
Management of Hyperglycemia in Type 2 Diabetes, 2018. https://doi.org/10.2337/dci18-0033
A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD).
This new consensus statement is a summary of findings based on a comprehensive literature search of peer reviewed articles published from 2014 to February 2018.
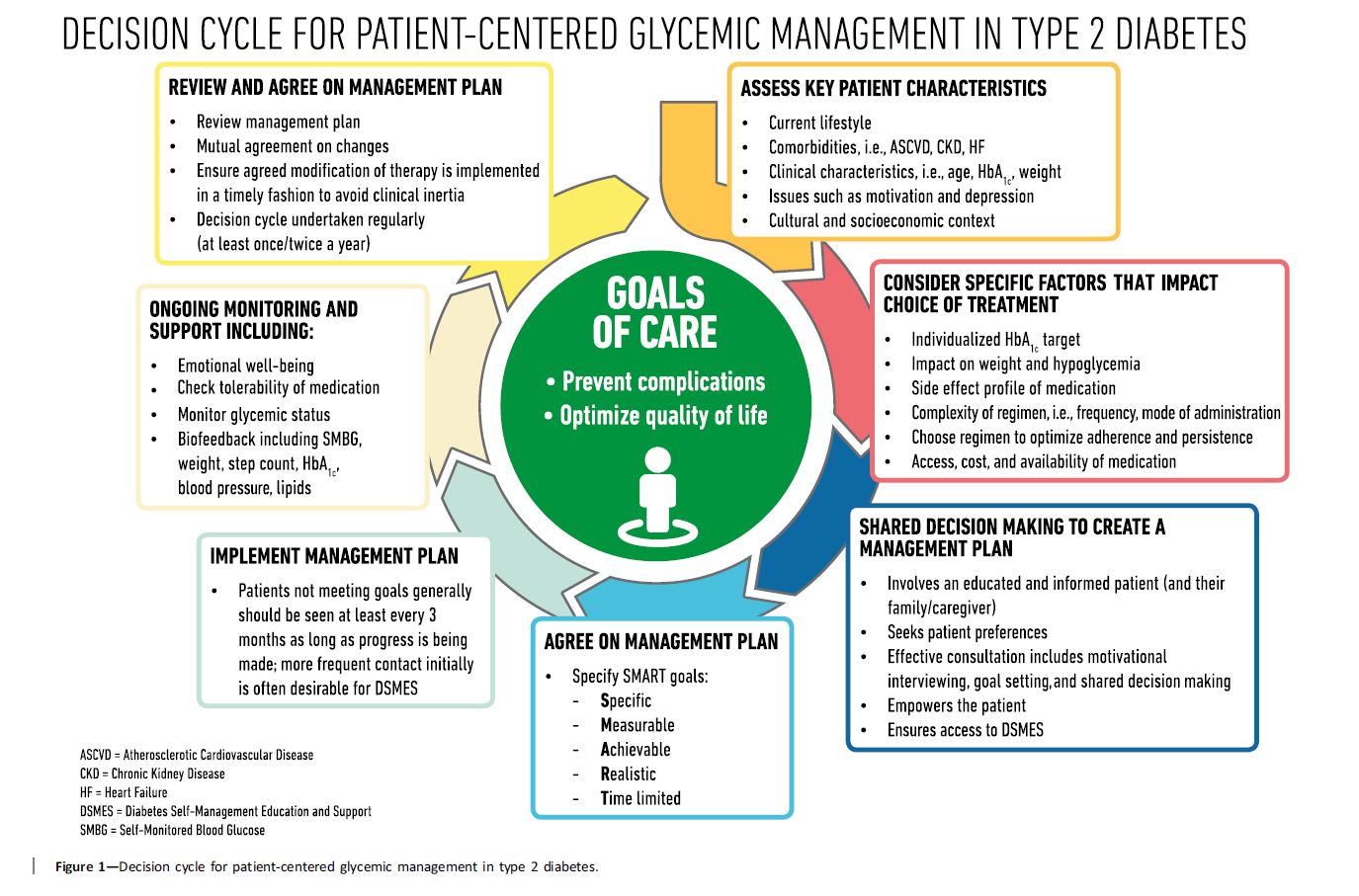
Here are some key statements from the Principles of Care Section that really stood out. In addition, the Decision Cycle Chart below, is an excellent summary of person centered considerations to determine the best path to take when deciding upon lifestyle and medication therapy.
Key concepts that I found intriguing and helpful from this section:
- The greatest risk reduction comes from improving poor glycemic control. There is a more modest risk reduction with near normalization. This statement helps educators to prioritize where we put our efforts, knowing that the greatest health improvement comes when we help PWD with higher A1cs levels get to target.
- Keep the care centered around the person with diabetes. Acknowledge that they often have multi-morbidities and other real barriers to self care including cost of therapy, mental health issues and competing priorities.
- All people with type 2 diabetes need access to ongoing DSMES Programs. DSMES programs are evidenced based and cost effective. They promote medication adherence, healthy eating, activity and improve self-efficacy.
Therapeutic inertia, also called clinical inertia, refers to the lack of action even when blood glucose targets are above target. This is something I have frequently seen in my diabetes practice. A common example of this is a PWD on two to three different diabetes medication and basal insulin, with an A1c is greater than 9%, yet no changes in therapy are made for months or years. The causes of this inertia may complex, but can be a result of the provider, person with diabetes or the health care system.
To avoid or stop Clinical inertia, here are recommended strategies:
- Evaluate the PWD medication taking persistence. Are they taking their medication at least 80% of the time? If not, explore the barriers and engage in problem solving.
- Reassess and modify treatment at least every three months to avoid clinical inertia
- Engage multidisciplinary teams that include nurse practitioners, pharmacists and diabetes educators who can suggest or implement therapeutic changes to improve A1c levels.
- Create coordinated care models, which include the person with diabetes as an active participant.