

For our May 4th Question of the Week, 48% of respondents chose the best answer. We wanted to “take a closer look” into this question.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: MS is 63, has type 1 diabetes, and will be having knee surgery. In addition to using an insulin pump and CGM to manage their type 1 diabetes, MS also takes empagliflozin (Jardiance) 25 mg daily to improve glucose levels.
In preparation for the upcoming surgery, which of the following is an accurate statement?
Answer Choices:
- Transition to insulin injections in preparation for surgery.
- Maintain perioperative glucose between 80-110.
- Stop empagliflozin (Jardiance) 3 days prior to surgery.
- Reduce basal insulin by half the night before surgery.
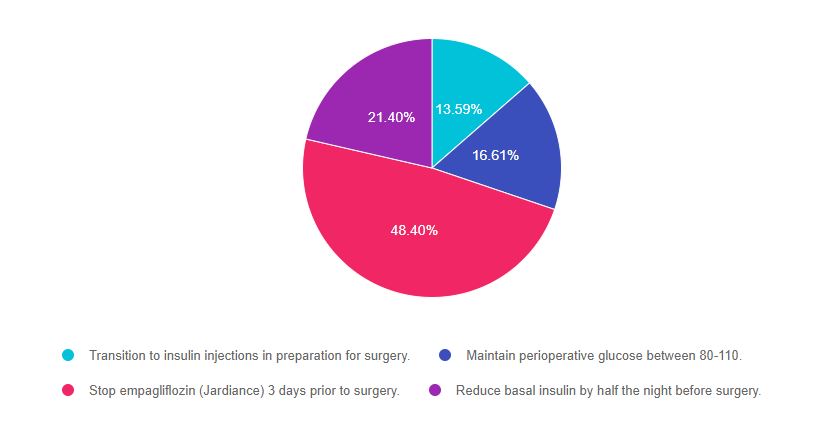
As shown above, the most common choice was option 3, the second most common answer was option 4, then option 2, and finally option 1.
Getting to the Best Answer
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to be familiar with type 1 and type 2 diabetes management in a variety of settings and situations.
Answers & Rationale
Answer 1 is incorrect, 13.59% chose this answer, “Transition to insulin injections in preparation for surgery.” Having glucose levels on target can help to improve surgical outcomes. For MS, staying on the insulin pump pre and post post-operatively will ensure best glucose management and allow MS to participate in care.
Answer 2 is incorrect, 16.61% of you chose this answer, “Maintain perioperative glucose between 80-110.” According to the ADA Standards, the perioperative glucose target is 80- 180. The goal of 80-110 is too narrow of a range and increases risk of intraoperative hypoglycemia.
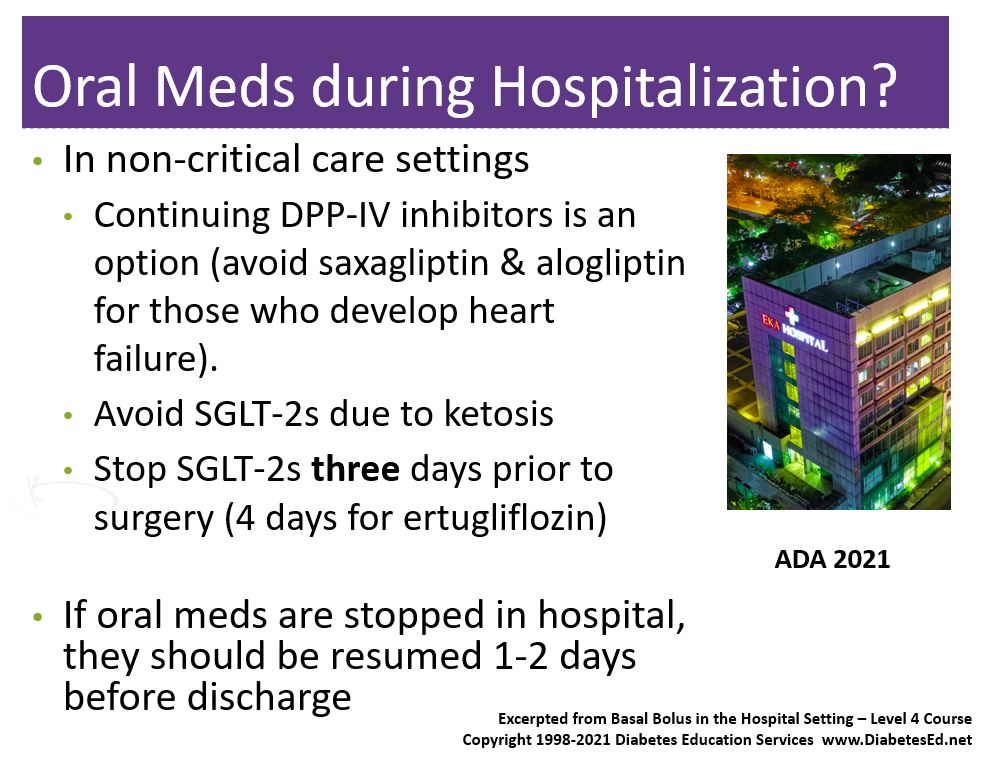
Answer 3 is correct, 48.40% of you chose this answer, “Stop empagliflozin (Jardiance) 3 days prior to surgery.” The new ADA 2021 Standards recommend stopping all SGLT-2s three days prior to surgery and ertugliflozin four days prior to surgery. In addition, SGLT-2s should be stopped with hospital admission. The reason behind this recommendation is to prevent DKA or ketoacidosis during hospitalization. (See slide below from our Basal Bolus in the Hospital Setting Level 4 Class).
Download Free Med PocketCards
Answer 4 is incorrect, 21.40% of you chose this answer, “Reduce basal insulin by half the night before surgery.” For someone with type 1 diabetes, if the basal rate is set correctly there is no basal dose reduction needed, even if someone is NPO. Reducing basal by 50% could actually put them at risk for hyperglycemia pre-operatively. If MS is at risk of hypoglycemia, we might consider making a 5-10% basal rate reduction, but not 50%.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
See ADA Standard 15 – Diabetes Care in the Hospital Setting
Want to learn more about this question and more?
Enroll on our
Basal/Bolus Therapy in Hospital Webinar 1.5 CEs
Recorded and Ready for viewing

Glucose control in the hospital matters! This course provides participants with a step-by-step approach to safely and effectively implement Basal Bolus Insulin Therapy in the inpatient setting. We discuss appropriate insulin dosing based on the individual’s clinical presentation and apply dosing strategies to a variety of case studies. Included are hard-to-manage situations that commonly occur in hospital settings and a discussion of solutions that will keep people safe and get glucose levels to goal. In addition, sample basal/bolus and insulin drip guidelines plus lots of resource articles are included.
Topics Include:
- Discussing appropriate insulin dosing based on the individual’s clinical presentation
- Applying dosing strategies to a variety of case studies
- Introduce hard-to-manage situations that commonly occur in hospital settings
- A discussion of solutions that will keep individuals safe and get glucose levels to goal
- Sample basal/bolus and insulin drip guidelines plus lots of resource articles are included
Join us for our Live Webinars
Including Brand New Specialty Courses!
Can’t join live? No worries, we will record the webinar and post it to the Online University!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.