
For last week’s practice question, we quizzed participants on what is the best intervention for euglycemic DKA. 55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Question: KT is a 54-year-old, who presents to the emergency room with nausea and vomiting. KT weighs 58kg, has been feeling very tired and has diabetes and hypertension.
Meds include: losartan, metformin, and empagliflozin.
Labs: Na 140, K 4.0, Chloride 99, Bicarb 15, Glucose 189, Anion Gap 26, pH 7.1 and positive urine ketones
After infusing 2 liters of normal saline, what would be the best intervention for KT?
Answer Choices:
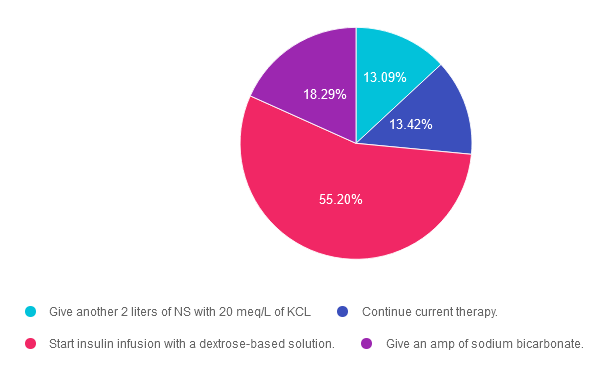
- Give another 2 liters of NS with 20 meq/L of KCL
- Continue current therapy.
- Start insulin infusion with a dextrose-based solution.
- Give an amp of sodium bicarbonate.
Getting to the Best Answer
Answer 1 is incorrect. 13% chose this answer. “Give another 2 liters of NS with 20 meq/L of KCL.” Since KT has already received 2 liters of normal saline for fluid resuscitation, the next step is to provide a solution with glucose, and possibly potassium depending on KT’s electrolyte levels. Even with euglycemic DKA, KT has depleted their glycogen stores and the cells are in desperate need of glucose for two reasons; to stop burning fat for fuel and to replete glycogen stores.
Answer 2 is incorrect. 13.42% of you chose this answer. “Continue current therapy.” While this answer is tempting, it does not provide a clear plan of action for KT. The only therapy this is currently being provided is an IV of normal saline. Even though KT’s blood glucose is less than 200mg/dL, in order to stop ketosis, we need to start IV insulin along with 5-10% dextrose to preserve blood glucose and replace glycogen stores.
Answer 3 is correct. About 55.20% of respondents chose this. “Start insulin infusion with a dextrose-based solution.” YES! This is the best answer. The next step is to provide an IV solution with 5-10% glucose, and possibly potassium depending on KT’s electrolyte levels. Even with euglycemic DKA, KT has depleted their glycogen stores and the cells are in desperate need of glucose for two reasons; to stop burning fat for fuel and to replete glycogen stores. In addition, in order to stop ketosis, we need to start IV insulin at a few units an hour!
Finally, Answer 4 is incorrect. 18.29% chose this answer. “Give an amp of sodium bicarbonate.” Since KT is in acidosis, this is a tempting answer. However, the acidosis will usually be corrected with administration of IV fluids and insulin. If not, and the pH is still below 7.0, bicarb administration may be considered.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Keynote Presentation on DKA & Euglycemic DKA at
16th Annual Conference
Expanding the Universe of Diabetes Care hosted by CA ADCES
May 3-4th at Universal City, CA

Beverly will be speaking on DKA and EDKA on Saturday – May 4, 2024 at 11:30 am
Below is Saturday’s schedule of topics and flyer for more information. We hope to see you there!
>>Register for the Conference
>>Flyer for Event
- Discover the secrets to a successful and sustainable Diabetes Education Program – Tony Song, MBA
- Exercise Success Part 3 & 4 – Jacqueline Thompson, MS, RD, CDCES, MES
- Dynamic Duo: Registered Dietitian & Pharmacist Co-Appointments in Diabetes Care – Christal Pham, PharmD, APh, CDCES, Melanie Barbee, MS, RDN, CDCES, DipACLM
- Advocacy Update: Breakdown the Barriers to Evidence-Based Diabetes Care – Teresa Martin MS RDN CDCES LD
- New criteria and treatment guidelines for DKA, Euglycemic DKA, and HHS – Beverly Thomassian, RN, MPH, CDCES, BC-ADM
- Exercise Success Part 4 – Jacqueline Thompson, MS, RD, CDCES, MES
- Diabetes Technology: Understanding the Differences in the Latest CGMs and Pumps – David Ahn, MD
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- July 2026 e-News | Meet ADA Educator of the Year & Clinical Updates
- Rationale of the Week | Sudden Onset of Hyperglycemia – Why?
- Sizzling Summer Sale | 20% off Online Courses | July 13th
- Question of the Week | Best Action for Steroid-Induced Hyperglycemia?
- Rationale of the Week | Diabetes and Sleep Health
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.