
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
Join us on August 19th, 2026, at 11:30 am PST, for the 2026 NEW FREE BC-ADM® Exam Success Mini-Webinars

After carefully reviewing the Board Certification in Advanced Diabetes Management (BC-ADM®) Examination Content Outline, Coach Beverly identified several advanced topics that deserved additional attention to boost healthcare professionals’ readiness for the exam.
She created a series of FREE 20 to 30-minute mini-webinars that focus on these high-yield content areas, filling the gaps and completing your BC-ADM Boot Camp experience.
Join Coach Beverly live on August 19 as she walks through these focused review sessions designed to strengthen your advanced clinical knowledge and boost your confidence before the December BC-ADM exam. Can’t attend live? No problem! Each BC-ADM® Exam Success Mini-Webinars will be recorded and added to Level 4 of the BC-ADM Boot Camp Bundle for on-demand access.
While these complimentary webinars do not include continuing education (CE) credit, they are packed with practical insights, exam-focused content, and advanced clinical pearls that will help you master complex concepts and prepare for BC-ADM success.

Author, Nurse, Educator, Clinician, and Innovator, Beverly has specialized in advanced diabetes management for over twenty years and has successfully passed the CDCES exam six times. As president and founder of Diabetes Education Services, Beverly is dedicated to optimizing diabetes care and improving the lives of those with diabetes.
“As a diabetes nurse specialist for over 30 years, few things have been as rewarding as advocating for high-quality care on behalf of people living with diabetes. Earning my BC-ADM 25 years ago wasn’t easy—it pushed me into unfamiliar territory that felt overwhelming at the start. But with time, this new knowledge became part of my DNA. Whether I’m seeing individuals at our rural clinic or designing new teaching slides, my BC-ADM continues to make me a better clinician, educator and advocate.”
Exciting news: the New ADCES 7th Edition of the Review Guide and the Art and Science of Diabetes Care. If you are preparing to take your diabetes certification exams or need a comprehensive resource to refer to, these books are for you! Since we offer the e-version, you can order today and receive them in your inbox within 24 hours.
If you are considering taking the BC-ADM exam, 2026 may be your year. There are significant eligibility, renewal, and exam content changes coming in 2027 – so sign up to take your BC-ADM exam by November 1, 2026. Read more about the upcoming updates to the BC-ADM certification in Coach Bev’s article below. Or join her Free Prep for BC-ADM Webinar on July 29th.
Continued below…
Are you heading to the ADCES in Columbus, Ohio? If so, please stop by and say hi to Coach Beverly at either of her presentations.
On August 9th at 12:30, Coach Bev will be participating in a panel discussion on “Diabetes and Entrepreneurship”, led by the amazing Sarah Hormachea in the Exhibit Hall Learning Lab #3, Sunday, at 12:30pm. Grab your lunch and join us!
Also on Aug 9th at 2:30, Coach Bev will present “Healing through Connection,” a talk designed to allow diabetes health care professionals time to connect and share stories. There is so much to talk about. Hope to see you there!
Looking forward to connecting with all of you in person or virtually!
With hearts full of gratitude,
Coach Beverly, Bryanna, Ashlie, and Katarina

The Board Certification in Advanced Diabetes Management (BC-ADM) credential recognizes your clinical expertise and dedication to outstanding diabetes care.
Wondering What the Next Steps Are?
Join Coach Beverly for a FREE, information-packed webinar to map out your journey. Learn strategies to succeed at this mastery-level exam and map out your study journey. Plus, we will be adding in a special bonus section during the last 15 minutes.
Webinar airs July 29th at 11:30 am PST
This Review Guide is a must-have for anyone preparing for the CDCES and the BC-ADM Exam. With over 500 sample test questions with rationale, you can quickly assess your strengths and make a plan to fill in knowledge gaps.
Book details:
This updated edition delivers evidence‑based guidance you can use right away and is a powerful tool for strengthening your clinical expertise and filling in knowledge gaps in preperation for diabetes certification exams.
Book details:
Original Pricing: Starting at $449
New Pricing: Starting at $399
Original Pricing: Starting at $459
New Pricing: Starting at $399
Original Pricing: Starting at $519
New Pricing: Starting at $499

“I’ve managed my diabetes for years, but ever since starting cancer treatment, my blood glucose has been all over the place. I don’t know what I am doing wrong.”
As diabetes health professionals, our job is to support people through both complex clinical situations and the emotional challenges of living with cancer and diabetes. Having the knowledge to address both can improve engagement, lead to better outcomes, and strengthen relationships with the people we work with.
Diabetes and cancer are no longer just parallel health crises sharing a person’s chart; they are deeply entangled pathologies where hyperglycemia, inflammation and the risk of cancer development are interrelated. For diabetes healthcare professionals, mastering this bidirectional threat no longer falls under the rare case scenario.
As a diabetes professional, you have an important role in detecting sudden hyperglycemia as a result of chemotherapeutic agents, like checkpoint inhibitors and PI3k inhibitors. In addition, you can encourage people with diabetes to engage in regular cancer screenings and be aware of reportable symptoms. This is an immediate, high-stakes clinical mandate that can improve prompt treatment and detect cancer earlier.
The shared risk factors between type 2 diabetes and cancer (older age, elevated body weight, and lack of physical activity) increase this bidirectional association, but diabetes-related factors such as underlying disease physiology or diabetes treatments may also increase this cancer-diabetes connection.
One of the most clinically actionable areas of recent research highlights the relationship between a new diabetes diagnosis and pancreatic and other cancers.
People with type 2 diabetes face about twice the risk of developing pancreatic cancer compared to those without the condition, while an older adult (over 50) with new-onset diabetes experiences a sharper increase in risk within the first few years.
New onset of atypical diabetes (lean body habitus and negative family history) in a middle-aged or older person may precede the diagnosis of pancreatic adenocarcinoma. Additionally, in a nationwide cancer registry in New Zealand, post pancreatitis diabetes mellitus was associated with significantly higher risk (2.4-fold) of pancreatic cancer compared with pancreatitis after type 2 diabetes. (ADA).
Diabetes is associated with increased risk of cancers of the liver, pancreas, endometrium, colon and rectum, breast, and bladder.
Large-scale cohort analyses reveal that individuals with diabetes face a roughly doubled risk of developing
There are also notable 1.2- to 1.5-fold increases in:
People with diabetes are encouraged to schedule recommended age-and sex-appropriate cancer screenings, coordinated with their primary health care professional. As diabetes professionals, you can encourage individuals to take action and to reduce their modifiable cancer risk factors. Actions that help with diabetes management also reduce risk of cancer including:
The cancer frontier of oncology has been revolutionized by precision therapies, but these life-saving advancements can come with steep glucose elevations due to beta cell disruption.
Hyperglycemia due to chemotherapy may either be transient (improving upon treatment cessation) or represent permanent diabetes.
Immune checkpoint inhibitors are used to treat many types of cancer, such as melanoma, non-small cell lung cancer, bladder cancer, renal cell carcinoma, breast cancer, and Hodgkin lymphoma.
Common immune checkpoint inhibitors include: pembrolizumab (Keytruda), nivolumab (Opdivo), ipilimumab (Yervoy), durvalumab (Imfinzi), atezolizumab (Tecentriq).
The most likely Immune checkpoint inhibitors that rigger rapid, autoimmune-mediated destruction of beta cells include:
Insulin therapy is the cornerstone of management, as individuals typically present with rapid-onset, severe hyperglycemia or DKA. Many will initially need an insulin drip, followed by the implementation of basal bolus insulin therapy along with continuous glucose monitoring.
PI3K inhibitors are used primarily to treat advanced breast cancer (specifically HR+/HER2- tumors with PIK3CA mutations) and blood cancers (such as lymphomas, leukemias, and follicular lymphoma).
Phosphatidylinositol 3-kinase (PI3K) inhibitors are small molecules designed to disrupt intracellular signaling pathways, thereby inhibiting cancer cell growth and survival. Within this class, targeted inhibition of the alpha isoform (PI3Kα) disrupts downstream insulin receptor signaling, frequently resulting in profound, on-target hyperglycemia and acute insulin resistance.
Which PI3K medications are associated with glucose elevations?
These two types of PI3Kα inhibitors have a 60% incidence of causing hyperglycemia, typically appearing within the first 2 weeks of therapy.
People at increased risk of hyperglycemia from PI3K inhibitor therapy include those with:
Glucose management is crucial since significant hyperglycemia can lead to discontinuation and/or reduction in PI3K medication dose, which can decrease therapy efficacy.
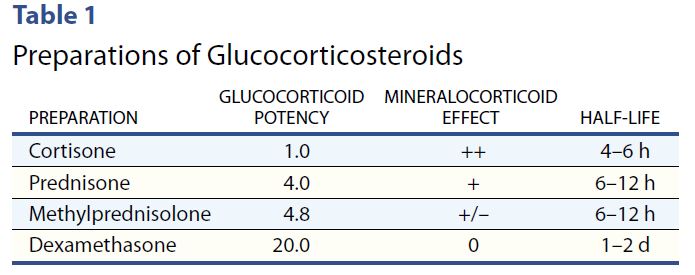
Cancer treatment often includes concurrent steroid therapy to enhance efficacy. However, steroid therapy can induce or worsen hyperglycemia.
Steroids have their highest potency at 4-12 hours, with the exception of the very potent dexamethasone, which has a half life of 1-2 days.
With morning steroids, including dexamethasone, people will experience elevated glucose values after breakfast, lunch, dinner, and at bedtime but will have a significant drop toward normal glucose overnight.
Therefore, hyperglycemia is greatest 1–2 hours after a meal, with persistent elevation until the following meal, followed by a return to normal overnight.
To treat steroid induced hyperglycemia, NPH. Neutral Protamine Hagedorn (NPH) insulin is an effective treatment choice since it is an intermediate acting basal insulin. NPH insulin is cloudy and has an onset of 1–4 hours. Its peak is 6–10 hours and its duration is about 10–16 hours. Download our Insulin PocketCards.
For individuals on once daily steroids, morning NPH with some bolus insulin can effectively target daytime hyperglycemia. For those taking steroids twice daily, an additional dose of NPH plus bolus as needed, is added at dinnertime.
Join Coach Beverly July 21 at 11:30am to learn more during our Cancer and Diabetes Webinar.
As diabetes professionals, we are stepping into a vital new role at the intersection of metabolic health and oncology. Modern cancer therapies like checkpoint inhibitors and PI3K inhibitors are absolute game-changers for oncology, but they often trigger sudden, severe hyperglycemia that catches patients and healthcare professionals off guard.
That is where our expertise becomes a literal lifesaver. By actively monitoring for sudden hyperglycemia and aggressively championing routine cancer screenings, we are doing so much more than just managing a chronic disease. We are taking on an urgent, high-stakes clinical mandate that ensures patients get immediate treatment when they need it most and catches cancer at its earliest, most treatable stages.
Ultimately, our vigilance bridges the gap between effective cancer therapy and safe metabolic health, directly shaping better, life-saving outcomes for the people in our care.
Explore the unexpected link between cancer and diabetes — and master glucose management strategies for people with diabetes undergoing treatment.
Individuals with cancer often experience hyperglycemia secondary to treatment, which can increase the risk of infection and other complications. Recent research has also identified a significant link between diabetes and cancer. This course uses a case study approach to explore this connection and provide practical strategies for managing steroid-induced hyperglycemia and improving quality of life for people navigating both conditions.
Course Topics:
Our July newsletter is packed with timely content you won’t want to miss. Plus, celebrate summer with our Sizzling Sale and get 20% off all Online Courses!
We sat down with ADA Outstanding Educator of the Year recipient Dr. Diana Isaacs and asked her a slew of interview questions. She generously shared her insights on the future of diabetes, the importance of connection, and doled out plenty of words of wisdom for us diabetes professionals. Congratulations, Diana, on a well-deserved award; we are so proud of you.
Coach Beverly discusses the intersection of diabetes and cancer. The article includes a summary of chemotherapy-induced hyperglycemia, along with treatment strategies. Join our upcoming webinar on July 21st, along with the article below for a comprehensive review.
Continued below…
The next article breaks down the newly announced Medicare Bridge Program for Weight Management. It includes prescribing information and eligibility requirements for Medicare Coverage.
Our guest contributor, Lilly Mees, LMSW, CDCES, explores how an individual’s self-efficacy affects their ability to manage diabetes. Read more and plan to join Lilly’s webinar on July 23rd.
Lastly, we consider equitable care for people with diabetes who live with hearing impairment or deafness. Learn more about a DSME program that incorporates American Sign Language.
Don’t forget our Question of the Week, the July 20th deadline for Scholar applications, and our Sizzling Summer Sale.
With hearts full of gratitude,
Coach Beverly, Bryanna, Ashlie, and Katarina
Did you know that YOU are practicing in a healthcare system where the traditional fee for service model is giving way to value-based diabetes care, and how essential YOU are in that shift?
As a diabetes professional, you will want to keep up to date on this upheaval of traditional models of care. You have the opportunity to take a leadership role and demonstrate your worth.
Healthcare is changing, and it is changing quickly. Terms like digital quality measures (dQMs), HEDIS®, STAR Ratings, interoperability, value-based contracting, artificial intelligence, and digital health technology are appearing more frequently in healthcare conversations.
While some of these concepts may seem far removed from day-to-day diabetes education, they are increasingly influencing how healthcare is delivered, measured, and reimbursed.
Today’s diabetes technologies such as continuous glucose monitors (CGMs), connected insulin delivery systems, and digital apps generate rich patient data that support chronic disease management and contribute to digital quality reporting. For diabetes care and education specialists (DCESs), understanding these trends is becoming more than simply staying current. It is about recognizing how our profession can continue to grow and demonstrate value within an evolving healthcare system.
 Healthcare is shifting because the current system is increasingly unsustainable. Costs continue to rise, outcomes remain uneven, and clinicians face growing administrative and reporting burdens that take time away from patient care. As a result, the United States healthcare system is moving from a fee for service model that rewards volume to one that emphasizes quality, outcomes, patient experience, and cost effectiveness. This shift is reflected in the Quintuple Aim, a framework that defines “what better care” means today.
Healthcare is shifting because the current system is increasingly unsustainable. Costs continue to rise, outcomes remain uneven, and clinicians face growing administrative and reporting burdens that take time away from patient care. As a result, the United States healthcare system is moving from a fee for service model that rewards volume to one that emphasizes quality, outcomes, patient experience, and cost effectiveness. This shift is reflected in the Quintuple Aim, a framework that defines “what better care” means today.
Originally introduced as the Triple Aim by the Institute for Healthcare Improvement, it has expanded to include clinician well-being and health equity. The Quintuple Aim focuses on:
Achieving these goals requires better data, stronger care coordination, and more meaningful ways to measure quality across the healthcare continuum.
Historically, quality measures relied on manual chart reviews or administrative claims data collected long after care was delivered. Today, healthcare is moving toward digital quality measures, which use electronic health records, patient generated health data, and interoperable systems to evaluate care more efficiently and more accurately. Programs such as HEDIS® and Medicare STAR Ratings continue to play an important role in measuring healthcare performance. As quality measurement becomes increasingly digital, organizations are looking for ways to improve outcomes while creating a better experience for both clinicians and the people they serve.
Clinicians today are overwhelmed by documentation requirements, reporting tasks, and manual data entry that often feel disconnected from actual patient care. Much of this work happens outside the visit, reviewing charts, pulling reports, reconciling data, and ensuring that quality metrics are accurately captured.
Manual chart reviews- time consuming and prone to error
Data reconciliation- pulling information from multiple systems
Tracking missed care gaps- directly affecting quality scores
Inconsistent documentation- variability across clinicians
Automated data capture- improves accuracy and reduces variability
Integration of CGM data- connecting patient generated health data directly to quality metric reporting
Real time gap identification-spots missing care gaps such as retinal eye exams or overdue kidney function testing
Reduced administrative burden- frees up clinician time and could lower cost of care
By shifting quality reporting from manual processes to automated digital workflows, healthcare organizations can create a more streamlined experience for both care teams and patients. More accurate and timely data supports better decision making, improved outcomes, and stronger performance in value based care programs.
Recent updates to HEDIS® reflect the growing role of diabetes technology in routine care, particularly CGM’s. For the 2024 measurement year, NCQA updated the Hemoglobin A1c Control for Patients With Diabetes measure and renamed it Glycemic Status Assessment for Patients With Diabetes, allowing either hemoglobin A1c or glucose management indicator (GMI) derived from CGM data to be used when assessing glycemic status.
Looking ahead, NCQA has proposed a new HEDIS measure, Continuous Glucose Monitoring Utilization for Patients With Diabetes, for the 2027 measurement year, which would track CGM use among adults with diabetes. While there is interest in expanding CGM based reporting beyond glucose management indicator to include metrics such as time in range, those elements have not yet been formally incorporated into HEDIS.
Together, these changes reflect a growing alignment between diabetes technology and value-based care, reinforcing CGM as a meaningful tool for improving outcomes and meeting evolving quality expectations.
As healthcare continues to evolve, you are uniquely positioned to help organizations navigate this transformation. The shift toward digital quality measures, expanded use of CGM data, and growing emphasis on value-based care highlight the need for clinicians who understand both the human side of diabetes and the technology that increasingly supports it. You already excel at patient engagement, technology adoption, behavior change, and chronic disease management, all core drivers of quality performance.
By deepening familiarity with digital reporting, leveraging diabetes technology, and helping with closing care gaps, you can play an even more influential role in improving outcomes and demonstrating value across the healthcare system. This transition represents not just a change in how care is measured, but an opportunity for you to help shape what high quality diabetes care looks like in a digital future.

Join this exclusive 30‑minute exclusive session, lead by expert Marie Frazzitta, DNP, FNP‑C, PMHNP, CDCES, MBA, who will provide a high‑level overview of how digital quality measures, CGM data, and value‑based care are transforming diabetes care delivery and reporting. You’ll learn how these shifts create new opportunities for diabetes health professionals to lead, demonstrate value, and shape the future of technology‑enabled diabetes care.
Marie is a nurse practitioner and healthcare strategist with experience across health systems, payer organizations, and digital diabetes technology. She brings a rare cross‑sector perspective to diabetes care, quality improvement, and digital health, helping organizations modernize chronic disease management and prepare for digital quality transformation.
Marie’s work spans clinical leadership, population‑health strategy, value‑based care performance, and digital innovation. Board certified as a Family Nurse Practitioner and trained as a Psychiatric Mental Health Nurse Practitioner, she integrates whole‑person care, behavioral science, and technology‑enabled practice to strengthen patient engagement and improve outcomes.
She has published and presented nationally on diabetes care (Type 1, Type 2, and diabetes in pregnancy), diabetes technology, digital quality measures, and patient engagement strategies including motivational interviewing.
Marie contributes to national initiatives through advisory and leadership roles with organizations such as the Association of Diabetes Care & Education Specialists (ADCES), the American Diabetes Association (ADA), and National Committee for Quality Assurance (NCQA), supporting workgroups and committees focused on diabetes care, digital quality measurement, and innovation.

🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00

Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!

Author: Beverly Thomassian, RN, MPH, CDCES, BC-ADM
CEO: DiabetesEd Services
At my recent physical, my provider noticed the crumpled list of questions I was clutching and asked to see my list of concerns. I reluctantly handed it over, explaining they were just mental notes for myself. My practitioner—usually kind and curious—scanned the paper, handed it right back, and said, “I can’t address all of these today. Pick your top three.”
What happened over the past 6 months that impacted our connection?
What if the greatest future contribution of artificial intelligence (AI) in health and diabetes care isn’t replacing healthcare professionals—but giving us back the time and emotional energy to be fully present with the people we serve?
That is one of the most inspiring messages from the recent Diabetes Care article, “Diabetes Care in 2050: A Human-Centered Road Map From Time in Range to Time in Happiness.”
Rather than imagining a future in which technology overshadows human relationships, the authors envision a healthcare system where AI and digital innovation reduce administrative burdens, personalize care, and allow clinicians to focus on what matters most: meaningful human connection.
Healthcare has become increasingly complex, especially in diabetes. New medications, continuous glucose monitoring, automated insulin delivery systems, and sophisticated data platforms are being released at a record-breaking pace. Yet many healthcare professionals find themselves spending more time documenting, interpreting data, and navigating electronic health records than they do sitting face-to-face with the people they care for.
The article argues that by 2050, AI could be tasked with managing much of this cognitive and administrative workload—organizing information, identifying trends, generating documentation, and supporting clinical decision-making. This shift has the potential to return our attention to listening, coaching, and partnering with people living with diabetes.
One idea that particularly resonated with me is the authors’ proposal to redefine diabetes success from solely focusing on clinical metrics such as hemoglobin A1C, Time in Range, blood pressure, and cholesterol levels to a more human-based metric. While clinical measures are important, they don’t fully capture what matters to the individual.
The vision presented in this paper expands our perspective from “Time in Range” to “Time in Happiness.”
As caregivers, we can shift to a goal not solely focused on numbers, but to help people spend more of their time free from the constant burden of managing diabetes.
As diabetes healthcare professionals, this concept aligns beautifully with person-centered care. Our role has never been to prescribe medications or interpret glucose reports.
We help people navigate fear, frustration, competing priorities, financial barriers, family responsibilities, and the emotional weight of living with a chronic condition.
However, it can create conditions that allow those human qualities to flourish by handling repetitive tasks and providing clinicians with timely, actionable insights.
AI should augment—not replace—clinical judgment.
Imagine beginning a visit with an AI-generated summary highlighting glucose trends, medication-taking patterns, potential barriers, and individualized recommendations based on current evidence.
Instead of spending the first ten minutes gathering information, you could begin with a meaningful question such as, “What has been the hardest part of managing your diabetes since we last met?” Technology becomes the assistant, allowing the healthcare professional to remain the healer.
Instead of staying late to chart, your conversation with the individual is transcribed in the patient’s own words and language and uploaded to the electronic medical record.

Administrative responsibilities continue to grow while visit lengths frequently remain unchanged. Documentation, prior authorizations, inbox management, and data review play a major role in clinician fatigue. If AI can safely automate many of these tasks, healthcare professionals may experience greater professional satisfaction and more opportunities to practice the type of medicine that originally inspired them to enter healthcare. Caring for others becomes less about managing paperwork and more about building relationships.
Of course, the authors wisely acknowledge that this future is not guaranteed. Achieving a human-centered healthcare system will require deliberate implementation, ethical attention, equitable access to technology, and healthcare reforms that value people over processes. AI is only a tool. Its value depends on how thoughtfully we integrate it into care. The article calls for co-designed solutions that include healthcare professionals and people living with diabetes in shaping these innovations, so technology improves rather than fragments the care experience.
This future vision reinforces a belief I’ve held throughout my career: diabetes care is not about choosing between technology and interpersonal connection. It is about using technology to strengthen human connections. Every innovation should ultimately answer one question: Does this help us better understand, support, and partner with the person sitting in front of us?
As we look toward the future, I hope AI becomes the quiet partner working behind the scenes—organizing information, identifying patterns, and simplifying complexity—while healthcare professionals do what only humans can do: listen deeply, inspire hope, foster trust, and walk alongside people through life’s challenges. If we achieve that balance, perhaps by 2050 we really will measure success not only by Time in Range but also by Time in Happiness. And that is a future worth building.
Founder & CEO: DiabetesEd Services
Diabetes Care in 2050: A Human-Centered Road Map From Time in Range to Time in Happiness Guy Fagherazzi, Emmanuel Cosson, Chantal Mathieu, Renza Scibilia, Kyle Jacques Rose, Kamil Armacky, Korey Hood, Bart Torbeyns, Elise Bismuth, Stéphane Besancon, Pratik Choudhary, Roberto Mallone, Pierre-Yves Benhamou, Dianna J. Magliano, Carine de Beaufort, Jean-Pierre Riveline, Michael Joubert; Diabetes Care in 2050: A Human-Centered Road Map From Time in Range to Time in Happiness. Diabetes Care 2026; dci260059. https://doi.org/10.2337/dci26-0059
🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00
Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!

Author: Ashlie Sabourin
Customer Advocate
Artificial Intelligence (AI) for CDCES and BC-ADM Exam Prep – Benefits & Cautions
AI for CDCES and BC-ADM exam prep is becoming increasingly popular among healthcare professionals and certification candidates. Tools such as ChatGPT and Copilot can help learners create study guides, generate practice questions, explain difficult concepts, and organize educational materials.
Used thoughtfully, AI for CDCES and BC-ADM exam prep can be a valuable study aid. However, AI-generated content may be outdated, oversimplified, incomplete, or incorrect. AI works best as a supplemental learning tool alongside evidence-based resources, clinical judgment, and trusted educational materials.
The strongest learners combine AI-assisted exam preparation with critical thinking, information verification, and trusted clinical references.
The most important factors affecting the quality of AI-generated content is the quality of the prompt.
Vague prompts often produce broad, generic results. More specific prompts typically generate more focused and useful responses.
“Make me a diabetes study guide.”
The more context you provide, the more useful the output is likely to be.
Healthcare recommendations change over time. Including the current year in your prompt can help focus AI responses on more recent information.
Examples:
This simple step may reduce the likelihood of receiving outdated information.
The safest and most effective ways to use AI is by working directly from trusted educational content.
Examples include:
Rather than asking AI to search broadly for information, consider providing educational content directly and asking AI to help organize it.
For example:
A webinar transcript discussing insulin management.
Example prompts:
This approach allows learners to maximize the value of trusted educational resources while tailoring materials to their preferred learning style.
One of the most powerful uses of AI for exam preparation is creating active learning tools.
Many learners spend hours rereading notes. While review is important, active recall often improves retention more effectively.
Active recall requires learners to retrieve information from memory rather than simply rereading content.
AI can quickly generate:
Front:
What is the ADA Time in Range (TIR) goal for most adults with diabetes?
Back:
Greater than 70% of glucose readings between 70–180 mg/dL.
Front:
A patient using basal insulin has fasting glucose within target but elevated post-meal readings. What might be some treatment options?
Back:
To improve postprandial glucose, review MNT, activity levels, consider adding a GLP-1 or GLP-1/GIP combo medication, or bolus insulin before meals.
Example prompts:
Download our Medication PocketCards
AI is most effective when used interactively rather than passively.
Instead of accepting the first response, continue the conversation.
Helpful follow-up questions include:
These types of questions encourage deeper understanding and clinical reasoning rather than memorization alone.
AI can also help:
AI tools may draw information from a variety of online sources. Whenever possible, direct AI to prioritize reputable clinical references.
Examples include:
You can also include instructions such as:
Providing source guidance often improves the quality and reliability of AI-generated content.
AI-generated content should always be reviewed critically.
AI can occasionally provide inaccurate information with a high degree of confidence. Independent verification is especially important in healthcare education.
Always verify:
Continue to rely on trusted resources such as:
AI can be a valuable addition to your study toolkit when used thoughtfully and responsibly. By combining AI-assisted learning with trusted educational resources, evidence-based references, and critical thinking, learners can create personalized study materials while maintaining confidence in the accuracy and quality of the information they are reviewing.
The goal is not to replace traditional study methods—it is to enhance them.
🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00
Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!
Artificial intelligence (AI) is transforming diabetes prevention, monitoring, and management. As clinical care tasks and data grow exponentially, providers and individuals living with or at risk for diabetes seek ways to optimize timely, personalized, and effective care.1
AI can support this by enabling screening and imaging, risk predictions, AI-enhanced devices, individualized self-management tools, and clinical support.1 Because diabetes care requires individualized rather than one-size-fits-all treatment, integrating clinical, behavioral, and lifestyle data with AI could reduce routine data review, allowing providers to focus on meaningful conversations, shared decision-making, and personalized goal-setting. Used thoughtfully, AI could support clinical expertise and strengthen, not replace, the human element that is essential to effective care.

Author: Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
For decades, diabetes management relied on retrospective data, reviewing information such as lab results, glucose logs, food records, and medication histories to understand what had occurred. When I began in diabetes care over 20 years ago, we had only a few computer-generated reports and logbooks, and gathering and interpreting the data took time. We used checklists to ensure labs, vitals, risk assessments, and preventive measures were completed.
Now, rather than spending appointment time on checklists and handwritten logs, we can start each visit with a comprehensive summary of key diabetes assessments and clinical care tasks. Integrated reminders, concise summaries, and data platforms enable a much quicker transition to intervention discussions.
In practice, we already use platforms like Dexcom Clarity, Abbott LibreView, MiniMed CareLink, Tandem source, Omnipod Glooko, and Tidepool, which use algorithms to analyze glucose patterns and generate insights for clinicians and device users. Data from CGMs, activity trackers, sleep monitors2, and insulin delivery systems can reveal patterns that were nearly impossible to detect within the time constraints of 20 years ago. Conversations now shift from, “What happened here?” to, “What can we learn from these patterns for future considerations?”
During diabetes care visits, AI-powered ambient scribes (such as Dragon CoPilot, Ambience, Heidi AI, Freed, and other EHR-embedded scribes)3 can assist with documentation by summarizing key elements of the conversation. Because this significantly reduces time spent at the computer, providers can focus more on the individual. Based on my experience, this reduction in administrative burden also enables deeper shared decision-making regarding management adjustments, health behavior changes, barriers, and concerns.
Following the visit, ambient scribes can organize information into a clear, personalized after-visit summary that reinforces key recommendations, action steps, and education provided. However, accuracy remains a concern; large language models (LLMs) generating discharge summaries were shown to contain errors, though the risk of harm was assessed as low1.
From a dietitian’s perspective, LLMs can also help create individualized nutrition resources tailored to food choices, culture, and clinical needs. Instead of providing a generic meal plan, tools like ChatGPT, Gemini, and EHR-embedded AI can generate meal ideas, recipe modifications, or personalized food lists. A recent study using ChatGPT (GPT-5 version)4 found that ChatGPT could approximate carbohydrate targets but had limitations in accuracy when balancing multiple dietary requirements simultaneously (such as carbohydrate percentage, total calories, and meal planning constraints).
LLMs’ effectiveness and accuracy can improve with well-designed prompts that provide clinical context, specific goals, and defined constraints, but clinical review and oversight are recommended. Prompts may often require refinement, and LLMs simply react to input words, leading to hallucinations5.
AI can extend support beyond the diabetes clinical visit with tracking tools that can provide users with summarized insights. Examples of food photo interpretation and glucose trackers include SNAQ, UnderMyFork,6 Glucose Buddy, GlucoAI, and Freestyle Libre Assist. While these apps can still have errors and inaccuracies, these tools may help with understanding meal components beyond carbohydrates, such as the impacts of food type and protein, fat, and fiber content.
ChatGPT, Gemini, and Claude are also being used for carbohydrate counting, and a recent study compared these LLMs with expert dietitians for carbohydrate estimation from meal photographs. Across 30 meals, dietitians had the lowest mean absolute error (13 ± 10 g), followed by ChatGPT (20 ± 18 g), Claude (23 ± 21 g), and Gemini (28 ± 26 g). L.7
In addition to tracking, between-visit AI support may improve outcomes. A recent randomized controlled trial8 found that a fully automated AI-driven Diabetes Prevention Program achieved weight loss and glycemic improvements similar to those of a human coach in adults with prediabetes and overweight or obesity.
However, AI has important limitations. It may generate inaccurate recommendations, overlook complex medical conditions, or fail to recognize economic, cultural, and racial disparities or emotional and behavioral challenges that influence diabetes self-management.1
Future AI-enabled clinical diabetes care could feature the use of a digital twin, a virtual model that simulates an individual’s glucose patterns, meals, activity, medications, sleep, genetics, and prior treatment responses to predict the physiological impacts of proposed changes.1
For example, clinicians might ask, “Based on this person’s metabolic history and patterns, what if we reduce breakfast carbohydrates, start a GLP-1 medication, modify insulin, or adjust activity?” In these scenarios, the digital twin can inform what-if considerations.
A recent systematic review9 of 4 studies involving 2,662 adults with type 2 diabetes found that digital twin-based interventions improved glycemic management and reduced treatment burden, including significant reductions in diabetes medications and improvements in time in range.
While these findings are promising, evidence remains limited, and further research is needed to validate these applications in diverse populations.
Artificial intelligence is evolving diabetes care.
AI-powered tools help organize health data, reduce administrative tasks, identify patterns and make predictions, personalize nutrition and treatment strategies, and extend support between visits.
While AI enhances diabetes management and prevention, its value is supported by clinical expertise, compassion, and personalized care.
The Academy of Nutrition and Dietetics and the American Society of Nutrition published a 2026 resource guide for practitioners. This guide provides basic definitions of the different types of AI models and how these types are translated into practice. This publication links to a few educational and professional development courses specific to AI and valuable for all diabetes care providers. Check it out here.
 Author: Christine Craig, MS, RDN, CDCES
Author: Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00
Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!


