
For last week’s practice question, we quizzed participants on what steps to address an elevated A1C. 56% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Question: KT is a 17-year-old with newly diagnosed diabetes and an A1C of 13.6%. The provider starts KT on 30 units of basal insulin and 10mg empagliflozin (Jardiance). KT is asked to get C-peptide levels checked and their C-peptide level is 0.9 ng/mL.
Based on this information, what is the next most important step?
Answer Choices:
- Add bolus insulin and stop empagliflozin
- Discuss the importance of starting CGM
- Evaluate auto immune markers
- Decrease basal insulin and start metformin
Getting to the Best Answer
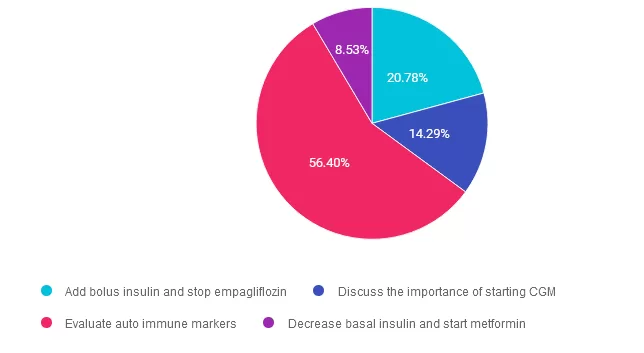
Answer 1 is incorrect. 20.78% chose this answer. “Add bolus insulin and stop empagliflozin.” Since KT’s c-peptide level is 0.9ng/mL, it is between the normal range of 0.5 and 2.0 nanograms per milliliter (ng/mL). This means there is no urgent need to start KT on basal bolus insulin therapy, as long as we have basal insulin on board and we are monitoring blood glucose levels. According to ADA Standards, we can continue both the basal insulin and Jardiance and even consider adding metformin or a pediatric approved GLP-1 RA. Once we have the type 1 antibody results, we can determine best path forward.
Answer 2 is incorrect. 14.29% of you chose this answer. “Discuss the importance of starting CGM.” While it is important to monitor glucose levels, this is not the MOST important next step. To determine if KT has type 1 diabetes, we quickly need to evaluate if they are experiencing autoimmunity by testing for these; autoantibodies to insulin, GAD, islet antigen 2, ZnT8. If one or more of these comes back positive, it verifies KT has immune mediated type 1 diabetes and has a clear indication for basal bolus insulin therapy.
Answer 3 is correct. About 56.40% of respondents chose this. “Evaluate auto immune markers.” YES, GREAT JOB. This is the best answer. Since KT’s C-peptide is within the normal range, we need to evaluate immune markers. To determine if KT has type 1 diabetes, we quickly need to evaluate autoimmunity by testing for; autoantibodies to insulin, GAD, islet antigen 2, ZnT8. If one or more of these comes back positive, it verifies KT has immune mediated type 1 diabetes and is an indication for basal bolus insulin therapy.
Finally, Answer 4 is incorrect. 8.53% chose this answer. “Decrease basal insulin and start metformin.” Given that KT’s C-peptide is in normal range, we certainly could consider adding metformin and decreasing basal insulin. However, KT may still be in the honey moon phase and may be producing some insulin. For this reason, to determine if KT has type 1 diabetes, we quickly need to evaluate autoimmunity by testing for; autoantibodies to insulin, GAD, islet antigen 2, ZnT8. If one or more of these comes back positive, it verifies KT has immune mediated type 1 diabetes and is an indication for basal bolus insulin therapy.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join us live on December 17, 2024 for our
Meds Management Update for Type 2 Diabetes
Level 2 Standards of Care Intensive
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes guidelines. She kicks it off with a brief overview of the different classes of medications and then uses a case study approach to apply the ADA algorithm.
Objectives:
- Describe the role of Diabetes Care & Education Specialists in advocating for optimal therapeutic approaches.
- Discuss the application of the new ADA/EASD Guidelines to improve glucose and reduce CV and renal risk.
- List strategies to initiate & adjust oral & injectable therapy using a person-centered approach.
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our Level 2 | Meds Management Update for Type 2 Diabetes awards 1.5 CPEUs in accordance with the Commission on Dietetic Registration’s CPEU Prior Approval Program.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.