Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Our September 8, 2020, Question of the week quizzed test takers on a complicated case study that asked what was the most important information to share with a person starting on a GLP-1 Receptor Agonist. Although 55% of respondents chose the correct answer, 45% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: AJ takes 85 units of basaglar at bedtime and 10 -12 units of glulisine (Apridra) at meals, plus metformin and empagliflozin at maximum dose. Fasting blood sugars are 130 or greater and the rest of the day, AJs blood sugars are in the 200s. AJ has a BMI of 32 and an A1c of 9.3%. The diabetes specialist recommends adding semaglutide (Ozempic) 0.5 mg to the regimen. What teaching information is most important given the addition of this new medication?
Answer Choices:
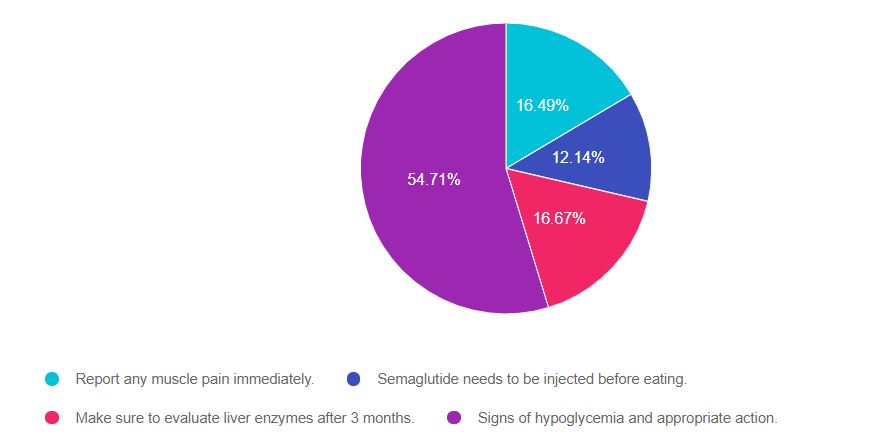
As shown above, the most common choice was option 4, the second most common answer was option 2, then option 3, and finally option 1.
If you are thinking about taking the certification exam, this vignette practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question and common knowledge. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, eliminate false answers and choose the BEST answer.
And you may want to Download our Medication PocketCards for detailed info on the available diabetes meds.
Answer 1 is incorrect. 17% chose this answer, “Report any muscle pain immediately”. This is a juicy answer. It is true that statins, the medication class used to manage lipids in diabetes, can cause muscle pain. But, the medication being added, semaglutide (Ozempic), is a GLP-1 Receptor Agonist, not a statin. Its main side effects includes nausea and loss of appetite, but muscle pain is not a common side effect of GLP-1 Inhibitors. This answer is false.
Answer 2 is incorrect. 12% of you chose this answer, “Semaglutide needs to be injected before eating”. This is another juicy answer. There are 2 forms of semaglutide. One is Ozempic, it is a once a week injection. People taking this injectable version, do not need to inject on an empty stomach. However, the oral form of semaglutide (Rybelsus), does need to be taken on an empty stomach with only a sip of water (See our Medication PocketCard for more details).
Answer 3 is incorrect. About 17% of respondents chose this, “Make sure to evaluate liver enzymes after 3 months”. It is true that we monitor liver enzymes for people with diabetes if they are on statins or to help screen for fatty liver disease. However, this GLP-1 Receptor Agonist has no indication to monitor liver enzymes after starting treatment.
Finally, Answer 4 is correct. 55% chose this answer, “Signs of hypoglycemia and appropriate action”. Yes, this is the BEST answer and it was a little tricky. Semaglutide (Ozempic), is a GLP-1 Inhibitor and does not cause hypoglycemia. However, this person is on a 85 units of basal insulin daily, plus 10 -12 units of bolus insulin at meals. With the additional glucose lowering impact of the GLP-1 Receptor Agonist, they are at risk of hypoglycemia from the insulin. Many people actually require a decrease in their insulin dose when adding on or increasing the dose of a GLP-1 RA.
Download our Medication PocketCards for detailed info on the available diabetes meds.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

In each webinar, either Coach Beverly, Dr. Isaacs, or Ms. Armstrong, highlight the critical content of each topic area, so you can focus your study time most efficiently. They also launch multiple poll questions to help participants focus on key concepts and assess their knowledge while learning the best test-taking strategies.
2020 Boot Camp Live Stream Webinar Schedule with Coach Beverly
All courses air at 11:30 a.m. (PST)
Can’t make it live?
No worries! All video presentations and podcasts will be available now on-demand.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
[yikes-mailchimp form=”1″]Our August 18th Question of the week quizzed test takers on the difference between a CDCES and BC-ADM. Although 54% of respondents chose the correct answer, 46% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Answer Choices:
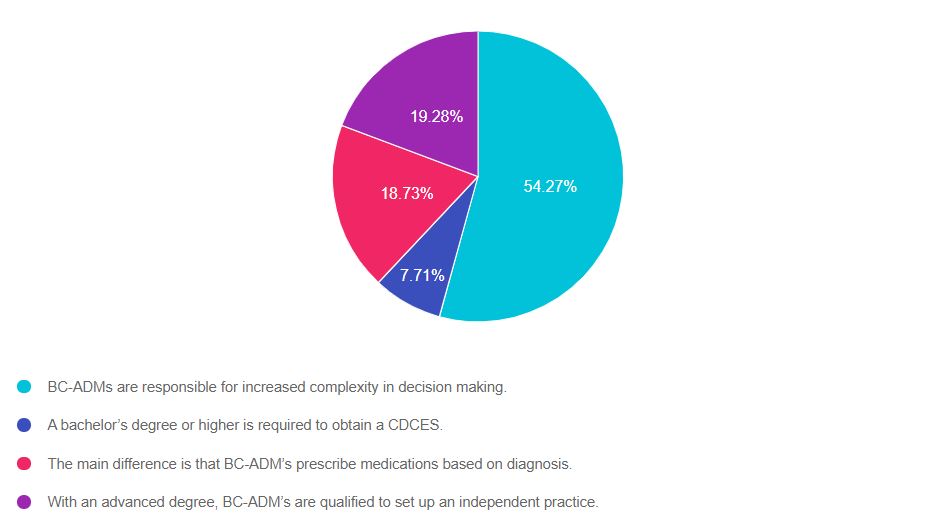
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 3, and finally option 2.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer. And remember, sometimes the simplest answer is the best answer.
Answer 1 is correct. 54% chose this answer. “BC-ADMs are responsible for increased complexity in decision making.”
According to the ADCES website:
“The BC-ADM skillfully manages complex patient needs and assists patients with therapeutic problem-solving. Within their discipline’s scope of -practice, healthcare professionals who hold the BC-ADM certification adjust medications, treat and monitor acute and chronic complications and other comorbidities, counsel patients on lifestyle modifications, address psychosocial issues, and participate in research and mentoring.”
Answer 2 is incorrect. 8% of you chose this answer. “A bachelor’s degree or higher is required to obtain a CDCES.”
Eligibility to take the exam is based on licensure, registration, or certification. According to the CDCES website, the following health care professionals meet the discipline requirement.
Answer 3 is incorrect. About 19% of respondents chose this. “The main difference is that BC-ADM’s prescribe medications based on the diagnosis”.
The BC-ADM is a certification exam and it does not confer prescriptive authority. Only those with certain licenses can prescribe medications, and the regulations can vary from state to state. For example, I am a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. As a licensed RN, I do not have prescriptive authority. Certification does not change your scope of practice and can come from different organizations. Licensure comes from governmental authority.
Finally, Answer 4 is incorrect. 19% chose this answer. “With an advanced degree, BC-ADM’s are qualified to set up an independent practice.”
This is a juicy answer but is not correct. Let’s say I want to set up shop as a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. Even with my BC-ADM, I couldn’t bill for services, and under whose oversight would I see people with diabetes and make treatment recommendations?
Again, it’s not the BC-ADM that creates the opportunity to set up an independent practice. As a licensed RN, I can’t set up an independent practice and bill for my services in my state. Certification does not change your scope of practice and can come from different organizations. Each state’s licensure and scope of practice regulations come from a governmental authority. We must practice within the legal parameters of our scope of practice based on licensure.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
In each webinar, either Coach Beverly, Dr. Isaacs, or Ms. Armstrong, highlight the critical content of each topic area, so you can focus your study time most efficiently. They also launch multiple poll questions to help participants focus on key concepts and assess their knowledge while learning the best test-taking strategies.
2020 Boot Camp Live Stream Webinar Schedule with Coach Beverly
All courses air at 11:30 a.m. (PST)
Can’t make it live?
No worries! All video presentations and podcasts will be available now on-demand.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
[yikes-mailchimp form=”1″]Our August 4th Question quizzed test takers on CV Disease risk management and diabetes. Although 49% of respondents chose the correct answer, 51% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: RJ is 67 years old with a 40+ year history of type 1 diabetes. GFR is 62, UACR is < 30, A1c is 6.7%, B/P is 132/72, LDL cholesterol is 98, RJs BMI is 28.6. RJ uses multiple daily injections and CGM to manage RJs diabetes.
RJ’s other medications include: Levothyroxine 100mcg daily, atorvastatin 40mg daily, Aspirin 81 mg daily and a multivitamin.
Based on your assessment, which of the following interventions would improve RJs outcome?
Answer Choices:
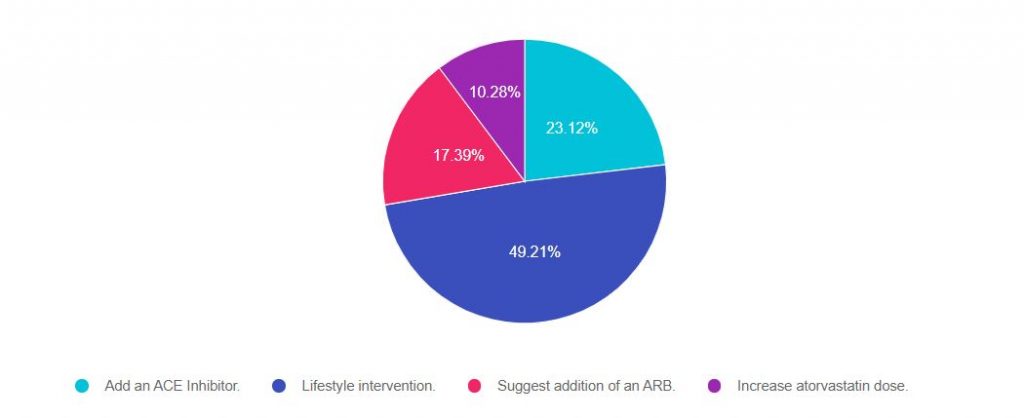
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers will ask about the guidelines for specific ADA Standards of Care. This question is pulled from section 10 of the Standards on CV Disease and Risk Management. To purchase your own ADA Standards, visit our store.
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
Answer 1 is incorrect. 23% chose this answer. “Add an ACE Inhibitor.”
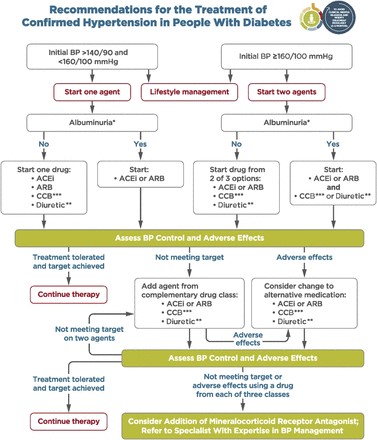
Many people chose this juicy answer. It is true that in the past, people with type 1 would be automatically started on an ACE Inhibitor because it was thought starting an ACE would offer renal protection. However, based on extensive research, the American Diabetes Association stopped recommending adding an ACE for people with type 1 without the diagnosis of hypertension a few years back.
The current blood pressure goal for people with diabetes is 140/90.
If a person with type 1 diabetes has hypertension, defined as either systolic greater than 140 or diastolic more than 80, repeated on 2 different occasions, initiate blood pressure therapy.
Lower blood pressure goal of 130/80? It is recommended to do a cardiovascular risk assessment using the CV Risk Calculator on all people with diabetes. If the 10 year risk of having a CV event is greater than 15%, the blood pressure goal is 130/80 may be appropriate, if it can be safely attained. The choice of blood pressure therapy is further refined by presence or absence of microalbuminuria.
We don’t have enough information to calculate his CV Risk, so based on the information we have, adding an ACE Inhibitor is not indicated at this time. And of course, since we only have one blood pressure, we need to collect more data before taking action.
Answer 2 is correct. 49% of you chose this answer. “Lifestyle intervention.”
This is the best answer. Looking at this profile, we can see that RJ’s BMI is above 25 and LDL is slightly elevated. Let’s refer RJ to a Registered Dietitian. By coaching RJ on healthy food choices, increased whole foods and fiber, and taking a look at animal protein consumption, there is an opportunity to improve not only RJs blood pressure but also RJs LDL cholesterol. In addition, we can evaluate RJs activity level and encourage 150 mins a week of activity plus strengthening that would contribute to his overall health.
Answer 3 is incorrect. About 17% of you chose this answer. “Suggest addition of an ARB.” See rationale under answer 1.
Finally, Answer 4 is incorrect. 10% of you chose this answer. “Increase atorvastatin dose.” Currently, RJ is on high intensity statin therapy with RJs atorvastatin dose of 40mg. He does not present with any concerning CV risk factors or events that would kick RJ into high risk category. We could calculate RJs 10 year risk of CV disease and if it is more than 20% or if RJ doesn’t response to lifestyle changes, we could consider a further increase in the statin dosing. Based on the info we have at this moment, this is not the BEST answer (but it is a consideration : -).
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
This question addressed the use of SGLT-2 Inhibitors in addition to insulin for MS, who is living with Type 1 Diabetes. MS is worried about weight gain and is on a low keto diet. It is safe for here to add an off-label medication?
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: MS has type 1 diabetes and is on a low carb diet to help her keep her weight on target. She has a BMI of 24.3. MS has a friend with type 1 who is taking an SGLT-2 in addition to insulin to help with weight management. MS wants to know if she could add on an SGLT-2 to her insulin treatment plan.
What is the Diabetes Specialist’s best response?
Answer Choices:
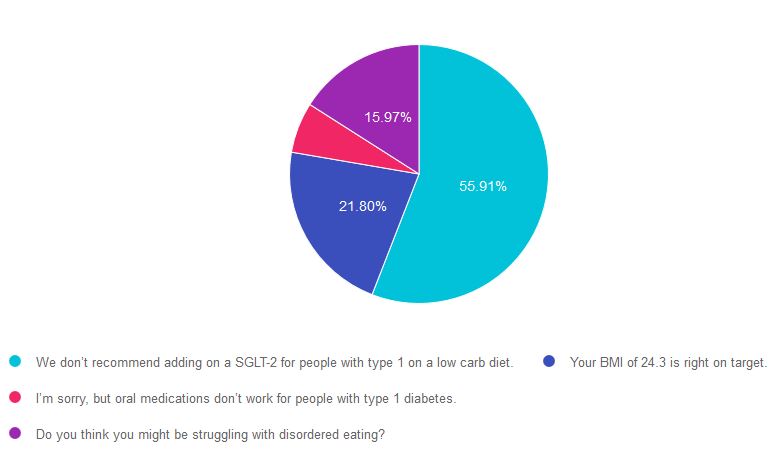
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 4, and finally option 3.
If you are thinking about taking a certification exam, this practice test question will set you up for success. The test writers will include warnings about medications and ask you to choose the best response. Your job is to weed through the particulars, pluck out the most important elements, eliminate at least two false answers to improve your odds of success to 50/50.
Answer 1 is correct! “We don’t recommend adding on an SGLT-2 for people with type 1 on a low carb diet.” Even though SGLT-2’s are sometimes prescribed to people with type 1 diabetes (in addition to insulin), they are not FDA approved in type 1 and are considered “off-label.” SGLT-2 also contains a warning of an increased risk of ketoacidosis. This risk is especially important to consider in type 1 diabetes, since people with type 1 using an SGLT-2 Inhibitor may decrease their daily insulin dose and increase the risk of ketoacidosis.
This risk might be exacerbated by a low carbohydrate diet. As outlined in the ADA Standard 5, “This [low carbohydrate] eating pattern is not recommended at this time for women who are pregnant or lactating, people with or at risk for disordered eating, or people who have renal disease, and it should be used with caution in patients taking sodium-glucose cotransporter 2 inhibitors due to the potential risk of ketoacidosis.”
Answer 2 is incorrect! “Your BMI of 24.3 is right on target.” This is a juicy answer because it is true. The BMI is below 25, but it does not address the key intent of the question.
Answer 3 is incorrect. “I’m sorry, but oral medications don’t work for people with type 1 diabetes.” This is tricky. No oral medications are FDA approved for type 1 diabetes, but some are prescribed (metformin, SGLT-2s) by diabetes providers in addition to insulin. Still not the best answer.
Finally, Answer 4 is incorrect. “Do you think you might be struggling with disordered eating?” Another tempting answer, but MS isn’t exhibiting any signs of under-eating or under-dosing insulin or disordered eating.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want more practice questions?
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions, and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Our May 26th Question of the week was a question about carb counting. Although 56% of respondents chose the correct answer, 44% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: AJ is motivated to decrease weight. AJ eats an egg sandwich and hash browns 5 times a week. You look up the calories on an app and find that the egg sandwich has 370 calories and the medium hash browns have 390 calories.
If AJ doesn’t eat the hash browns for one month, how much weight would AJ lose?
Answer Choices:
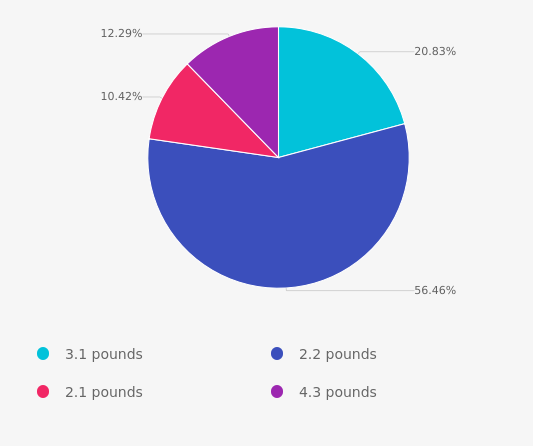
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.
If you are thinking about taking a certification exam, this practice test question will set you up for success. The test writers will anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and do the math with care.
Answer 1 is incorrect. 20% chose this answer. This question is all about paying attention to details. AJ eats the hash browns 5 times a week or 20 times a month. If you chose this answer, you had AJ eating hash browns every day.
Answer 2 is correct! 56% of you chose this correct answer. AJ eats hash browns 5 times a week or 20 times a month. Each hash brown has 390 calories. 20 x 390 = 7, 800 calories. There are 3,500 calories in a pound. So, 7,800 / 3,500 = 2.2 pounds loss in a month. Yay. Great job.
Answer 3 is incorrect. About 10% of respondents chose this. If you chose this answer, you might have been calculating the number of calories in the egg sandwich instead of the hash browns.
Finally, Answer 4 is incorrect. 12% chose this answer. You probably thought AJ was stopping eating both the egg sandwich and hash browns, which would lead to a 4.3-pound weight loss.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want more practice questions?
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions, and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
[yikes-mailchimp form=”1″]Our May 19th Question of the week was a question about carb counting. Although 58% of respondents chose the correct answer, 42% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LS uses an insulin pump and the 500 rule for carbohydrate coverage. For breakfast, LS plans to eat ½ cup of oatmeal, 3/4 cup of blueberries, a cup of skim milk, a tablespoon of peanut butter, and a cup of coffee with a packet of Splenda. Her insulin to carb ratio is 1 to 12 for breakfast and lunch. Her insulin to carb ratio is 1 to 15 for dinner.
How much insulin does LS need for breakfast?
Answer Choices:
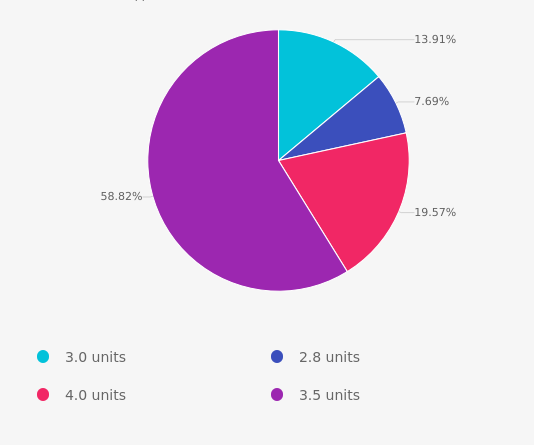
As shown above, the most common choice was option 4, the second most common answer was option 3 then option 1 and finally option 2.

Answer 1 is incorrect. 14% chose 3.0 units as the answer. This answer was juicy but wrong. Maybe this group thought the total carb count was 45 gms and then divided by insulin to carb ratio of 1:15? If yes, read the question again to see what insulin to carb ratio is a better choice. Also, rethink the total carb count.
Answer 2 is incorrect. Only 8% of respondents chose 2.8 units as an answer. This group got the carb count correct but may want to read the question again to see which insulin to carb ratio is a better choice.
Answer 3 is also incorrect. About 20% of respondents chose 4.0 units. This group might need to reassess the carb count, keeping in mind that milk is 12gms of carb. And, more importantly, keep in mind that LS uses an insulin pump that can deliver very precise insulin doses. No need to round up for this question.
Finally, Answer 4 is correct. 58% of test takers chose this correct answer.
First, lets count up the carbs for breakfast:
Now, let’s do the math:
LS’s insulin to carb ratio is 1 to 12 for breakfast. She is going to eat 42 gms of carb. 42/12 = 3.5 units of insulin to cover breakfast.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
This course is an essential review for anyone in the field of diabetes. This course summarizes the 2021 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for health care professionals involved in diabetes care and education.
Earn 2.0 CEs and get ready to lead the charge to implement best care practices for the New Year.
Topics Include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This question addressed rising blood glucose and best insulin adjustment strategy. Since this was our most popular question this month, we wanted to provide an explanation to pass on this valuable information to all of you and people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LS takes 20 units 70/30 insulin twice daily with an insulin pen. LS states that blood sugars are usually on target, but over the past week, blood sugars have suddenly increased. LS confirms that they are taking insulin on a regular basis.
Which factor could be contributing to this sudden blood glucose rise?
Answer Choices:
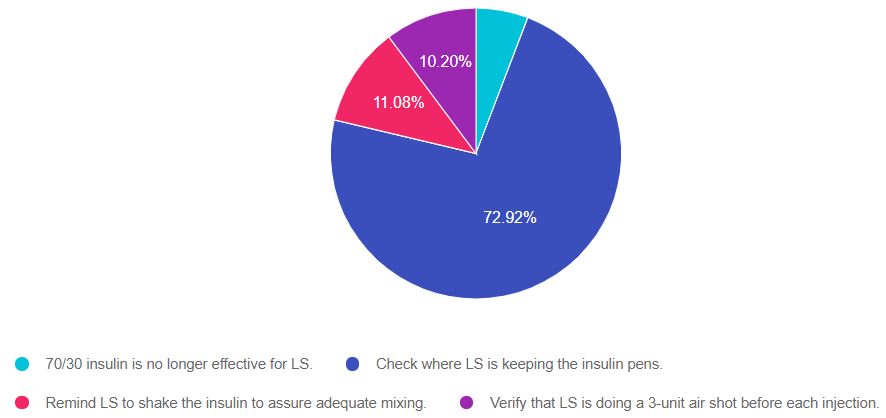
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally option 1.
If you are thinking about taking a certification exam, this practice test question will set you up for success. The test writers will anticipate possible wrong answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, eliminate at least two false answers to improve your odds of success to 50/50.
Answer 1 is incorrect “70/30 insulin is no longer effective for LS”. About 5% chose this answer. Based on the vignette, LS has been using 70/30 insulin and keeping blood glucose in target. It is only in the last week that blood glucose levels are rising. This points to another undiscovered recent issue that is causing blood sugars to elevate.
Answer 2 is correct! “Check where LS is keeping the insulin pens”. A whopping 73% of you chose this correct answer Great job. Insulin is a very sensitive protein and can lose effectiveness when stored in places where there are extreme temperatures.
Read package insert for detailed information:
Answer 3 is incorrect. “Remind LS to shake the insulin to assure adequate mixing.” About 11% of respondents chose this. Insulin manufacturers recommend NOT shaking 70/30 insulin since it can make the insulin less effective.
70/30 insulin mixing instructions
Invert the vial or pen at least 10 times to mix the two insulin until is appears white and cloudy. Do not shake. Do not use it if insulin looks clear or contains any lumps or particles.
Finally, Answer 4 is incorrect. “Verify that LS is doing a 3-unit air shot before each injection.” 10% chose this answer. The correct answer is to prime the insulin pen with 2 units of insulin before each injection to make sure that the pen and needle are working. When priming the pen, at least one drop of insulin should appear at the tip of the needle. Also, it’s a good idea to remind people to change the needle before each injection.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want more practice questions?
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Our April 31st Question of the week was a question about aerobics, hypothyroidism, cholesterol, and type 2 diabetes. Although 58% of respondents chose the correct answer, 42% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
You are working with KS, a 57-year-old with type 2 diabetes, who wants to join the water aerobics program at their local YMCA. KS has a history of hypothyroidism and has an LDL cholesterol of 98 mg/dl. KS’s medications include levothyroxine and metformin XR 1000 mg BID.
According to the ADA and the American College of Sports Medicine, what would be the best recommendation?
Answer Choices:
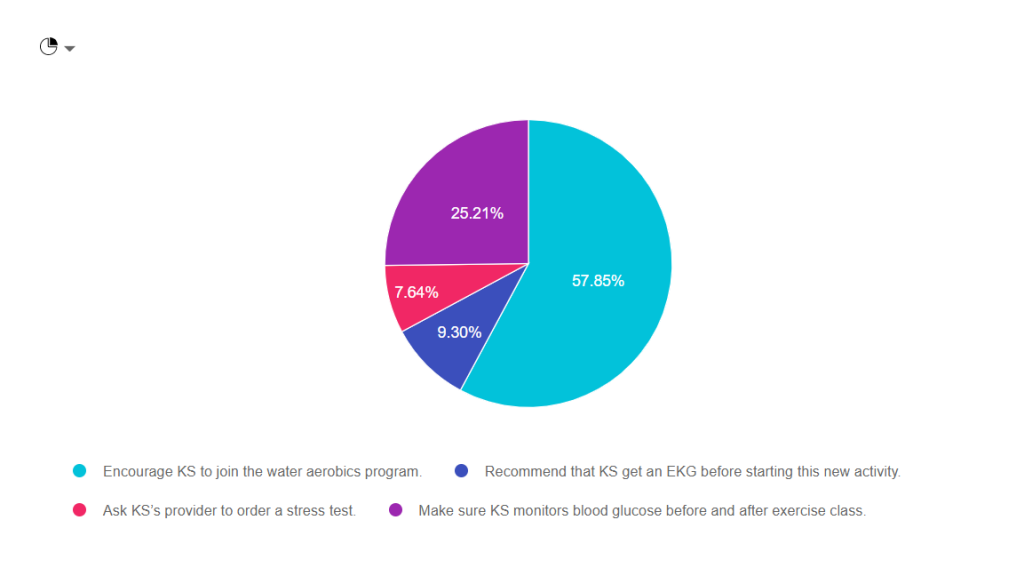
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.

Answer 1 is Correct! Encourage KS to join the water aerobics program. Based on the information provided, she would benefit from adding activity to her routine. Exercise decreases visceral adiposity, improves mood, lower glucose by enhancing insulin sensitivity. See our Exercise Resource Page for helpful info.
Answer 2 is incorrect. About 10% of respondents chose “Recommend that KS get an EKG before starting this new activity.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting an EKG for those with risk factors for cardiovascular events.
Answer 3 is also incorrect. About 10% of respondents chose “Ask KS’s provider to order a stress test.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting a stress test for those with risk factors or symptoms of cardiovascular events.
Finally, Answer 4 is incorrect. “Make sure KS monitors blood glucose before and after exercise class.” Having diabetes is a lot of work. As diabetes specialists, it is important that we don’t unnecessarily increase the burden of daily self-care. While KS may gain interesting information by checking BG levels before and after exercise, it is NOT necessary to monitor glucose before and after.
Why not? Since KS is not on any medication that causes hypoglycemia, her risk of low blood sugar is almost none. In addition, most people on oral medications are only allotted one strip a day to monitor blood sugars. Asking KS to check twice on water aerobics days may translate to extra out of pocket expenses that can also add to the financial burden of diabetes.
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
Pre-exercise Evaluation- 2020 Standards Of Care
The ADA consensus report “Screening for Coronary Artery Disease in Patients With Diabetes” (172) concluded that routine testing is not recommended. However, providers should perform a careful history, assess cardiovascular risk factors, and be aware of the atypical presentation of coronary artery disease in patients with diabetes. Certainly, high-risk patients should be encouraged to start with short periods of low-intensity exercise and slowly increase the intensity and duration as tolerated. Providers should assess patients for conditions that might contraindicate certain types of exercise or predispose to injury, such as uncontrolled hypertension, untreated proliferative retinopathy, autonomic neuropathy, peripheral neuropathy, and a history of foot ulcers or Charcot foot. The patient’s age and previous physical activity level should be considered. The provider should customize the exercise regimen to the individual’s needs. Those with complications may require a more thorough evaluation prior to beginning an exercise program (171).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]