
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

JT, a 17-year-old recently hospitalized with a new diagnosis of type 1 diabetes, is using Multiple Daily Injections (MDI) therapy. JT uses fingerstick blood glucose monitoring but wants to move to a CGM. JT’s mother wants to know how long fingerstick monitoring must be used before a CGM can be started. According to the ADA 2025 Standards of Care, when can a CGM be initiated after a type 1 diabetes diagnosis?

Gain confidence in interpreting the Glucose Profile Report (AGP) & CGM data using a
person-centered approach
As diabetes technology is becoming commonplace in our practice, figuring out how to make sense of all the data can seem overwhelming. Join Diana Issacs and Coach Beverly for a truly unique learning experience.
Topics include:
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
C.K. is a 55-year-old elementary school teacher diagnosed with type 1 diabetes ten years ago and is managing glycemic control with multiple daily injections (MDI) and a CGM. You are seeing C.K. for diabetes education due to an increasing hemoglobin A1c from 7.0% to 9.9%. During the appointment, C.K. reports missing mealtime doses due to being “too busy to get all that stuff out” at both work and home. C.K. notes that a friend from church has an insulin pump and asks if an insulin pump would help improve their A1c.
As the diabetes care and education specialist, what factors do you need to assess before determining if C.K. is ready for insulin pump therapy?
Join us live October 22nd – 23rd, 2025!
30+ CEs with Expanded Accreditation!


Join our expert team for engaging, interactive sessions that bring the ADA Standards of Care to life—covering medications, behavior change, technology, and more. Ideal for CDCES or BC-ADM exam prep, this course also includes a 4-hour Virtual Medical Nutrition Therapy Toolkit and bonus content that also meets CDCES renewal requirements.
Upon completion of this activity, participants should be able to:

Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES

Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun!
Program Faculty Disclosures:
Partners for Advancing Clinical Education (Partners) requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated according to Partners policies. Others involved in the planning of this activity have no relevant financial relationships.
Faculy Bios & Disclosures:
 Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd Services
Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd ServicesDisclosures:
Beverly Thomassian has no financial disclosures
Bio:
 Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Disclosures:
Dr. Diana Isaacs has the following relevant financial relationships:
Bio:
Diana Isaacs was awarded 2020 ADCES Diabetes Educator of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She serves in leadership roles for several pharmacies and diabetes organizations. She has numerous diabetes publications and research projects with a focus on medications, CGM and diabetes technology.
For the past three year, Dr. Isaacs has served as a contributing author for the 2023 ADA Standards of Care.
As the Program Coordinator and clinical pharmacist specialist in the Cleveland Clinic Diabetes Center, Dr. Isaacs brings a wealth of clinical knowledge combined with extensive research and speaking experience to this program.
Activity Start and End Date: 10/22/25 – 10/23/2025
Estimated time to complete the activity: 15 hours and 30 minutes
_____________________________________
Jointly provided by Partners for Advancing Clinical Education and Diabetes Education Services
![]()
![]()
Joint Accreditation Statement:
![]() In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Physician Continuing Education:
Partners designates this enduring material for a maximum of 15.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nursing Continuing Professional Development:
The maximum number of hours awarded for this Nursing Continuing Professional Development activity is 15.50 contact hours.
Pharmacy Continuing Education:
Partners designates this continuing education activity for 15.50 contact hour(s) (1.550 CEUs) of the Accreditation Council for Pharmacy Education.
(Universal Activity Number – JA4008073-9999-25-206-L01-P)
Type of Activity: Application
For Pharmacists: Upon successfully completing the activity evaluation form, transcript information will be sent to the NABP CPE Monitor Service within 4 weeks.
Dietitian Continuing Education:
This program offers 15.50 CPEUs for dietitians.
Interprofessional Continuing Education:
![]() This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
For additional information about the accreditation of this activity, please visit https://partnersed.com.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on ADA 2025: Which MNT Statement Is False? 50% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Question: According to the 2025 ADA Standards of Care, which of the following statements about medical nutrition therapy (MNT) for adults with type 2 diabetes is NOT TRUE?
Answer Choices:
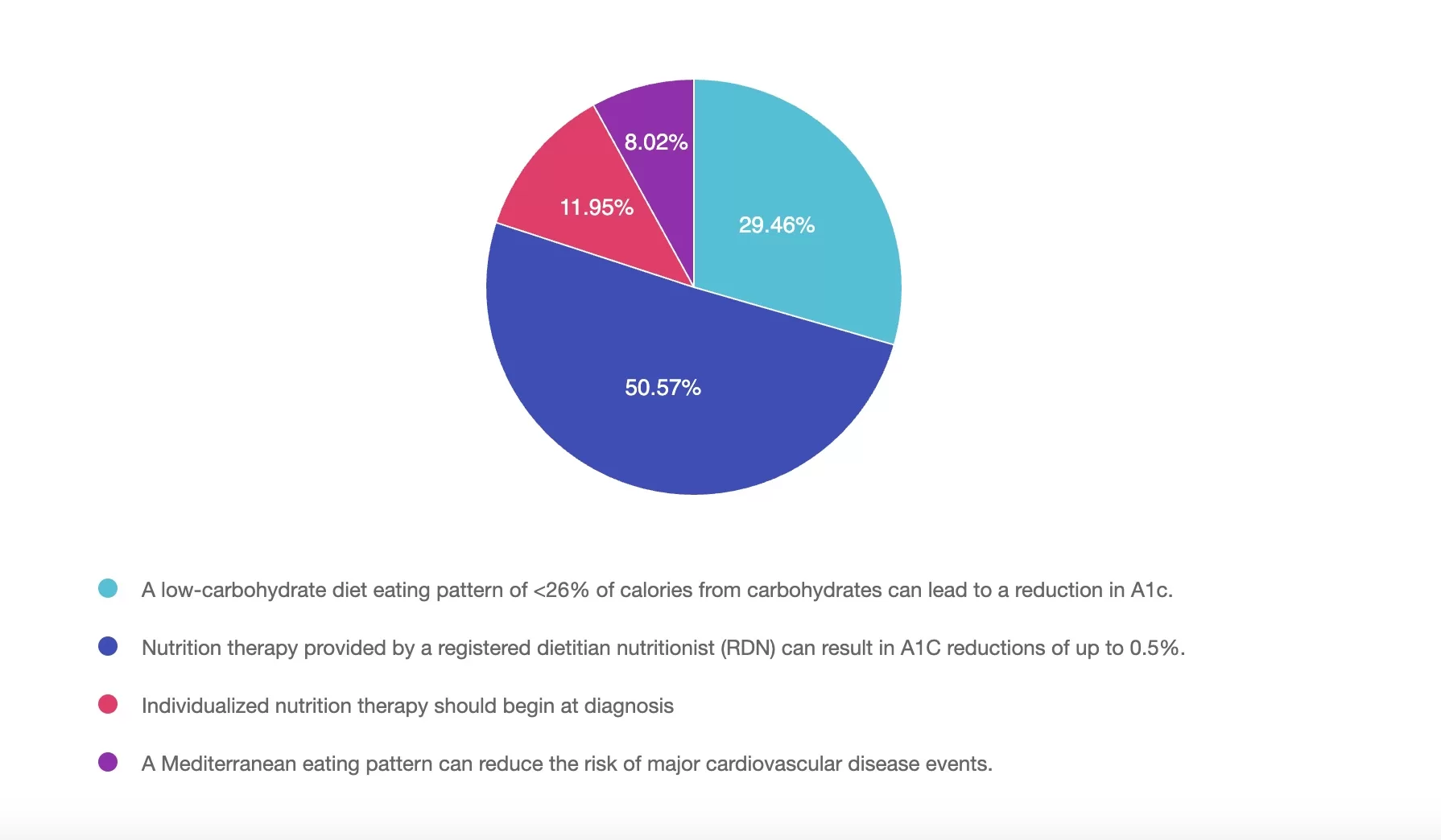
Answer 1 is incorrect. 29% chose this answer, “A low-carbohydrate diet eating pattern of <26% of calories from carbohydrates can lead to a reduction in A1c.” Low-carbohydrate eating patterns (defined as <26% of calories from carbohydrates) have been shown to lower A1C in adults with type 2 diabetes and are supported by the 2025 ADA Standards of Care as one of several individualized eating patterns.
Answer 2 is correct. 50% of you chose this answer, “Nutrition therapy provided by a registered dietitian nutritionist (RDN) can result in A1C reductions of up to 0.5%.” The 2025 ADA Standards of Care state that medical nutrition therapy (MNT) provided by an RDN can lead to A1C reductions of 0.3% to 2%, especially in individuals with type 2 diabetes. The answer is not true because a 0.5% reduction underestimates the potential benefit.
Answer 3 is incorrect. About 11% of respondents chose this, “Individualized nutrition therapy should begin at diagnosis.” The ADA recommends that individualized MNT should be initiated at the time of diagnosis. Additional times for referral include annually or when not meeting treatment goals, when complications occur or when transitions in life occur.
Finally, Answer 4 is incorrect. 8% chose this answer, “A Mediterranean eating pattern can reduce the risk of major cardiovascular disease events.” The Mediterranean eating pattern has been associated with improved glycemic control and a reduced risk of cardiovascular events, making it an eating pattern to consider for people with type 2 diabetes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Join us live on June 5, 2025, at 11:30 am PST to watch our brand new webinar, Weight-Inclusive Diabetes Care: Turning Compassion into Practical Tools by Jessica Jones, MS, RDN, CDCES
This session provides healthcare providers with actionable strategies to integrate weight-inclusive care into diabetes management practices, focusing on improving outcomes through respect for body diversity and individual autonomy. Weight stigma is a well-documented barrier to effective care, contributing to poorer glycemic control, disordered eating, and care avoidance. By shifting from a weight-focused approach to one aligned with Health at Every Size (HAES®), providers can foster trust, enhance participant engagement, and support sustainable health behaviors.
Jessica Jones, MS, RD, CDCES, will share evidence-based insights on mitigating weight stigma and applying HAES-aligned strategies in practice. Participants will learn how to build rapport, set realistic nutrition goals, and implement interventions that prioritize blood sugar management, joyful movement, and intuitive eating. This session equips providers with tools to deliver compassionate, person-centered care, improving both clinical outcomes and the provider-participant relationship.
Course topics:
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Walking is often recognized as the most accessible and underrated form of exercise. While some may argue in favor of high-intensity cardio or resistance training, a growing body of evidence suggests that walking offers significant benefits—especially when approached with intention and consistency.
According to Dr. Elroy Aguiar, an assistant professor of exercise science at The University of Alabama, walking remains one of the most beneficial forms of movement due to its low barriers to entry—minimal cost, equipment, or skill required. “That’s why we say it’s the best,” Dr. Aguiar notes. And yet, despite this accessibility, many individuals struggle to find time to incorporate walking into their busy, sedentary lives.

Not all walking provides the same health return. The intensity, particularly cadence (steps per minute), plays a crucial role in determining health outcomes.
🕒 100 steps per minute is considered moderate intensity
⚡ 130 steps per minute qualifies as vigorous intensity
Dr. Aguiar’s research, published in the British Journal of Sports Medicine, indicates that health benefits from walking begin to accumulate at moderate or higher intensities. Most people naturally walk at a pace of 110–115 steps per minute when moving briskly. Increasing cadence just slightly can shift the effort from moderate to vigorous, maximizing the health payoff in a shorter time span.
For those looking to increase the challenge of walking, rucking—walking with a weighted backpack—offers a practical solution.
Adding resistance increases oxygen demand, raises heart rate, and enhances caloric burn without requiring a change in pace or duration. According to Dr. Aguiar, this method can also improve lower body strength and bone density, particularly with consistent practice over time.
While it won’t replace traditional strength training, rucking offers an accessible way to gain some muscular benefits while walking. A light weight to start, gradually increased, can help prevent injury and support adaptation.
A 2024 study published in the Scandinavian Journal of Medicine and Science in Sports found that both the quantity and intensity of physical activity are associated with better health outcomes. Remarkably, even one minute of higher-intensity activity per day was linked to a lower likelihood of having metabolic syndrome—a cluster of risk factors including visceral adiposity, high blood pressure, high blood sugar, low HDL cholesterol, and elevated triglycerides.
Dr. Aguiar explains that an individual’s most intense one-minute activity across the day can serve as a strong indicator of metabolic health. Even brief, high-intensity bursts of activity may help reduce risk for diabetes, hypertension, and cardiovascular disease.
Another practical strategy supported by research is post-meal walking. A 15-minute walk after meals can help blunt spikes in blood glucose, particularly in older adults at risk for glucose intolerance.
When muscles are active, they draw glucose from the bloodstream to use for energy, thereby reducing blood sugar levels and easing the demand on insulin. Over time, this can help prevent insulin resistance, a precursor to Type 2 diabetes.
Dr. Aguiar notes that consistent post-meal movement can reduce the workload on the pancreas and enhance the muscles’ ability to absorb and use glucose. This daily practice may offer long-term protection against metabolic syndrome, hypertension, and diabetes.
Large-scale studies have shown clear associations between step count and mortality risk. A 2023 meta-analysis published in the European Journal of Preventive Cardiology found:
Additionally, a study by the University of Granada concluded that while more steps bring more benefits, the majority of cardiovascular protection appears to occur around 7,000 steps/day. The popular goal of 10,000 steps per day, while not evidence-based, remains a useful motivational benchmark.
For elite athletes, walking may offer limited fitness returns. However, for individuals who are sedentary or new to exercise, walking provides a low-impact, effective entry point to better health.
Some key benefits of walking for the general population include:
Walking is especially valuable for individuals managing or at risk for Type 2 diabetes, obesity, hypertension, and metabolic syndrome.
Walking delivers significant, sustainable health benefits with minimal risk
Walking is a powerful yet underappreciated form of movement. Whether used to regulate blood sugar, reduce cardiovascular risk, or improve mental clarity, walking remains one of the most effective and inclusive health strategies available.
For anyone looking to improve overall health without the barriers of cost, complexity, or time—walking offers a proven path forward.
📚 References
Gain confidence in interpreting Glucose Profile Report (AGP) & CGM data using a person-centered approach! Earn 4.0 CEs
If you are preparing for certification exams or want to up your game using CGM data to improve outcomes, this course is for you.
1:30am to 2:30pm PST
Gain confidence in interpreting Glucose Profile Report (AGP) & CGM data using a person-centered approach.
As diabetes technology is becoming commonplace in our practice, figuring out how to make sense of all the data can seem overwhelming. Join Diana Issacs and Coach Beverly for a truly unique learning experience.
Dr. Isaacs has a special knack for breaking down the essential elements of the Ambulatory Glucose Profile (AGP) report to provide participants with a clear road map for data interpretation. She includes many sample practice cases utilizing CGM data for various types of people with diabetes including type 2 and people with type 1 not on pumps.
Coach Beverly will build on Dr. Isaacs’ presentation and switch the focus to the person living with diabetes. Using a case study approach, she will provide strategies to integrate the AGP with person-centered care that empowers individuals to experience increased confidence in their diabetes self-management.
By attending this interactive workshop, participants will become more confident in interpreting the AGP and continuous glucose monitor (CGM) data and determining needed medication and lifestyle adjustments with a person-centered approach.
Topics include:
Review CGM key metrics and individualize time in-range goals
Learn how to recognize patterns with the AGP report efficiently
Utilize the AGP report as a discussion guide when meeting with a person with diabetes
Recommend lifestyle and medication adjustments based on CGM data
Strategies to recognize the expertise of the individual and collaborate on person-centered problem solving.
A 10-year-old child with newly diagnosed type 1 diabetes is being discharged from the hospital. Which of the following components is most critical to include in the initial outpatient diabetes management plan to reduce the risk of diabetic ketoacidosis (DKA) and hospital readmission?
This course includes updated goals & guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes & their families. We discuss the clinical presentation of diabetes, goals of care, & normal growth & development through the early years through adolescence. Strategies to prevent acute & long-term complications are included with an emphasis on positive coping for families & children with diabetes.
Objectives:
For last week’s practice question, we quizzed participants on How Well Do You Know Coach Bev? 33% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Which early job taught Coach Beverly the value of loving your work and providing excellent service?
Answer Choices:
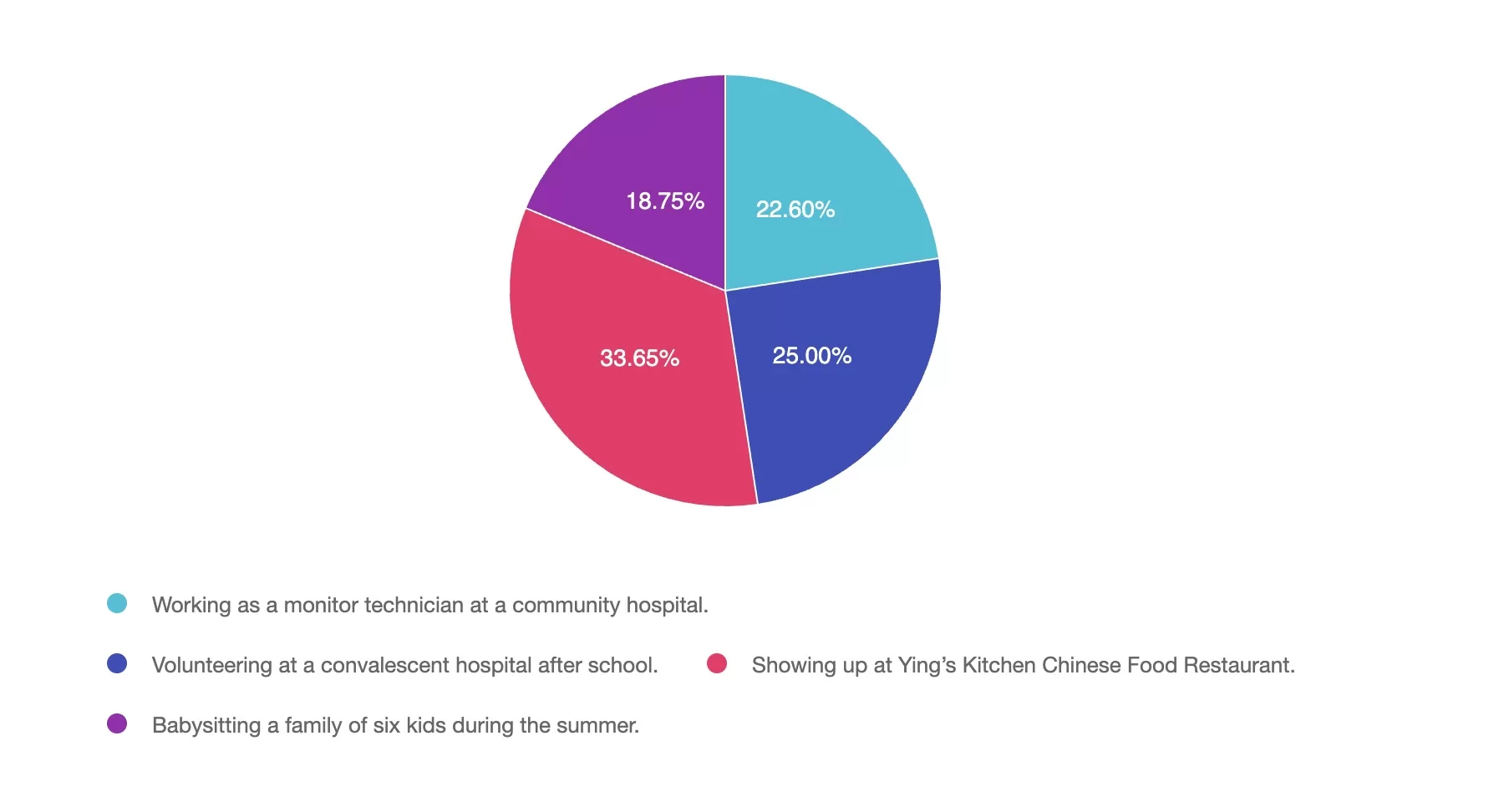
Answer 1 is incorrect. 22% chose this answer, “Working as a monitor technician at a community hospital.” Beverly worked as a monitor tech and nurses aide at a community hospital while attending nursing school. These experiences taught her about navigating medical terminology and hospital systems.
Answer 2 is incorrect. 25% of you chose this answer, “Volunteering at a convalescent hospital after school.” Coach Bev did lead Bingo games and play guitar at a convalesent home after school. She loved connecting with older adults and hearing their stories.
Answer 3 is correct. About 33% of respondents chose this, “Showing up at Ying’s Kitchen Chinese Food Restaurant.” This is the best answer. Her 8 years at Ying’s Kitchen taught her about hard work, attention to detail, and loving what you do.
Finally, Answer 4 is incorrect. 18% chose this answer, “Babysitting a family of six kids during the summer.” Watching 6 kids over the summer helped her recognize that being a parent has lots of perks, but she wasn’t ready.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
According to the 2025 ADA Standards of Care, which of the following statements about medical nutrition therapy (MNT) for adults with type 2 diabetes is NOT TRUE?
This four-hour course highlights the latest ADA evidence-based nutrition and exercise guidelines. Our nutrition expert, Christine Craig, MS, RD, CDCES, provides strategies to apply this important information to individuals living with diabetes. She includes in-depth discussions on different approaches to person-centered meal planning and the benefits and limitations of each. If you are getting ready to take your diabetes certification exam, this course provides essential content for exam success.
Topics addressed by Christine Craig, MS, RD, CDCES
-Medical Nutrition Therapy Updates and Critical Content
-Describe person-centered nutrition issues based on assessment and clinic data.
-Explore national guidelines for medical nutrition therapy and how to individualize interventions from a person-centered perspective.
-State how to customize nutritional approaches in people living with complications of diabetes.
-How to Eat by the Numbers and Meal Planning Approaches
-Describe the impact of micro and macronutrients on health.
-List different meal planning approaches and the pros and cons of each.
-Describe how to help people with diabetes to read labels and be thoughtful consumers.
-Keeping Well Through Activity and Nutrition
-Describe activity benefits, precautions, and recommendations
Fee: $69.00/ 4.25 CEs
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on Decoding AGP Report-Test Your Knowledge. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AJ asks you why their blood glucose levels are “all over the place”. When you look at the AGP, you notice the coefficient of variation is 26%. What is the best response?
Answer Choices:
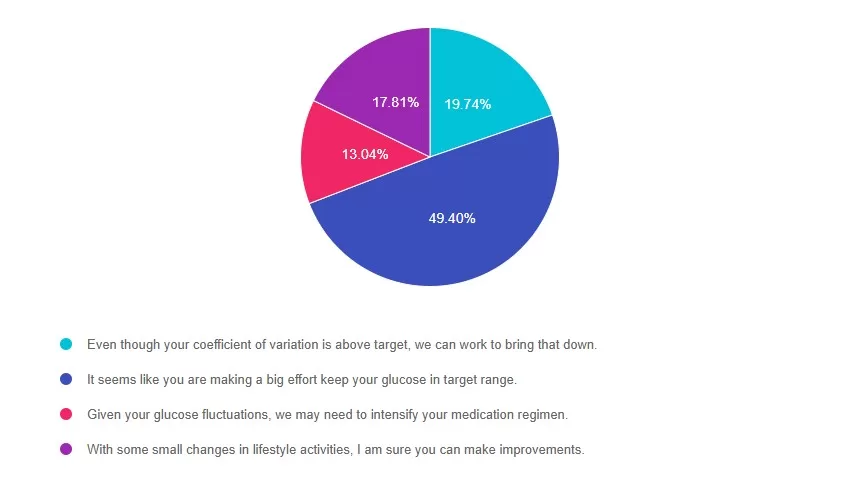
Answer 1 is incorrect. 19% chose this answer, “Even though your coefficient of variation is above target, we can work to bring that down.” According to ADA Standards, the goal for glucose variability (or coefficient of variation) is less than 36%. AJ has a coefficient of variation of 26%, which is significantly below the target. This is a wonderful opportunity to recognize AJ’s self-management efforts.
Answer 2 is correct. 49% of you chose this answer, “It seems like you are making a big effort keep your glucose in target range.” YES, this is the BEST Answer. AJ has a coefficient of variation of 26%. That is 10% below the target of 36%. This is a wonderful opportunity to recognize AJ’s self-management efforts.
Answer 3 is incorrect. About 13% of respondents chose this, “Given your glucose fluctuations, we may need to intensify your medication regimen.” According to ADA Standards, the goal for glucose variability (or coefficient of variation) is less than 36%. AJ has a coefficient of variation of 26%, which is significantly below the target. This is a wonderful opportunity to recognize AJ’s self-management efforts.
Finally, Answer 4 is incorrect. 17% chose this answer, “With some small changes in lifestyle activities, I am sure you can make improvements.” According to ADA Standards, the goal for glucose variability (or coefficient of variation) is less than 36%. AJ has a coefficient of variation of 26%, which is significantly below the target. This is a wonderful opportunity to recognize AJ’s self-management efforts.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Dr. Isaacs has a special knack for breaking down the essential elements of the Ambulatory Glucose Profile (AGP) report to provide participants with a clear road map for data interpretation. She includes many sample practice cases utilizing CGM data for various types of people with diabetes including type 2 and people with type 1 not on pumps.
Topics include:
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.