

For last week’s practice question, we quizzed participants on determining if someone has diabetes based on ADA Standards. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 47 years old and who just got lab results from their annual physical. Their fasting plasma glucose result was 129 mg/dL. The provider is worried that JR might have diabetes and sent them to back to the lab to check their A1C, which came back 6.4%.
According to the 2024 ADA Standards, to most accurately assess if JR has diabetes, which of the following follow-up actions is recommended?
Answer Choices:
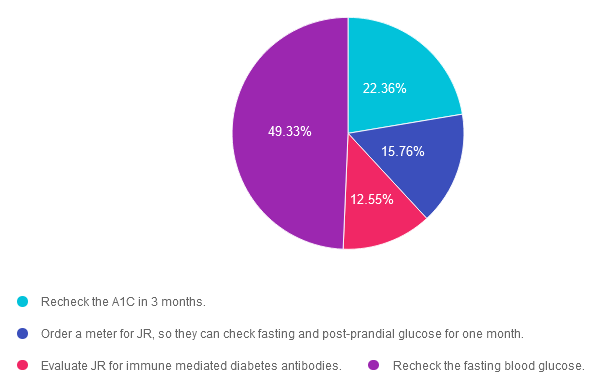
- Recheck the A1C in 3 months.
- Order a meter for JR, so they can check fasting and post-prandial glucose for one month.
- Evaluate JR for immune mediated diabetes antibodies.
- Recheck the fasting blood glucose.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 22.36% chose this answer. Recheck the A1C in 3 months. According to ADA Standard 2 on Diagnosis and Classification of Diabetes, “if an individual has discordant results from two different tests, then the test result that is above the diagnostic cut point should be repeated, with careful consideration of factors that may affect measured A1C or glucose levels.” Since JR’s fasting BG test result meets the diagnostic threshold of equal to or greater than 126 mg/dL, we would need to repeat the fasting test, to see if the second lab would confirm diagnosis. We would also consider factors (hemoglobinopathies, lab issues) that might be affecting the accuracy of the A1C result.
Answer 2 is incorrect. 15.76% of you chose this answer. Order a meter for JR, so they can check fasting and post-prandial glucose for one month. Since home glucose meters have limited accuracy, they are not recommended for diagnosis of diabetes. In addition “if an individual has discordant results from two different tests, then the test result that is above the diagnostic cut point should be repeated, with careful consideration of factors that may affect measured A1C or glucose levels.” Since JR’s fasting BG test result meets the diagnostic threshold of equal to or greater than 126 mg/dL, we would need to repeat the fasting test, to see if the second lab would confirm diagnosis. We would also consider factors (hemoglobinopathies, lab issues) that might be affecting the accuracy of the A1C result.
Answer 3 is incorrect. About 12.55% of respondents chose this. Evaluate JR for immune mediated diabetes antibodies. In this case study, JR does not present with risk factors or symptoms of immune mediated type 1 diabetes or LADA. However, since their fasting blood sugar meets the diagnostic threshold for diabetes, we need to redraw JR’s fasting blood glucose, to confirm (or dispute) diagnosis.
Finally, Answer 4 is correct. 49.33% chose this answer. Recheck the fasting blood glucose. YES – GREAT JOB, According to ADA Standard 2 on Diagnosis and Classification of Diabetes, “if an individual has discordant results from two different tests, then the test result that is above the diagnostic cut point should be repeated, with careful consideration of factors that may affect measured A1C or glucose levels.” Since JR’s fasting BG test result meets the diagnostic threshold of equal to or greater than 126 mg/dL, we would need to repeat the fasting test, to see if the second lab would confirm diagnosis. We would also consider factors (hemoglobinopathies, lab issues) that might be affecting the accuracy of the A1C result.
On the other hand, if an individual has discordant results from two different tests, then the test result that is above the diagnostic cut point should be repeated, with careful consideration of factors that may affect measured A1C or glucose levels. The diagnosis is made based on the confirmatory screening test. For example, if an individual meets the diabetes criterion of A1C (two results ?6.5% [?48 mmol/mol]) but not FPG (<126 mg/dL [<7.0 mmol/L]), that person should nevertheless be considered to have diabetes.We hope you appreciate this week’s rationale!
Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.