at University Hospitals Leuven and associate professor at the University of Leuven and colleagues, they reviewed episodes of hypoglycemia, DKA and A1c levels and quality of life measures in a study of 1,913 adult patients with type 1 diabetes.

There were decreases noted in hypoglycemia, DKA, diabetes-related hospital visits, and work sick days. The “quality of life” measures were noted as “overall stable;” A1c levels did not appear to reflect any changes in study participants.
Users of isCGM rated the system as much more convenient than fingerstick glucose testing. Although A1c levels did not change, people using isCGM had greater satisfaction in managing their diabetes.
“Patients prefer to use isCGM compared to fingersticks” – Anne Peters, MD, Director, USC Clinical Diabetes Program
Using an “isCGM” can be helpful for clinicians, CDCES, nurses, and patients in reviewing BG levels stored within the isCGM device.
Click here for more information.
Written by Catherine Cullinane RN, CDCES, our resident Tech Thursday Content Writer
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]