
The new ADA Standard on Chronic Kidney Disease and Risk Management outlines importance of measuring kidney function and the impact on our practice and quality of life for people living with diabetes.
I wanted a better understanding of these renal metrics since they are such an important indicator of risk, treatment and health outcomes.
Based on my review, we share four findings and take a closer look at renal function tests and their significance.
4 Kidney function findings that impact our practice:
- Predicts CV Disease – albuminuria is associated with kidney disease and is a predictor of cardiovascular events, so it is important to measure and accurately evaluate urine protein and take action to prevent cardiovascular events.
- SGLT2’s slow progression of chronic kidney disease and decrease risk of CV events. Therefore SGLT2 therapy is recommended for those with a GFR of 25 or greater with urinary albumin creatinine 300mg/g or more.
- Frequency of measure depends on findings. People with diabetes need to have their Urinary Albumin Creatinine Ratio (UACR) measured yearly. However, if the UACR is 30mg/g or greater and their GFR is less than 60, kidney function should be tested twice a year.
- Measure of success: If urine albumin severely increased, the goal is to provide an intervention and decrease albuminuria by 30%.
What is albuminuria?
Albuminuria is a general term that means there is significant protein in the urine. In the old days, we would order a 24 hour urine collection to determine the degree of albumin in the urine. We used the terms microalbuminuria to describe slightly elevated protein levels and macroalbuminuria to describe significant urine albumin. Since those terms are no longer used, how do we describe how much protein is in the urine? Now, we use Urinary Albumin Creatinine Ratio (UACR) to determine levels of urine protein and their significance.
What Exactly is Urinary Albumin Creatinine Ratio (UACR)?
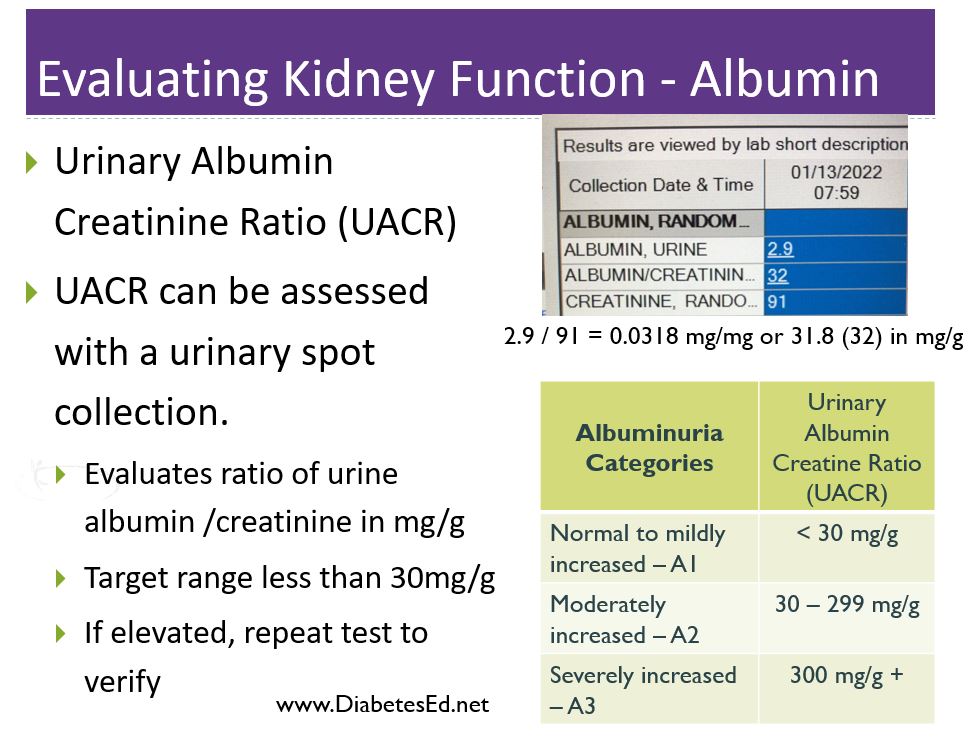
Simply put, UACR is ratio of urine albumin to urine creatinine. The UACR is usually already calculated on the lab report, but using this lab example to the right, the albumin is 2.9 and the urine creatinine is 91. To determine the UACR, you would divide albumin by creatinine, 2.9 / 91 = 0.0318 in mg/mg. Then convert it to mg/g by moving the decimal point over three places, or 31.8 (32) in mg/g.
The reason this value is reported as a ratio as opposed to just urine albumin, is to account for the concentration and hydration status of the individual which improves accuracy.
UACR is an important measure of kidney health and the goal is to measure it yearly and if elevated, more frequently.
Any level of UACR 30mg/g or greater indicates kidney damage and requires prompt protective action by the health care team.
Action to protect the kidney include lifestyle interventions, blood pressure (ACE or ARB) and blood glucose management, along with use of SGLT-2 Inhibitors, GLP-1 RA’s and possibly finerenone.
Testing for UACR and Confirming Results
Testing for UACR is fairly easy. The ADA has approved using urine dipstick or a urine sample to calculate the UACR, However, according to the standards, two of three tests need to be positive to confirm diagnosis within a 3 to 6 month period before confirming diagnosis of moderate or severe albuminuria. Exercise within 24 h, infection, fever, congestive heart failure, marked hyperglycemia, menstruation, and marked hypertension may elevate UACR independently of kidney damage.
How to test for GFR
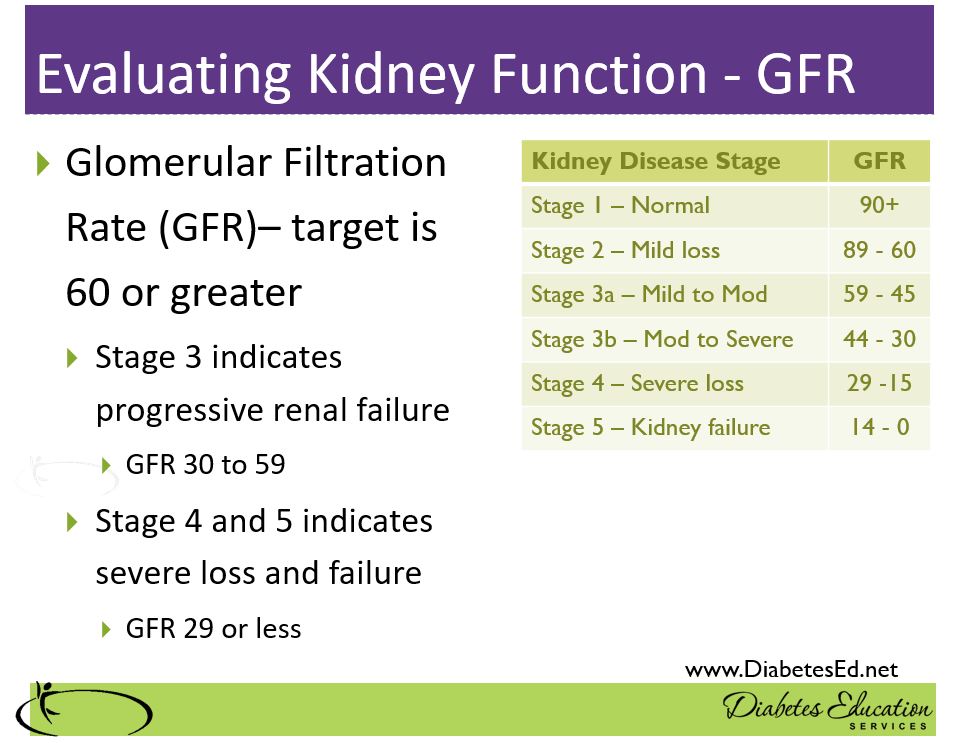
Another measure of kidney function is the Glomerular Filtration Rate. The result is derived from a complicated mathematical calculation, using the person’s creatinine and other data. For this reason, it’s often called an estimated GFR or eGFR. People with diabetes need their creatinine evaluated yearly to determine their GFR. Here is a link to an eGFR Calculator.
For people with diabetes, we start keeping a close eye on the GFR when levels start dropping below 60. As with UACR, heath care providers need to take preventive action to maintain kidney function and protect GFR through lifestyle and medications.
In conclusion, as diabetes specialists, being familiar with the results of these kidney health measures help us advocate on behalf of people with diabetes. Making sure our health care organizations are regularly measuring kidney function and taking action to protect these amazing filtering units can save lives and improve quality of life.