Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

November is Diabetes Awareness Month, and there’s no better way to expand your knowledge than by attending one of the many free webinars hosted by Diabetes Education Services. These webinars provide essential insights that can help you stay informed and empowered in your journey to becoming a Diabetes Educator.
This month, join Coach Beverly—a trusted expert in diabetes education—as she leads a series of engaging and informative webinars. With her wealth of experience and passion for helping others, Coach Beverly will guide you through topics ranging from the basics of diabetes to more advanced management strategies. Don’t miss these valuable opportunities to learn from one of the top educators in the field. Be sure to register for the upcoming sessions and make the most of Diabetes Awareness Month!


Register above or simply visit DiabetesEd.net and browse the Free Resources Tab. While most webinars are available to attend at no cost, you have the option to purchase the session if you wish to earn Continuing Education (CE) credits.
For more information or any questions, please email [email protected].
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our Level 4 | The Impact of Adverse Childhood Experiences on Health awards 1.0 CPEUs in accordance with the Commission on Dietetic Registration’s CPEU Prior Approval Program.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
How You Can Participate:
Share your plans and activities for National Diabetes Month by Submitting the activities form by November 29th. Tell us what you’re doing to spread awareness, provide education, or advocate for diabetes prevention and management. Your ideas have the power to motivate others to take action, and we’d love to amplify your voice by sharing your initiatives on our social media channels or website.

As we celebrate National Diabetes Month, we have the opportunity to inspire change, build stronger communities, and help individuals affected by diabetes lead healthier lives. Whether you’re just starting your diabetes education journey or have been in the field for years, your contributions are vital to improving diabetes care. By sharing your plans and participating in our giveaway, you’re helping to spread the word and create a more informed, supportive environment for everyone impacted by diabetes.
We can’t wait to hear from you and see how you’re making a difference this National Diabetes Month. Together, we can create a lasting impact!
Submit your Diabetes Ed Awareness activity by Nov 29th and enter to win—we look forward to celebrating your efforts with you! 💙
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on practicing cultural humility. 92% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Question: You are caring for ML, a Latinx person with newly diagnosed diabetes about lifestyle modifications. ML mentions that traditional family dinners are a central part of their daily routine.
How can the educator apply cultural humility in their approach to diabetes education to support ML’s dietary needs and preferences?
Answer Choices:
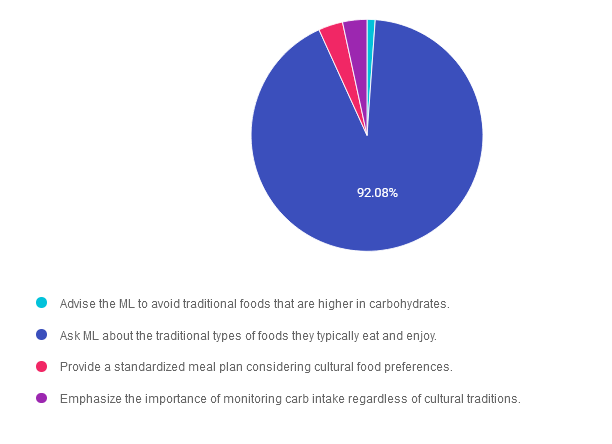
Answer 1 is incorrect. 1.13% chose this answer. “Advise the ML to avoid traditional foods that are higher in carbohydrates.” This answer was obviously incorrect to the majority of you, which highlights your knowledge of cultural humility and person-centered care. Even though it is important to monitor carbohydrates, we can’t disregard their cultural traditions. By considering the importance of cultural humility and person-centered care, we can help individuals determine a meal planning approach that works for them.
Answer 2 is correct. 92.08% of you chose this answer. “Ask ML about the traditional types of foods they typically eat and enjoy.” Yes, one of the main tenants of MNT is to “maintain the pleasure of eating.” This BEST answer highlights the importance of cultural humility and person-centered care. By considering the importance of cultural humility and person-centered care, we can help individuals determine a meal planning approach that works for them. Great job!
Answer 3 is incorrect. About 3.40% of respondents chose this. “Provide a standardized meal plan considering cultural food preferences.” One of the main tenants of MNT, is that there is NO one standardized meal plan. Our goal is to create an individualized meal plan in collaboration with the individual, based on their values, needs and preferences. By considering the importance of cultural humility and person-centered care, we can help them determine a meal planning approach that works for them.
Finally, Answer 4 is incorrect. 3.40% chose this answer. “Emphasize the importance of monitoring carb intake regardless of cultural traditions.” Our goal is to create an individualized meal plan in collaboration with the individual, based on their values, needs and preferences. Even though it is important to monitor carbohydrates, we can’t disregard their cultural traditions. By considering the importance of cultural humility and person-centered care, we can help individuals determine a meal planning approach that works for them.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness. Topics covered include:
We will review sample test questions, and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Intended Audience: This FREE webinar is designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in achieving excellence in diabetes care and becoming Certified Diabetes Care and Education Specialists®.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 7 times. She is a nationally recognized diabetes expert for over 25 years.
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

LC is a 49-year-old living with type 2 diabetes and reports during their appointment they have stopped their statin because of concern over risk of type 2 diabetes incidence with statin use.
Using the ADA Standards of Care as a guide, what would be the best response to LC concerns?
Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness. Topics covered include:
We will review sample test questions, and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Intended Audience: This FREE webinar is designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in achieving excellence in diabetes care and becoming Certified Diabetes Care and Education Specialists®.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 7 times. She is a nationally recognized diabetes expert for over 25 years.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

This November, many of you celebrated National Diabetes Awareness Month to highlight the importance of education, prevention, and support for those living with diabetes. We asked you to describe your activities and the responses we received were both inspiring and uplifting. They showcased the diverse ways you dedicated your time and efforts to support diabetes awareness and advocacy.
We were inspired by individuals across the nation who stepped up to make a difference in their communities. From hosting local events to sharing resources online, your efforts highlight the power of collective action in spreading awareness and offering support.
Educating and Raising Awareness
Supporting Patients and Communities
Promoting Healthy Lifestyles
“Our team participated in a community walk to raise awareness and promote physical activity.”
Advancing Professional Knowledge
Creative Engagements
These heartfelt stories reflect the diverse and impactful ways individuals contributed during National Diabetes Awareness Month, showing that even small acts can make a big difference.
Thank you to everyone who participated in our “Share Your Action to Win” giveaway! 🎉 Your stories and actions to raise awareness for National Diabetes Month have been truly inspiring. 💙
Raffle Winners:
Chasity Eversole, Lauren Cline, Vanita Achar, Jennifer Kutrovac, Majorie Smith, Heidi Bates, Anissa Avanesyan, Inuka Midha, Diana Morrow, Alexander Ray, Colleen Dougherty, Monica Astorga
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

Dawn Desoto RD, CDCES, celebrates the fall and winter season with a collection of recipes that nourish and heal. Dazzle your taste-buds and energize your gut bacteria with this delicious and seasonal compilation.
Choose a pie pumpkin and wash it’s exterior. Cut in half lengthwise and remove the seeds and pulp. Roast in your oven for about 45 minutes at 350 degrees F.
Simply peel away the skin from the flesh and toss the pumpkin pulp into your food processor or blender.
Ingredients:

In a large bowl, whisk eggs and pumpkin puree together. Add the rest of the ingredients and whisk them together while slowly pouring in the evaporated milk.
Pour mixture into pie crust. Bake in the oven for 20 minutes at 390 degrees, reduce oven to 350 degrees and bake for another 45 – 60 minutes until inserted toothpick comes out clean. Store in the refrigerator overnight.

Mix the melted butter or coconut oil, walnuts, and cinnamon together and pour over the apples. Bake in the preheated oven until the apples are soft, about 20 – 30 minutes. Stir once during the baking.

Pour the wine into a small saucepan along with the orange zest and juice and all of the spices
Bring almost to a boil and add the pear halves. Turn down the heat and let the pears simmer gently for 20 – 30 minutes, or until they have slightly softened. Carefully turn the pears over a few times throughout the cooking time to ensure they color evenly. When the pears are cooked remove them from the wine and place them on plates. Add a tablespoon of yogurt to each plate and sprinkle with toasted almonds.

Combine coconut milk, oats, chia, banana, maple syrup in a pint-sized jar and stir. Top with blueberries and coconut. Cover and refrigerate overnight. Heat up and sprinkle with walnuts and cinnamon in the morning.
285 calories, 6 gm protein, 57 gms carbohydrate, 7 gms fiber 6 gm fat
To add more color into our diets, I am sharing my Spinach Pomegranate Salad recipe

Toss the spinach leaves with the rest of the ingredients. Serves 4
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on type 1 and food insecurity. About two thirds of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
AR is an 8 year old with type 1 diabetes who has a CGM but still uses insulin injections due to lack of insurance coverage. AR’s parents struggle with food insecurity and some days AR only has school provided breakfast and lunch. You notice he is experiencing level 1 hypoglycemia frequently around 6pm.
What is the best first intervention?
Answer Choices:
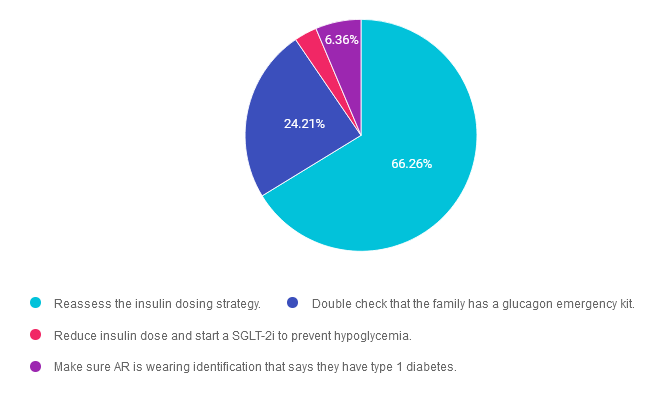
Answer 1 is correct. 66.26% chose this answer. “Reassess the insulin dosing strategy.” YES, this is the BEST answer. GREAT JOB! It appears that JR may not have adequate food intake on some days in the early evening hours. To compensate for this decreased food intake, the insulin dose will most likely need to be lowered to prevent dinnertime hypoglycemia. Of course, we would also need to connect AR and their family with social services and other resources.
Answer 2 is incorrect. 24.21% of you chose this answer. “Double check that the family has a glucagon emergency kit.” Although it is important for all people living with type 1 diabetes to have a glucagon rescue medication, the first goal is to prevent severe hypoglycemia. In this situation, the first action is to adjust the insulin dose to prevent dinnertime hypoglycemia. Of course, we would also need to connect AR and their family with social services and other resources.
Answer 3 is incorrect. About 3.18% of respondents chose this. “Reduce insulin dose and start a SGLT-2i to prevent hypoglycemia.” In this situation, the first action is to adjust the insulin dose to prevent dinnertime hypoglycemia. SGLT-2’s are off label for people living with type 1 diabetes and since AR is not in a stable situation, this would not be a good time to evaluate the effectiveness of adding on an SGLT. Of course, we would also need to connect AR and their family with social services and other resources.
Finally, Answer 4 is incorrect. 6.36% chose this answer. “Make sure AR is wearing identification that says they have type 1 diabetes.” Yes, wearing identification is recommended for people living with type 1 diabetes, but more importantly, we want to prevent hypoglycemia. In this situation, the first action is to adjust the insulin dose to prevent dinnertime hypoglycemia. Of course, we would also need to connect AR and their family with social services and other resources.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness. Topics covered include:
We will review sample test questions, and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Intended Audience: This FREE webinar is designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in achieving excellence in diabetes care and becoming Certified Diabetes Care and Education Specialists®.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 7 times. She is a nationally recognized diabetes expert for over 25 years.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
You are caring for ML, a Latinx person with newly diagnosed diabetes about lifestyle modifications. ML mentions that traditional family dinners are a central part of their daily routine.
How can the educator apply cultural humility in their approach to diabetes education to support ML’s dietary needs and preferences?
Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness. Topics covered include:
We will review sample test questions, and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Intended Audience: This FREE webinar is designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in achieving excellence in diabetes care and becoming Certified Diabetes Care and Education Specialists®.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 7 times. She is a nationally recognized diabetes expert for over 25 years.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on helping someone flustered and late to an appointment. 73% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is a 22-year-old living with type 1 diabetes who arrives late for their appointment and seems out of sorts. When looking at the ambulatory glucose profile, you notice that time in range is less than 40% and coefficient of variation is also over 40%. You remember from a previous visit that JR had experienced almost half a dozen adverse childhood experiences and had elevated diabetes distress.
Based on this information, what is the next best step?
Answer Choices:
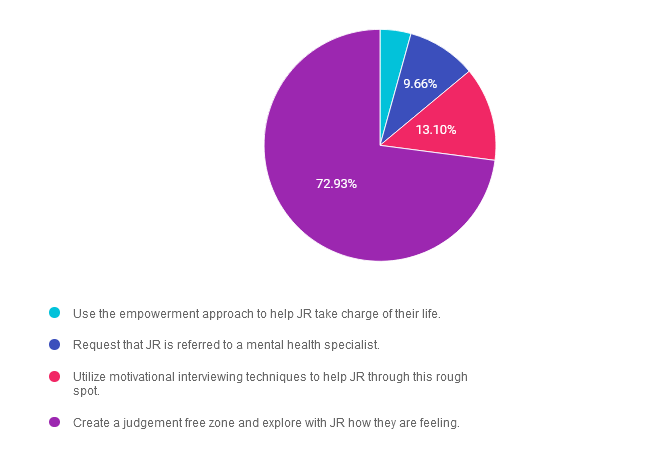
Answer 1 is incorrect. 4.31% chose this answer. “Use the empowerment approach to help JR take charge of their life.” Even though the empowerment approach can be used as a tool to help people take a more active role in their self-care, given JR’s level of distress, this would not be the best approach. We will need to first assess the situation and discuss next steps as part of collaborative care.
Answer 2 is incorrect. 9.66% of you chose this answer. “Request that JR is referred to a mental health specialist.” Even though JR is clearly struggling with diabetes distress and being “out of sorts’, this does not automatically mean he needs to be referred to a mental health specialist. We will need to first assess the situation and discuss next steps as part of collaborative care.
Answer 3 is incorrect. About 13.10% of respondents chose this. “Utilize motivational interviewing techniques to help JR through this rough spot.” Even though motivational interviewing can be used as a tool to help people take a more active role in their self-care, given JR’s level of distress, this would not be the best approach. We will need to first assess the situation and discuss next steps as part of collaborative care.
Finally, Answer 4 is correct. 72.93% chose this answer. “Create a judgement free zone and explore with JR how they are feeling.” YES, GREAT JOB. We need to provide a safe environment for JR to have the freedom to share what is happening in their life and support them in taking action to decrease their distress.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Adverse childhood experiences (ACE) are associated with an increased risk of diabetes, heart disease, cancer & a variety of other health consequences for adults. This session reviews how diabetes care & education specialists can provide screening, assessment, & trauma-informed care to individuals who experienced ACEs & are living with toxic stress. We will explore strategies to address ACES & improve outcomes for individuals & communities. Throughout, we will focus on supporting self-care with a focus on recognizing & promoting resilience.
Objectives:
Learning Outcome:
Participants will identify how trauma can impact diabetes and self-management along with strategies to support hope when working with people with diabetes.
Target Audience:
This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs/RDNs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions. The practice areas for RDs/RDNs for CDR reporting are healthcare, preventative care, wellness, and, lifestyle along with, education and research.
CDR Performance Indicators:
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 15 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert.
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our Level 4 | The Impact of Adverse Childhood Experiences on Health awards 1.0 CPEUs in accordance with the Commission on Dietetic Registration’s CPEU Prior Approval Program.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.