“What Year ADA Standards Should I Study?”
 Given my seven-time experience taking the CDCES exam, I can say with complete conviction that being familiar with the American Diabetes Association (ADA) Standards of Care is one of the most important and essential strategies to prepare for exam success. More importantly, this evidence-based guidebook is crucial for providing the best clinical and person-centered care, with close attention to the Social Determinants of Health.
Given my seven-time experience taking the CDCES exam, I can say with complete conviction that being familiar with the American Diabetes Association (ADA) Standards of Care is one of the most important and essential strategies to prepare for exam success. More importantly, this evidence-based guidebook is crucial for providing the best clinical and person-centered care, with close attention to the Social Determinants of Health.
Taking CDCES in January or February 2025?
If you are taking the exam in January or February 2025 and you have already read the 2024 ADA Standards cover-to-cover, you are all set. It takes at least a year for the exam writers to include new questions culled from the ADA Standards. Having said that, if there are any critical new guidelines that impact clinical care, education, or treatment of diabetes, that content can be included in the exam that same year. From my review of the 2025 Standards, there are no critical new clinical guidelines that need immediate adoption into practice. One important caveat to consider: if you are relying on last year’s standards, make sure to read through the Summary of Revisions section included in the Standard of Care, so that you that latest information under your belt.
Taking the Exam in 2025 Sometime?
On the other hand, if you are taking the exam in 2025 and haven’t reviewed the ADA Standards in the past, I recommend a thorough review of the most recent ADA Standards. You can access the ADA Standards on our CDCES Coach App and the ADA Website at www.diabetes.org.
Short on Time?
In case of emergency, there is a shorter version of the ADA Standards called the Abridged version for Primary Care Providers that highlights critical clinical content. The abridged version is usually released in February by the ADA. It can also be used as a quick review after you have read the document in full. Again, after successfully passing the exam seven times, my advice is to be familiar with the ADA Standards of Care in its entirety.
Study Strategies from Coach Beverly
- Plan on reading one Standard a week, highlighting key content areas – you CAN do it!
- Review the most challenging Standards several times to allow the content to sink in.
- Provide a short in-service on an aspect of a Standard you found particularly difficult.
- Join our Level 2 – ADA Standards 2025 Update and Online Series, where Coach Beverly breaks down the critical content to help you focus your limited study time.
- Create old-fashioned flashcards and quiz yourself while walking.
- Join our FREE Prep for CDCES Certification Webinars.

“What Counts Toward My 1000 Hours and How Can I Accumulate Hours?”
If you are trying to accumulate practice hours, you may be wondering what counts toward the 1000 hours of Diabetes Self Management (DSME) Experience.
Below is an excerpt from the CBDCE Exam Handbook regarding what hours count towards this 1000-hour DSME requirement:
- Assessment: The participant’s DCE needs are identified. This process is led by the participant with the assessment and support of the educator.
- Education and Care Plan: The participant’s individualized education and care plan is developed. The plan reflects the participant’s self-management goals and current evidence and practice guidelines and includes criteria for evaluating outcomes.
- Interventions: The specialist delivers intervention options to assist the participant in meeting self-management goals.
- Ongoing Support: The specialist provides options for ongoing support and resources. The support option(s) is selected by the participant to best meet their self-management goals.
- Participant Progress: The specialist will monitor and communicate whether the participant is achieving their self-management goals and other outcome(s) to evaluate the effectiveness of interventions. Additional assessments are based on the participant’s needs across the lifespan.
- Documentation: The specialist documents the assessment, education plan, intervention, and outcomes in the participant’s health record.
- Services Development/Administration: Development and administrative activities performed as part of DSMES services.
Is There a Tracker to Document My Hours?
To help you keep track of your hours, we created the Diabetes Management Hours Tracker. The column “Remaining Hours Needed” is a formula that is tied to “Hours Completed” so be sure to only put numbers in the hour’s column so the formula automatically deducts those hours to get the remaining hours you need. Make sure you let your supervisor know you are tracking your hours, since they will need to attest and verify DSME hours completed.
Tracking your activities and hours consistently is key and this Hours Tracker excel sheet can help you tally your hours, while working toward your goal of becoming a CDCES.
Work Experience Hours: How To Gain Hands-On Experience
Meeting the 1,000-hour requirement for the Certified Diabetes Care and Education Specialist (CDCES) exam is achievable with a variety of approaches. The hours needed can include volunteer or paid hours. Below are some practical ways to accumulate hours if you are not able to accrue enough hours in your current work environment.
- Volunteer in Community Health Programs or Diabetes Camps
- Offer your expertise to local diabetes prevention or management programs, such as YMCA’s Diabetes Prevention Program, Diabetes Camps, or similar initiatives.
- Shadow a Diabetes Education Specialist in your Community
- Search for already existing diabetes programs in your community and volunteer to help with their diabetes program. This might even evolve into a paid position in the future.
- Join ADCES Local Networking Diabetes Groups
- Networking with diabetes educators in your area can lead to opportunities to gain hours and possible future employment.
- Join Diabetes Support Groups
- Facilitate or assist with support groups in person or online to provide guidance and share educational resources.
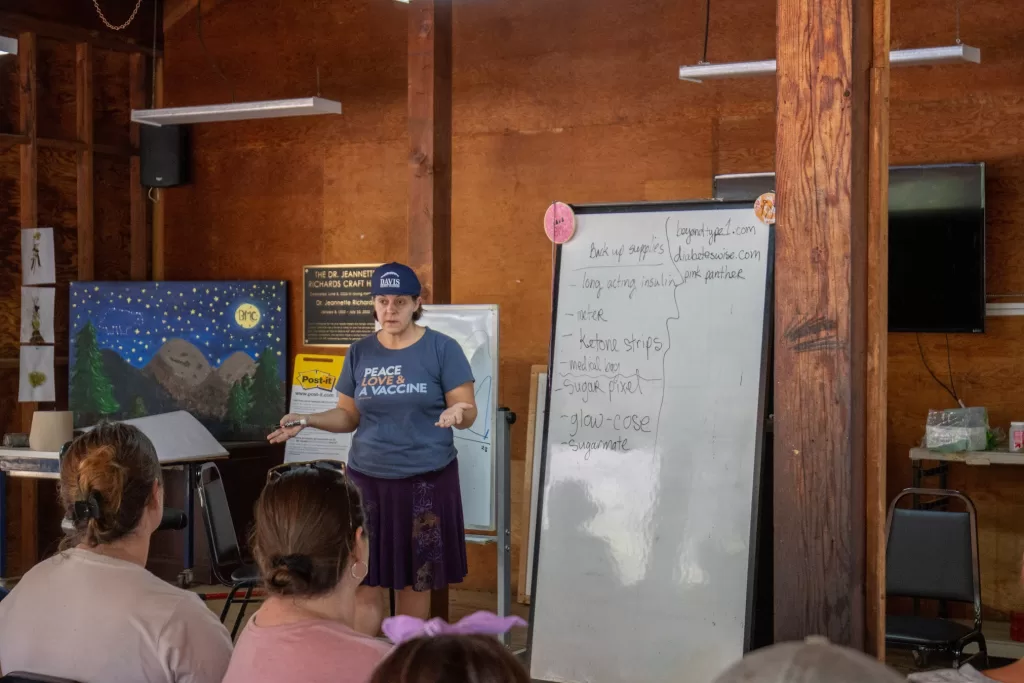
- Offer Educational Workshops or Webinars
- Create and present workshops for people with diabetes or even train other healthcare professionals about aspects of diabetes management.
- Collaborate with Pharmacies
- Partner with local pharmacies to provide diabetes education to people picking up diabetes-related medications or supplies.
- Participate in Health Screenings or Free Health Clinics
- Assist with diabetes screenings, provide educational coaching at health fairs, or sign up to provide diabetes coaching at your local free clinic.
- Support Long-Term Care Facilities
- Offer diabetes-related education to staff and residents in long-term care or assisted living facilities.
- Write or Develop Educational Content
- If you’re skilled in writing, contribute to diabetes educational materials for local papers and websites. You can count the time spent on research and content development towards your hours.
Resources to help Prepare for CDCES Exam
Are you Interested in Starting a Mentorship Program?
As part of our Bridge Program, Coach Beverly wants to support YOUR efforts to mentor a new generation of Diabetes Care and Education Specialists. If you are a mentor, we are offering significant discounts off of our Diabetes Boot Camp or Virtual 3 Day Program for groups of mentees who are practicing in underserved regions of our country. Please email us for more information at [email protected]