
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

“I’ve managed my diabetes for years, but ever since starting cancer treatment, my blood glucose has been all over the place. I don’t know what I am doing wrong.”
As diabetes health professionals, our job is to support people through both complex clinical situations and the emotional challenges of living with cancer and diabetes. Having the knowledge to address both can improve engagement, lead to better outcomes, and strengthen relationships with the people we work with.
Diabetes and cancer are no longer just parallel health crises sharing a person’s chart; they are deeply entangled pathologies where hyperglycemia, inflammation and the risk of cancer development are interrelated. For diabetes healthcare professionals, mastering this bidirectional threat no longer falls under the rare case scenario.
As a diabetes professional, you have an important role in detecting sudden hyperglycemia as a result of chemotherapeutic agents, like checkpoint inhibitors and PI3k inhibitors. In addition, you can encourage people with diabetes to engage in regular cancer screenings and be aware of reportable symptoms. This is an immediate, high-stakes clinical mandate that can improve prompt treatment and detect cancer earlier.
The shared risk factors between type 2 diabetes and cancer (older age, elevated body weight, and lack of physical activity) increase this bidirectional association, but diabetes-related factors such as underlying disease physiology or diabetes treatments may also increase this cancer-diabetes connection.
One of the most clinically actionable areas of recent research highlights the relationship between a new diabetes diagnosis and pancreatic and other cancers.
People with type 2 diabetes face about twice the risk of developing pancreatic cancer compared to those without the condition, while an older adult (over 50) with new-onset diabetes experiences a sharper increase in risk within the first few years.
New onset of atypical diabetes (lean body habitus and negative family history) in a middle-aged or older person may precede the diagnosis of pancreatic adenocarcinoma. Additionally, in a nationwide cancer registry in New Zealand, post pancreatitis diabetes mellitus was associated with significantly higher risk (2.4-fold) of pancreatic cancer compared with pancreatitis after type 2 diabetes. (ADA).
Diabetes is associated with increased risk of cancers of the liver, pancreas, endometrium, colon and rectum, breast, and bladder.
Large-scale cohort analyses reveal that individuals with diabetes face a roughly doubled risk of developing
There are also notable 1.2- to 1.5-fold increases in:
People with diabetes are encouraged to schedule recommended age-and sex-appropriate cancer screenings, coordinated with their primary health care professional. As diabetes professionals, you can encourage individuals to take action and to reduce their modifiable cancer risk factors. Actions that help with diabetes management also reduce risk of cancer including:
The cancer frontier of oncology has been revolutionized by precision therapies, but these life-saving advancements can come with steep glucose elevations due to beta cell disruption.
Hyperglycemia due to chemotherapy may either be transient (improving upon treatment cessation) or represent permanent diabetes.
Immune checkpoint inhibitors are used to treat many types of cancer, such as melanoma, non-small cell lung cancer, bladder cancer, renal cell carcinoma, breast cancer, and Hodgkin lymphoma.
Common immune checkpoint inhibitors include: pembrolizumab (Keytruda), nivolumab (Opdivo), ipilimumab (Yervoy), durvalumab (Imfinzi), atezolizumab (Tecentriq).
The most likely Immune checkpoint inhibitors that rigger rapid, autoimmune-mediated destruction of beta cells include:
Insulin therapy is the cornerstone of management, as individuals typically present with rapid-onset, severe hyperglycemia or DKA. Many will initially need an insulin drip, followed by the implementation of basal bolus insulin therapy along with continuous glucose monitoring.
PI3K inhibitors are used primarily to treat advanced breast cancer (specifically HR+/HER2- tumors with PIK3CA mutations) and blood cancers (such as lymphomas, leukemias, and follicular lymphoma).
Phosphatidylinositol 3-kinase (PI3K) inhibitors are small molecules designed to disrupt intracellular signaling pathways, thereby inhibiting cancer cell growth and survival. Within this class, targeted inhibition of the alpha isoform (PI3Kα) disrupts downstream insulin receptor signaling, frequently resulting in profound, on-target hyperglycemia and acute insulin resistance.
Which PI3K medications are associated with glucose elevations?
These two types of PI3Kα inhibitors have a 60% incidence of causing hyperglycemia, typically appearing within the first 2 weeks of therapy.
People at increased risk of hyperglycemia from PI3K inhibitor therapy include those with:
Glucose management is crucial since significant hyperglycemia can lead to discontinuation and/or reduction in PI3K medication dose, which can decrease therapy efficacy.
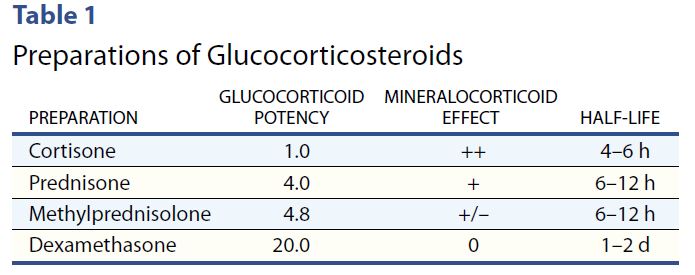
Cancer treatment often includes concurrent steroid therapy to enhance efficacy. However, steroid therapy can induce or worsen hyperglycemia.
Steroids have their highest potency at 4-12 hours, with the exception of the very potent dexamethasone, which has a half life of 1-2 days.
With morning steroids, including dexamethasone, people will experience elevated glucose values after breakfast, lunch, dinner, and at bedtime but will have a significant drop toward normal glucose overnight.
Therefore, hyperglycemia is greatest 1–2 hours after a meal, with persistent elevation until the following meal, followed by a return to normal overnight.
To treat steroid induced hyperglycemia, NPH. Neutral Protamine Hagedorn (NPH) insulin is an effective treatment choice since it is an intermediate acting basal insulin. NPH insulin is cloudy and has an onset of 1–4 hours. Its peak is 6–10 hours and its duration is about 10–16 hours. Download our Insulin PocketCards.
For individuals on once daily steroids, morning NPH with some bolus insulin can effectively target daytime hyperglycemia. For those taking steroids twice daily, an additional dose of NPH plus bolus as needed, is added at dinnertime.
Join Coach Beverly July 21 at 11:30am to learn more during our Cancer and Diabetes Webinar.
As diabetes professionals, we are stepping into a vital new role at the intersection of metabolic health and oncology. Modern cancer therapies like checkpoint inhibitors and PI3K inhibitors are absolute game-changers for oncology, but they often trigger sudden, severe hyperglycemia that catches patients and healthcare professionals off guard.
That is where our expertise becomes a literal lifesaver. By actively monitoring for sudden hyperglycemia and aggressively championing routine cancer screenings, we are doing so much more than just managing a chronic disease. We are taking on an urgent, high-stakes clinical mandate that ensures patients get immediate treatment when they need it most and catches cancer at its earliest, most treatable stages.
Ultimately, our vigilance bridges the gap between effective cancer therapy and safe metabolic health, directly shaping better, life-saving outcomes for the people in our care.
Explore the unexpected link between cancer and diabetes — and master glucose management strategies for people with diabetes undergoing treatment.
Individuals with cancer often experience hyperglycemia secondary to treatment, which can increase the risk of infection and other complications. Recent research has also identified a significant link between diabetes and cancer. This course uses a case study approach to explore this connection and provide practical strategies for managing steroid-induced hyperglycemia and improving quality of life for people navigating both conditions.
Course Topics:
Every year, National Nurses Week invites us to pause and honor a profession rooted in compassion, resilience, and an unwavering commitment to care.
This Nurses Week, I encourage you to take a moment to appreciate a nursing colleague, friend or family member. Let them know how their care and compassion has made a difference in your life!
As I reflect on my 40 years as a nurse, I feel both humbled and energized by the extraordinary legacy we carry forward. Nursing is not just a career—it is a calling shaped by human connection, scientific curiosity, and the courage to show up, again and again, for people in their most vulnerable moments.

The history of nursing is rich with pioneers who transformed care through both innovation and heart. Florence Nightingale is often recognized as the founder of modern nursing, bringing sanitation and data-driven care to the forefront. But beyond her statistics and systems, she modeled something deeper—the importance of presence. That legacy continues today in every nurse who sits at the bedside, listens without judgment, and advocates fiercely for those in their care.
The observance recognizes the critical role of nurses in patient care, research, leadership, and education. It raises public awareness of the challenges nurses face, such as staffing shortages and workplace stress – and promotes professional pride and public gratitude. The ANA and partner bodies like the American Association of Critical-Care Nurses host webinars, award ceremonies, and advocacy events to spotlight the profession’s impact
Today, nurses represent the largest group of healthcare professionals specializing in diabetes. Nearly half (46%) of those who hold a CDCES credential are nurses. That’s not just a statistic—it’s a reflection of the profound impact nurses have in shaping how diabetes care is delivered, understood, and experienced every day.
In the world of diabetes care, nurses have been at the center of transformation. From the early days of checking urine glucose to administering pork and beef insulin to today’s advanced technologies, nurses have led the way. As early adopters of continuous glucose monitoring and automated insulin delivery systems, nurses have bridged the gap between complex science and real-life application. We are educators, coaches, and translators—helping people make sense of numbers, medications, and daily decisions that can feel overwhelming.
What makes diabetes nursing uniquely powerful, is the ongoing contact nurses often maintain with individuals over a lifetime. Diabetes doesn’t take a day off, and neither does the emotional weight that often accompanies it. In my work, I’ve learned that the most meaningful breakthroughs don’t come from adjusting a medication or starting a CGM, they come from creating a space where someone feels seen, heard, and supported.
Over the decades, I’ve witnessed incredible advancements in diabetes care—new medications, smarter devices, and more personalized approaches. Nurses, along with their colleagues, are often the steady thread in a fragmented healthcare system. We are the ones who notice subtle changes, ask deeper questions, and advocate when something doesn’t feel right. In diabetes care, this might mean recognizing patterns in glucose trends, addressing social determinants of health, or simply acknowledging the burnout a person feels after years of self-management. These moments matter more than we often realize.
As I reflect on my journey, from bedside nursing to education, from rural clinics to national stages – I am continually reminded that our greatest impact comes not from having all the answers, but from presence. The simple act of sitting with someone, validating their experience, and walking alongside them can be profoundly healing – for them and for us. This mutual growth is at the heart of sustainable, meaningful care.
In hospitals, clinics, schools, and beyond – you show up at every hour of the day and night, bringing skill, compassion, and unwavering dedication. You give of yourselves in ways both seen and unseen, helping others heal, receive comfort, and feel cared for in their most vulnerable moments.
National Nurses Week offers us a moment to pause and honor your service and a profession grounded in compassion, resilience, and an unwavering commitment to showing up for others. Thank YOU!
Coach Beverly, RN and author of Healing through Connection for Healthcare Professionals!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access

In honor of Earth Day, April 22, 2026, we’re shining a light on the power of native plants in creating vibrant, resilient ecosystems—for wildlife and for people. See our Earth Day List of Resources Here!
Native plants—those that have evolved naturally in a specific region—play a crucial role in supporting local pollinators, birds, butterflies, and other wildlife. These plants provide essential food, pollen, and shelter that many species rely on for survival. And while the benefits to the environment are clear, cultivating native plants also boosts human well-being. Thriving ecosystems support cleaner air and water, increased biodiversity, and create opportunities for people to reconnect with nature.
When Coach Beverly moved into her home 26 years ago, she planted what many of us do—flowers and grasses that looked appealing and could withstand local heat. With an acre of land surrounding her home and office, she had space to experiment, adding a wide variety of foliage and trees for beauty and shade.
But like many at that time, she wasn’t yet aware of the importance of native plants—or how their presence (or absence) affects the animals, insects, and birds that share our space.
Over time, as she learned more about habitat loss and the plight of pollinators, she began to rethink her approach. Through research, visits to a nearby native nursery, and the help of trusted websites, she and her husband began the transformation: reshaping their land into a space that supports bees, butterflies, frogs, birds, lizards, and more. Today, their yard is not only beautiful but also an oasis for wildlife—and a model of sustainable gardening.
In addition to plants, providing a water source can be a game-changer for thirsty pollinators and wildlife. Whether it’s a birdbath, a shallow dish, or a small pond, water invites life into any garden.
Last year, Coach Beverly dug a small frog pond. Within weeks, frogs, toads, and birds made themselves at home. A year later, the pond teems with tadpoles, mosquito fish, dragonflies, water beetles, and countless other tiny creatures.
The pond has become a source of daily joy and fascination for family and visitors alike—a reminder of how deeply nature nurtures our spirits. It has also been a powerful tool for stress relief and mental well-being.
For those managing diabetes, chronic conditions, or everyday stress, spending time in nature and caring for living things can be deeply therapeutic. And it doesn’t have to be complicated.
Start small:
For the more adventurous, creating a native plant garden is a wonderful excuse to get outdoors, move your body, and take pride in a growing, living space. There’s something special about tasting a sun-warmed tomato that’s been nurtured from seed to fruit.
A great place to start is the article Audubon – 20 Common Types of Native Plants, which outlines beneficial plants found across the U.S. To make it local, cross-reference with your zip code using tools like the Native Plant Finder – NWF by the National Wildlife Federation.
For example, in Chico, California, the California Christmas-Berry is drought-tolerant and a favorite food source for local birds.
🌳 Here are a few native plant ideas to consider:
Need help sourcing plants? The Plant Native website offers a helpful directory of native nurseries throughout the U.S.
Many people feel overwhelmed or discouraged by the state of the planet. But there is also a growing awareness of our power to make change—and hope rooted in action.
Whether it’s planting a single native shrub, providing a bowl of water, or simply observing and appreciating the life around us, every effort makes a difference.
Visit www.earthday.org and Project Regeneration for more ideas and inspiration on how to help the Earth thrive.
Each person has the ability to nurture the planet and themselves, starting right at home. Native plants are a simple, beautiful way to support both biodiversity and human well-being.
So this Earth Day, consider taking that first step. Plant something. Provide water. Let nature in. And know that even the smallest actions ripple outward in meaningful ways.
🌎 Happy Earth Day from Coach Beverly and the Diabetes Education Services team.

Q: What do you see as the most common misconceptions healthcare professionals have about people who don’t engage effectively with diabetes self-management behaviors?
A: The most common misconceptions are that people who don’t engage with diabetes management are unmotivated, not scared enough, and don’t care about their health.
We asked our favorite diabetes psychologist, Susan Guzman, PhD, to share her insights on how to engage most effectively when providing care to people with diabetes. Keep reading for more expert insights.
Q: How do these misconceptions lead to further problems for people with diabetes and further frustrations for the HCPs?
A: Not understanding the actual barriers to effective engagement leads to responses that don’t help. If you think someone is unmotivated, you might encourage someone to try harder or offer advice that doesn’t meet the person’s needs. If you think someone isn’t taking action because they must not be scared enough, you might try to warn them of all the terrible complications that could happen if they don’t make changes. If you believe someone doesn’t engage with diabetes self-management because they don’t care about their health, you may stop suggesting changes thinking they won’t do it anyway.
Because these are misconceptions, these corresponding tactics are ineffective, often leading people to feel more disengaged and misunderstood, immobilized with fear and hopelessness. In turn, HCPs too can end up feeling more frustrated and hopeless about helping patients reach treatment targets.
Q: What are some of the actual reasons people may not engage with diabetes self-management?
A: There are many common barriers that can result in someone seeing that needed changes as not worth the effort required or seem unachievable. When you begin to see the “good reasons” for people feeling disengaged from diabetes care, you can start to spot solutions that better fit the problem. For example, someone might actually feel doomed (scary complications and early death are unavoidable) and are hopeless that their efforts will have a positive impact. Instead of a scary lecture, this person could really benefit from some “evidence-based hope”, learning that there is good evidence that with targeted effort as a team to reach target, it is possible to have a long and healthy life with diabetes.
Q: Are there quick ways to identify these common barriers to effective diabetes management and brief interventions to help?
A: Yes! There are simple evidence-based ways to identify common behavioral obstacles and address them in routine clinical care. In our one-day workshop, “Engaging the Disengaged: Innovative Strategies for Behavior Change in Diabetes” we will help participants gain confidence in using these tools, having more productive conversations and collaborating with patients in generating more engaging and effective treatment plans.
Q: Are there any upcoming trainings available to explore these techniques and strategies?
A: Yes! Dr. William Polonsky and myself are facilitating a 6-hour conference in San Diego designed to bring these concepts life. This course isn’t a lecture — it’s an immersive, skills-building experience. Using a collaborative, person-centered approach, participants will practice real communication strategies that enhance motivation, build patient confidence, and make self-management feel doable. From diabetes distress to action planning to long-term adherence, every skill you gain is immediately applicable in your practice.
Sign-up today, since we are limiting enrollment to 50 people!

Dr. Susan Guzman is a clinical psychologist specializing in diabetes. In 2003, Dr. Guzman co-founded the Behavioral Diabetes Institute (BDI), the first non-profit organization devoted to the emotional and behavioral aspects of living with diabetes.
At BDI, she serves as the Director of Clinical Education, developing and leading programs for people with diabetes and healthcare professionals. She has helped develop and facilitate diabetes distress group interventions for two NIH-funded research studies for adults with type 1 diabetes.
Dr. Guzman is passionate about helping to change the conversations in diabetes away from shame, blame, and judgment to those based on facts, empathy, and engagement. She has been part of a joint ADA/ADCES effort to address problematic language and messages in diabetes.

Dr. William H. Polonsky, PhD, CDCES
In addition to being the Co-Founder of the Behavioral Diabetes Institute, Dr. Polonsky is Associate Clinical Professor in Medicine at the University of California San Diego.
A licensed clinical psychologist, certified diabetes care and educational specialist (CDCES), and highly-cited research scientist with more than 150 peer-reviewed publications in the field of behavioral diabetes.
His most recent research projects have focused on quality of life in diabetes, diabetes-related distress, hypoglycemic fear, glucose monitoring behavior and attitudes in people living with diabetes, group-based behavior change programs, the influence of continuous glucose monitoring on quality of life, and the development of new methods for enhancing diabetes education. In addition, he continues to maintain a small clinical practice where he works with his patients to help alleviate the stresses, strains and aggravations of living with diabetes.
Of note, he has authored several books for the lay audience (e.g., Diabetes Burnout: What to Do When You Can’t Take it Anymore) and co-edited several others for health care professionals (e.g., A CORE Curriculum for Diabetes Education).
Have you ever left a medical appointment thinking, “I wish I had asked that question,” or “I wish someone really understood what this feels like”?
Managing type 2 diabetes is not just about numbers. It is about decisions. Emotions. Responsibilities. Fatigue. Food. Family. And sometimes feeling like you are carrying all of it alone.
That is why Coach Beverly and DiabetesSisters are proud to launch a new chapter in diabetes support on the West Coast!
Coach Beverly has been a nurse for 40 years and a diabetes specialist for 30. For two decades, she led a hospital-based diabetes support group that became a trusted space for women to gather, learn, and feel understood.
Now, she is bringing that experience to a new West Coast Type 2 Diabetes Support Group with DiabetesSisters.
What drew her to diabetes care was not only the science but the opportunity to make a difference in how women experience living with this condition.
She noticed that many conversations focused on what was not working. Very few recognized the daily effort required to manage a condition no one asked for.
She believes women deserve more than instruction. They deserve encouragement.
As she often reminds participants:
You are already doing more than you think.

This new diabetes support program on the West Coast is built around something simple and powerful: connection.
When women gather in Coach Beverly’s group, they talk about the realities of living with type 2 diabetes, including:
One woman shares something she has never said out loud. Another nods in recognition. And just like that, isolation begins to soften.
Peer support has been shown to strengthen confidence and encourage meaningful behavior change. Our 2024 survey data show that 90 percent of participants felt confident making behavioral changes, and 88 percent felt confident taking steps to support their diabetes management.
But beyond the numbers, there is something deeply human about being seen.
As one participant shared: “I feel so much more connected and less alone in my diabetes journey through the monthly meetings. DiabetesSisters is an amazing resource and community.”
That is the experience this new West Coast program is creating.
Because this is a new program on the West Coast, you have the opportunity to join from the very beginning.
At your first session, you can expect:
At the end of each meeting, you may choose one small, realistic commitment to focus on before the next session. Not a complete life overhaul. Just one doable step.
This is not about perfection. It is about progress. It is about living well while managing diabetes.
If you are a healthcare professional, this new diabetes support program on the West Coast offers an additional layer of care for women living with diabetes.
Diabetes management does not end in the exam room. Women benefit from structured peer support that addresses emotional health, daily decision-making, and lived experience.
Coach Beverly’s group complements clinical care and reinforces self-management behaviors. We welcome referrals for women living with type 2 diabetes who may benefit from additional support.

If you are living with type 2 diabetes and wondering whether this new group is for you, Coach Beverly has a simple invitation:
Come once.
And there is a seat waiting for you.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory & practice.

Featured Articles & Announcements ___________________________ |
Webinars & Programs
___________________________
March is National Nutrition Month, and I love the core of this year’s theme, “Discover the Power of Nutrition.” Nutrition does have the power to help individuals and communities thrive, especially our cherished community of people with prediabetes and diabetes.
This month, we recognize the impact that nutrition and Registered Dietitian Nutritionists (RDNs) make on people’s lives. All of us have been asked, “Just tell me what I can eat.” We share the basics with our clients and then refer them to our trusted and knowledgeable RDN colleagues, who expertly guide them through medical nutrition therapy and create customized meal plans that encourage folks to “maintain the pleasure of eating”.
In our first article, Christine Craig, MS, RDN, CDCES, explores the role and real impact of RDNs in a variety of settings. Ms. Craig also recognizes that we need to keep inviting people with diabetes to meet with dietitians, as MNT can lower A1C levels by 0.3 – 2%.
Explore our Carb Counting Made Easy Resource Page, featuring handouts, links, and our most frequently requested resources.
Coach Bev provides straightforward strategies (and a New Worksheet) that outline the steps to provide judgment-free coaching to the people in your care. Please, share this worksheet with your colleagues and let us know what you think!
Have you had people with diabetes ask you if those glucose watches really work? Me too! Dr. Beattie discusses which devices are approved for glucose sensing and which are not.
Diabetes Sisters and Coach Bev have teamed up to offer a virtual support group on the West Coast. Thank you in advance for sharing this resource with your clients.
Test your knowledge with a quiz that boldly broaches the topic of Pancreatic Parasites.
Lastly, we heard you! We moved up the dates of our CDCES and BC-ADM Bundles, so you have more time to prepare for exam success.
Celebrating the power of nutrition and RDNs!
Coach Beverly, Bryanna, Astraea & Katarina
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Enjoy this poem by Coach Bev that summarizes steps to achieve diabetes certification success in 53 seconds!
Get Ready for Diabetes Certification Success
___________________
We know you’re excited to take your certification exam — and we want you to walk in feeling confident, calm, and completely prepared. 🖥️ To make sure you have the content you need, we have moved up the dates for our Level 3 and Level 4 live courses by a few months. We will complete Level 3 live course updates by April 30th and Level 4 updates will wrap up by June 20th. 📆Download Boot Camp flyers for complete date listings. |
We are always keeping you in mind! All of our accredited content is person-focused and evidence-based. Plus, we make sure you have fun and feel engaged during our programs. |
To prepare for your CDCES, we recommend enrolling in our CDCES Boot Camp, which includes:
✔ Level 1 – Fundamentals (2026) Recorded and ready for immediate viewing. Build your foundation and master the core concepts.
✔ Level 2 – ADA Standards Intensive 2026. Live throughout February and March. We break down the Standards of Care so they actually make sense — and stick.
✔ Level 3 – Final Exam Prep Mastery. Originally scheduled for June… but you told us that was too late. We heard you.
Level 3 now begins in March and runs through April 30th — giving you earlier access to focused exam mastery and test-taking strategy.
⬇️Download CDCES Boot Camp Flyer with New 2026 Dates!
This is your CDCES step-by-step path: Level 1 → Level 2 → Level 3. From fundamentals to final confidence 🏆.
To prepare for your BC-ADM, we recommend enrolling in our BC-ADM Boot Camp, which includes:
✔ Level 2 – ADA Standards Intensive 2026.
✔ Level 3 – Final Exam Prep Mastery. Begins in March and runs through April 30th.
✔ Level 4 – Final Exam Prep Mastery. Begins in April and runs through June 20th.
⬇️ Download BC-ADM Boot Camp Flyer with New 2026 Dates
This is your BC-ADM step-by-step path: Level 2 → Level 3 → Level 4. From Standards to advanced to final confidence 🏆.
You are the reason that diabetes care gets better.
We appreciate your hard work, advocacy, and the care you give every day!
💜Coach Beverly, Bryanna, Astraea, and Katarina
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.

Announcements
___________________
Healing through Connection for Healthcare Professionals is available in:
Like me, I am sure you have experienced moments of intense frustration when you wanted to scream or give up!
Maybe you had to show up when you were emotionally spent and felt like you had nothing else to give.
I see you and I celebrate you—the hardworking healthcare professional who shows up day after day with heart and courage. In my book, Healing through Connection, I honor your journey and share strategies to help you care for your own well-being as you care for others.
Join a Virtual Conversation and Interview with Coach Bev on Feb 20th at 11:30am PST to delve into the healing power of creative endeavors.
If you can’t make the interview, enjoy this excerpt from Chapter 6, that dives into the Healing Power of Self-Expression and encourages you to dive into your creativity for healing, rejuvenation, and pure JOY.
Even if you can only commit to engaging creativity for a few minutes or half an hour a week, it makes a difference. Stop thinking about all the reasons you can’t do it, and instead, listen to that internal hum, get in the metaphorical car, turn on the ignition, and drive.
Within you lives a quiet, creative spark waiting for attention and care. When you tend to it, you renew your capacity to show up with presence, compassion, and strength, for yourself and for those in your care.
Healing through Connection is both a reminder and a roadmap; an invitation to care for yourself with the same compassion you offer others. It provides a rare perspective on mutual healing.
As we heal ourselves, we expand our capacity to help others with healing. Within the pages of this book, you’ll find a toolbox for exploring your truth, tapping into your emotions, and cultivating creativity. Together, we’ll explore the often-overlooked connection between your own lived experiences and those of the individuals in your care.
Continue reading to discover how making time for creative expression might offer you some unexpected benefits and opportunities for joy!
Did you know that Nobel Prize recipients are nearly three times more likely to engage in creative hobbies than their scientific counterparts?
Theoretical physicist Albert Einstein often played the violin when he encountered challenges in his theoretical work. He believed that music helped him think creatively and tap into his subconscious, enabling breakthroughs such as the theory of relativity.
Marie Curie, a two-time Nobel laureate for physics in 1903 and chemistry in 1911, went for frequent walks in the countryside, which allowed her to reflect and rejuvenate. These moments of tranquility likely helped her maintain focus during the grueling work of isolating radioactive elements.
It’s because they’re simply more open to having hobbies. They are more open to novel experiences and often turn to their creative endeavors when working through challenges. These seemingly unrelated scientific pursuits and personal hobbies can open doors for scientists to crosspollinate ideas across different fields, enabling them to gain fresh perspectives and uncover new insights.
Now, you may not be working toward securing the title of a Nobel laureate. Still, you might be interested in learning the secrets of expanding your mind, creating new connections, and better integrating the two sides of your brain hemispheres to provide better care or nurture your inner life.
You may be wondering how having an artistic hobby or winning a Nobel Prize in science relates to excelling as a diabetes specialist or healthcare professional. As a healthcare professional, you have likely lived through difficult experiences or witnessed profound suffering firsthand.
Plenty of science supports the idea that engaging in creative pursuits offers an outlet to express complex emotions that are not accessible through words alone.
The act of playing an instrument, taking an art class, exploring nature, or playing the bongo drums may provide a gateway to address unrequited trauma or pain, helping you to become more fully aware and present with your feelings. Did you have a childhood or adult hobby you loved doing? One that made you lose track of time as you entered the zone referred to as “flow”? Have you given yourself permission to make time for that hobby and lose yourself in that creative process?
You may want to take a ceramics or writing class, join the local choir, or start a band. Perhaps you found an old camera and want to learn more about photography or realized you’re good at painting. It can be hard to start as a beginner and potentially look silly or unskilled.
Here’s my advice: Let go of those sky-high expectations. No one expects you to paint like Monet in your first art class.
My motto is, if something makes me uncomfortable, I know I’m in the right place—because that’s where growth happens.
I encourage you to take that leap of faith and tolerate the momentary discomfort for long-term gain. It gets better, and before you know it, you will blossom in ways you never expected.
Download this worksheet to explore 20 creative endeavors that may spark inspiration within you. You may already be practicing some of these—or perhaps you have new ideas to add. Wonderful—keep going!
As a dance teacher for the past twenty years who can still balance a sword on her head, I am reminded every day that it is never too late to rediscover your joy.
Coach Beverly is honored to invite you to this special gathering and intimate conversation. During this virtual book launch, a special guest interviewer will join Coach Bev for a heartfelt conversation about why this book matters now and the real stories from clinical practice that inspired it.
Coach Bev will also share the personal journey of writing Healing through Connection and how she discovered her voice along the way. We will conclude with an interactive question-and-answer session and allow time for connection.
Come celebrate connection, healing, and the power of story as we honor the shared human experience at the heart of healthcare.
Thank you for YOUR support and commitment to promoting healing and connection every day!