

For our June 29th Question of the Week, 56% of respondents chose the best answer. Since people with diabetes will often need to undergo a procedure or surgery that requires they be NPO, we wanted to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: AR is living with type 2 diabetes, has an A1c of 7.4%, and takes metformin 1000 BID and 60 units of glargine at bedtime. AR is admitted to the hospital overnight for early morning surgery.
According to ADA Guidelines, what adjustment in his diabetes medications are needed to prepare for a safe surgery?
Answer Choices:
- Hold the evening metformin and glargine the night before surgery to prevent perioperative hypoglycemia.
- Hold morning metformin the day of surgery and give about 40 units of bedtime glargine the night before surgery.
- Hold metformin 3 days before surgery and give 60 units of bedtime glargine the night before surgery.
- Hold the metformin the day before surgery and give the glargine the morning of surgery to prevent perioperative hyperglycemia.
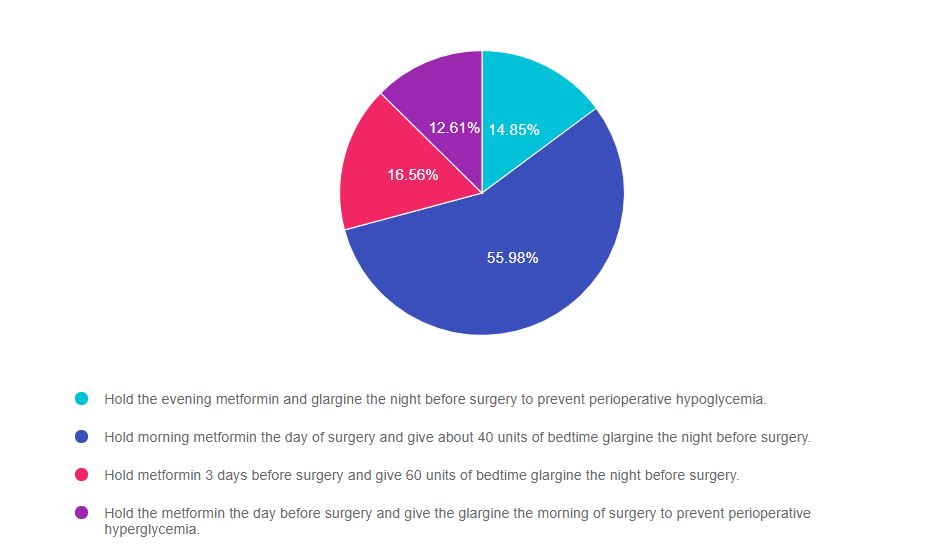
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 1, and finally option 4.
Getting to the Best Answer
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to be familiar with knowledge of preparation for surgery or other procedures that require the person with diabetes to be in a fasting state.
Answers & Rationale
Answer 1 is incorrect, 14.85% chose this answer, “Hold the evening metformin and glargine the night before surgery to prevent perioperative hypoglycemia.” Since AR has type 2 diabetes, even though AR is going to be NPO in preparation for surgery, AR can still take the evening metformin and most of the glargine. If AR holds both of these treatments, there is a high chance that AR will wake up with elevated morning blood sugars, which could delay surgery or lead to a hyperglycemic crisis.
Answer 2 is correct, 55.98% of you chose this answer, “Hold morning metformin the day of surgery and give about 40 units of bedtime glargine the night before surgery.” GREAT JOB. This is the BEST answer. According to the ADA, since AR has type 2 diabetes, even though AR is going to be NPO in preparation for surgery, AR can still take the evening metformin and 60-80% of the evening glargine. Since AR’s A1c is 7.4%, we give 60% of the usual 60 units of glargine (~40 units), so that AR wakes up with glucose close to the target, but not too low to cause hypoglycemia.
Answer 3 is incorrect, 16.56% of you chose this answer, “Hold metformin 3 days before surgery and give 60 units of bedtime glargine the night before surgery.” Since AR has type 2 diabetes, even though AR is going to be NPO in preparation for surgery, there is no reason for AR to hold the metformin for 3 days. AR can take metformin the day before surgery and resume metformin the evening after surgery if kidney function is stable. Since AR’s A1c is 7.4%, we give only 60% of the usual 60 units of glargine (~40 units), so that AR wakes up with glucose close to the target, but not too low to cause hypoglycemia.
Answer 4 is incorrect, 12.61% of you chose this answer “Hold the metformin the day before surgery and give the glargine the morning of surgery to prevent perioperative hyperglycemia.” Since AR has type 2 diabetes, even though AR is going to be NPO in preparation for surgery, there is no reason for AR to hold the metformin the day before surgery. AR can take metformin the day before surgery and resume metformin the evening after surgery if kidney function is stable. As far as changing glargine administration time to the morning to lower surgical glucose, this would not be advised since it would be a departure from AR’s usual routine and could cause unwanted glucose fluctuations.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our
Level 2 | Hospitals & Hyperglycemia Standards | 1.5 CEs

Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control and outline practical strategies to achieve targets in the inpatient setting. We incorporate the latest ADA Standards and provide links to resources and inpatient management templates.
Topics include:
- The impact of hyperglycemia in the hospital setting.
- The importance of inpatient glucose control.
- Three strategies to get glucose to goal in the hospital setting.
See Full Calendar for upcoming webinars and Virtual Courses.
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.