
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Today, is Winter Solstice, when we experience the shortest day and longest night of the year. From here we will slowly gain more light each day, marking this as an astronomical shift from darkness to light.
For many cultures, winter solstice marks a day of rebirth, saying goodbye to the past year and a universal deep breath for the future.
Susan Cooper penned a beautiful poem about winter solstice that we are thrilled to share with you below. Given this incredibly difficult year, it seems especially poignant and I hope you enjoy the read.
As a special bonus this year, Jupiter and Saturn will align in the night sky today, December 21st, in an event astronomers call the “great conjunction.”
The last time Jupiter and Saturn came this close was 1623, but that conjunction was too near the sun to be seen by Earthlings. 1226 is actually the most recent time such close conjunction of Jupiter and Saturn was visible to humans.
You can watch it online with webcasts from The Virtual Telescope Project, Slooh at NASA Telescope here.
And so the Shortest Day came and the year died
And everywhere down the centuries of the snow-white world
Came people singing, dancing
To drive the dark away
They lighted candles in the winter trees
They hung their homes with evergreen
They burned beseeching fires all night long
To keep the year alive
And when the new year’s sunshine blazed awake
They shouted, reveling
Through all the frosty ages you can hear them
Echoing behind us—listen!
All the long echoes, sing the same delight
This Shortest Day
As promise wakens in the sleeping land:
They carol, feast, give thanks
And dearly love their friends
And hope for peace.
And now so do we, here, now,
This year and every year.
Welcome, Yule!
This poem is available as a children’s hardcover with beautiful watercolor illustrations by Carson Ellis.

As health care professionals and Diabetes Specialists, how do we keep up to date with all the latest information on diabetes and COVID-19?
How do we prepare people with diabetes for the possibility of a COVID-19 infection and hospitalization?
To help, we have put together a list of free resources by category so you can easily access important and relevant information about COVID-19.
Plus, we have updated our Sick Days / COVID-19 and Diabetes Handout that we invite you to share with colleagues and people living with diabetes.
COVID-19, Sick days & Diabetes: Handout
Updated to reflect the latest CDC guidelines. Reviews sick day instruction for people with diabetes, plus COVID-19 specific information.
Article Library Sections

We have updated this content based on the ADA 2021 Standards of Care.
We are living longer and more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering a reduction of medication and insulin therapy intensity. The older population has unique issues and special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Topics include:
Join us live on December 23rd at 11:30 am (PST)
This course is included in: Level 2 – Standards of Care Intensive. Purchase this course individually for $29 or the entire bundle and save 70%.
Enroll in our entire Level 2 – Standards of Care Intensive to join us for the below for Live Webinar Updates. All courses air at 11:30 a.m. (PST)
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Blood glucose levels provide an immediate snapshot of a person’s state of inflammation, with or without diabetes.
According to recent research findings, admission glucose is also an excellent predictor of COVID-19 related deaths and severity of illness.
Researchers in Spain retrospectively evaluated over 11,000 patients positive with COVID on admission in 109 hospitals throughout Spain. They also evaluated admission blood glucose levels and their findings were startling.
The researchers were also able to stratify the risk of death based on admissions glucose levels.
For all 11, 000 patients admitted with COVID in this study, the mortality rate was 20%.
For patients with admission glucose of 140 – 180, the mortality rate increased to 33%.
The mortality rate skyrocketed to 41% if admission glucose was 180 mg/dL or greater.
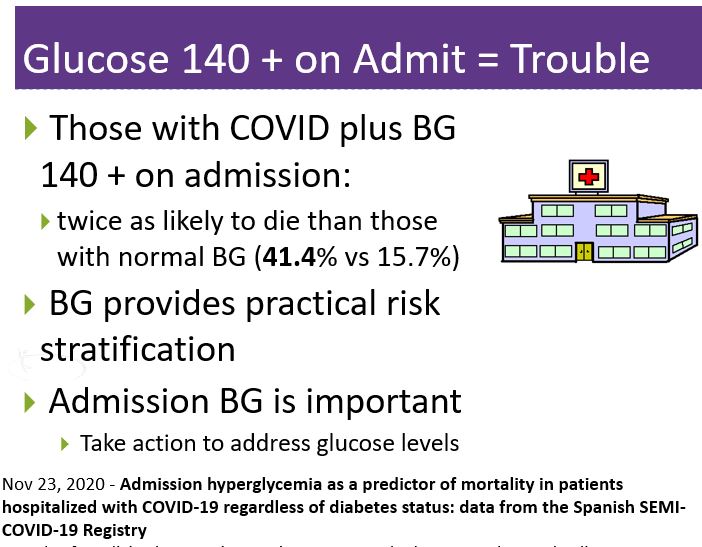
Read More Here Admission hyperglycemia as a predictor of mortality in patients hospitalized with COVID-19 regardless of diabetes status: data from the Spanish SEMI-COVID-19 Registry. November 2020
Annals of Medicine by Francisco Javier Carrasco-Sánchez, MD, PhD, and colleagues. Nov 23, 2020
Recorded & Ready for Viewing
Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM, has completely updated this critical presentation, to bring health care professionals up-to-date on the current state of COVID and its impact on diabetes care. She summarizes key information including critical teaching points and management strategies for people with diabetes who develop a COVID-19 infection.
Topics Include:
Join us to learn critical information about Diabetes and COVID Management

Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JL is a 78-year-old with type 2 diabetes who has been taking metformin 1000mg BID for the past year. She checks her BG each morning and says it usually ranges from 100 – 138. Her most recent A1c came back at 9.6% and the provider started her on dapagliflozin (Farxiga) 5 mg daily two days ago. JL arrives at the clinic in a panic and says she has been checking her blood glucose 3 times a day it has “jumped up to 236 and 242”. The diabetes specialist double-checked and verified random glucose of 249. What is the best explanation?
Click here to test your knowledge!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Drew Mendelow, 13, felt overwhelmed with all the new information he had to learn to navigate his new diagnosis of type 1 diabetes.
Since Drew already knew how to code games, he thought he could design an app that would help him track his insulin, blood sugars and carbohydrates consumed.
He ended up creating an app that would help with bolus insulin calculations and provide a shareable log.
Within months of diagnosis, Drew launched his new app T1D1. T1D1 stands for Type 1 diabetes from Day 1.
To make sure the T1D1 app is available for anyone with new type 1 diabetes, Drew is adamant his app remains free. “I want to make sure everyone can really use it.”
The T1D1 app has been rigorously evaluated by the Children’s Hospital in Washington D.C. It not only passed this detailed vetting process, but the team at Children’s Hospital is also recommending it to people and families with a new type 1 diagnosis.
Many people with type 1 diabetes are started on CGM and insulin pumps, eventually. These devices help determine insulin bolus doses. But for those who don’t yet have access to these tools or can’t afford these devices, the T1D1 app is very useful and designed by someone living with type 1 diabetes every day.
This easy-to-use app is available on google play or for iOS users. The set-up is straight forward and intuitive.
Users plug in their blood glucose and carbs, and the app determines how much insulin to take for any given meal or snack based on the user’s profile. This app greatly simplifies the process of determining needed insulin dose, plus keeps a record of glucose levels, carbs consumed and insulin delivered. In addition, this record can be easily emailed to providers or concerned family members.
Users can personalize their individual glucose target, the insulin-to-carb ratio at each meal /snack, and the correction ratio. They can also enter their most commonly consumed foods with custom serving sizes and carb amount, to create a personalized food library.
I love that this app is free, but users have the option to support Drew’s contribution to making a new diagnosis with type 1 just a little easier!

Perfect for those planning to take the CDCES / BC-ADM or for those who want to learn more about the technology used to manage diabetes.
As Diabetes Care and Education Specialists, we are expected to have expertise in diabetes technologies to improve person-centered care and optimize outcomes.
Yet, when it comes to insulin pumps, sensors, and calculations many of us feel overwhelmed and unsure about diabetes technology management. Coach Beverly created this 2-part Technology Toolkit to provide you with critical information on Insulin Pumps, Calculations, and Continuous Glucose Monitors.
If you want cutting edge information on diabetes technology, problem-solving, and using a formula to determine appropriate insulin dosing, we highly recommend this toolkit.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Given that people with diabetes might have a drink or two during the season, we thought that this was an important topic to discuss further. Our December 1st Question of the week was a question of alcohol consumption during the holidays. Over 60% of respondents, chose the best answer.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JL has diabetes and injects insulin 2-3 times a day. JL is at a holiday party and is struggling with wanting a holiday spirit. Which of the following is the best approach for JL?
Answer Choices:
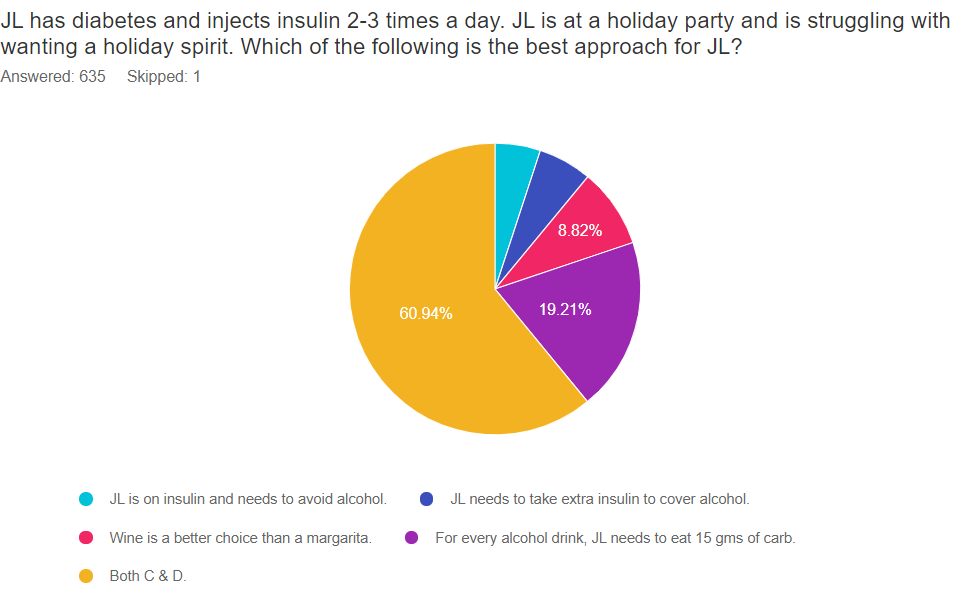
As shown above, the most common choice was option 5, the second most common answer was option 4, then option 3, then option 2, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam questions won’t have 2 right answers, but alcohol and diabetes is expected content on the exam.
Answer 1 is incorrect. 5.04% chose this answer. “JL is on insulin and needs to avoid alcohol.” Based on the American Diabetes Association standards of care, people with diabetes on insulin can include alcohol as part of their meal plan.
The current recommendations are; women with diabetes limit their alcohol consumption to one drink a day or less and men with diabetes limit consumption to two or fewer drinks a day.
There are side effects to consider. Alcohol can worsen triglyceride levels, intensify neuropathic pain, and lead to unwanted weight gain. Plus, it can increase the risk of hypoglycemia. So, the decision to consume spirits is a person-centered decision, based on individual needs and health status.

One serving of alcohol =
Answer 2 is incorrect. 5.98% of you chose this answer. “JL needs to take extra insulin to cover alcohol.” Alcohol can cause hypoglycemia for hours after consumption. Alcohol metabolism in the liver delays the release of glycogen stores and can lead to low circulating glucose levels. Some people with type 1 diabetes may even need to adjust their insulin dose at a meal if consuming alcohol.
People with type 1 diabetes need to be extra cautious if their before bed glucose is elevated after consuming alcohol. Before giving extra insulin to treat nighttime high glucose, remind them that glucose levels will trend down overnight with alcohol on board, and they probably don’t need that extra bolus of insulin.
Answer 3 is correct, but so is answer 4. “Wine is a better choice than a margarita.” Wine is a better choice since it does not have all the extra sugar and carbohydrates of a margarita. Wine consumption has a more predictable outcome whereas figuring out how much carbohydrate is in a margarita can be tricky. Mixed sugary drinks may cause blood glucose levels to rise initially than drop, later on, making management more difficult.
Answer 4 is correct, but so is answer 3. “For every alcohol drink, JL needs to eat 15 gms of carb.” Since we know that alcohol can lead to hypoglycemia for those who are on insulin therapy or take a sulfonylurea, coupling each of their favorite adult beverages with 15 gms of carb can prevent unwanted hypoglycemia.
Another issue is that the signs of hypoglycemia can mirror the signs of intoxication. Encourage people to keep a close eye on their CGM or meter results when imbibing. And include their friends in on helping to detect and treat hypoglycemia to keep safe during celebrations.
Answer 5 is correct. 60.94% chose this answer. “Both C & D.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“This is one of the best review courses I’ve ever taken.”
“I learned so much from the CDCES Exam Prep Toolkit. I now have an assessment after taking the practice exam on the areas I need to focus my studying.”
Student Feedback

Whether you are preparing for the CDCES or BC-ADM exam, this test-taking toolkit is designed to prepare you for success. This toolkit includes two courses with over 200 practice questions to help you prepare and simulate the exam. Plus, we have added a FREE bonus course, Language, and Diabetes – What we say matters. Coach Beverly added this course because she believes it contains critical content for the exam and for our clinical practice!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
A 12-year-old with new-onset hyperglycemia presents to the Emergency Room with positive urine ketones and blood sugar of 283. What action is required most immediately?
Click here to test your knowledge!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
To celebrate National Diabetes Month, we are excited to provide you with a bunch of helpful resources to help get the word out.

ADA’s FREE Living with Type 2 Diabetes Program: ADA’s program includes six digital, printable journeys to teach how to live well with diabetes; a monthly e-newsletter with tips, stories, and more resources; six free issues of the Diabetes Forecast® magazine; access to an online community and local events. (The program is available in both English and Spanish).
Insulin Cost Savings Toolkit Resource Page – A complete listing of low cost insulin options.
ADA Diabetes Education Library Offers over 170 topics on diabetes that are searchable by topic and language. A treasure trove of educational info.
CDC Diabetes Prevention Program Curricula and Handouts This site offers excellent resources for those interested in offering Diabetes Prevention Education.
National Diabetes Education Program is an online library of resources compiled by the NDEP to help provide accurate information and support for people living with prediabetes and diabetes.
Type 1 Diabetes Resource Page – Includes is a list of helpful online resources for Type 1 Diabetes. It include sites for national organizations like the American Diabetes Association (ADA), sites for diabetes interest groups, and other participant organizations that provide helpful diabetes tips and opportunities to join online groups.

See Full Free Resource Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.