
For last week’s practice question, we quizzed participants on ADA recommendations for metformin while pregnant. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Question: KR has polycystic ovary syndrome and takes metformin 850mg twice daily. KR just discovered they are 4 weeks pregnant. Fasting glucose is 103 mg/dl.
According to ADA Guidelines, if prediabetes diagnosis is confirmed, what is the next step?
Answer Choices:
- Continue metformin through first trimester.
- Start basal insulin, stop metformin.
- Add human basal bolus insulin.
- Stop metformin, start sulfonylurea.
Getting to the Best Answer
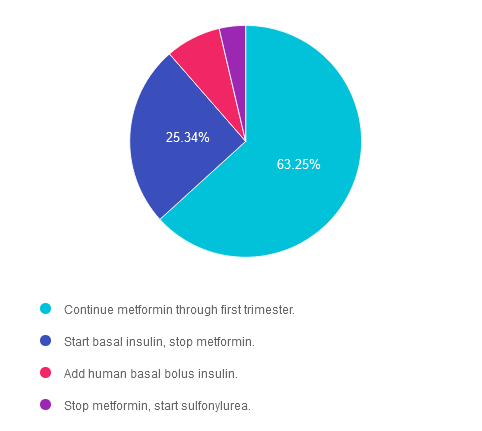
Answer 1 is correct. 63.25% chose this answer. “Continue metformin through first trimester.” YES, this is the best answer. According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Standard 15 goes on to say, “Insulin is the preferred medication for treating hyperglycemia in GDM. Metformin and glyburide, individually or in combination, should not be used as first-line agents, as both cross the placenta to the fetus. Other oral and noninsulin injectable glucose-lowering medications lack long-term safety data.” Given that KR has a fasting glucose in the prediabetes range, basal insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Answer 2 is incorrect. 25.34% of you chose this very tempting answer. “Start basal insulin, stop metformin.” However, according to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Given that KR has a fasting glucose in the prediabetes range, basal insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Answer 3 is incorrect. About 7.74% of respondents chose this. “Add human basal bolus insulin.” According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Given that KR has a fasting glucose in the prediabetes range, basal bolus insulin is not indicated at this time. KR needs referral to an RDN for nutrition therapy and ongoing evaluation of glucose levels.
Finally, Answer 4 is incorrect. 3.68% chose this answer. “Stop metformin, start sulfonylurea.” According to ADA Standard 15, “Metformin, when used to treat polycystic ovary syndrome and induce ovulation, should be discontinued by the end of the first trimester.” Standard 15 goes on to say, “Insulin is the preferred medication for treating hyperglycemia in GDM. Metformin and glyburide, individually or in combination, should not be used as first-line agents, as both cross the placenta to the fetus. Other oral and noninsulin injectable glucose-lowering medications lack long-term safety data.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join us live on June 11th at 11:30 am PST for our
Pregnancy & Diabetes
Level 2 Standards of Care Intensive
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, & understanding. This course reviews those special needs while focusing on Gestational Diabetes & Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, & prevention of complications during pregnancy. This is a helpful review for Certification Exams & those who want more information on people who are pregnant & live with diabetes.
Objectives:
- List three issues that affect pregnancy with diabetes.
- Describe the unique attributes of pre-existing diabetes in pregnancy & gestational diabetes.
- State the diagnostic criteria & management goals for gestational diabetes.
- Potential short-term & long-term complications of fetal exposure to hypoglycemia.
- Prevention measures to keep mother & baby healthy.
Learning Outcome:
Participants will gain knowledge of special considerations, individualized goals, and standards for people experiencing diabetes during pregnancy to improve outcomes.
Target Audience:
This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs/RDNs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions. The practice areas for RDs/RDNs for CDR reporting are healthcare, preventative care, wellness, and, lifestyle along with, education and research.
CDR Performance Indicators:
- 9.6.7
- 9.6.8
- 10.3.1
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working diabetes specialist and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
Recent Blog Bytes
- Rationale of the Week | Checkpoint Inhibitors Triggering Hyperglycemia
- Non-Invasive Glucose Monitoring: Update for Clinicians
- Question of the Week | Checkpoint Inhibitors Triggering Hyperglycemia
- Rationale of the Week | Indications for DXA Assessment of Bone Mineral Density
- Question of the Week | Common Cause of Missed Appts?
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.