Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
On Fridays, I get to provide diabetes care at a local clinic where about half of the people I see are Spanish-speaking only. We do have wonderful interpreters, but I have a strong desire to communicate directly with my clients and really understand what they are saying, in their language.
My Spanish is getting better, but I keep giving myself permission to appreciate where I am now, with the belief that even at my age, I can keep improving.

I took a few years of high school Spanish, but never really had a grasp on the language until I signed up to move to a small pueblo in Mexico, in 1987, to volunteer as a rural healthcare worker.
I lived with a local family and helped with daily chores in addition to providing services in the clinic. As part of the “Projecto Projimo”, I helped with everything from cleaning bathrooms to dressing wounds as pictured here. I also attended classes daily in Spanish, to become a “Promotora de Salud”, a community health worker.
Along with learning Spanish, I have gained some other valuable insights that I would like to share.
For the first few months I lived in Mexico, my Spanish was so bad I was reluctant to talk and embarrass myself.
Instead I did a lot of careful listening and observing.
As with anyone acquiring a new language, my brain was looking for patterns and listening for frequently used words. I studied cognates and learned about sentence structure and common phrases in my textbook, “Donde No Hay Doctor – Where There is No Doctor”, which I would read every night before passing out from mental exhaustion.
By the third month of living within this new community, I was able to understand most of the questions being asked and respond with rudimentary sentences. Sometimes I could even conjugate in the past tense. That was 30 years ago.
Now, working in the clinic, I have had to dust off my Spanish language skills, that have been languishing in the recesses of my brain for almost three decades. I have committed myself to expanding my Spanish vocabulary and improving my ability to communicate in ways that are meaningful.
When I meet with our Spanish-speaking clients in my current clinic, to fully understand what they are saying, I have to dedicate my whole being to hearing their diabetes stories.
It all starts with listening.
I am completely present to capture all the words they are saying coupled with their body gestures. Sometimes I get so enraptured in everything they are saying, then when they stop, I forget to ask the next question.
In that silence, we have a moment of understanding and togetherness that goes beyond language.
The funny thing is, in spite of knowing lots of diabetes phrases in Spanish and the names of dozens of fruits and vegetables, plus most of the body parts and medical conditions, there is still one phrase that I need to say with each new person I meet.
When people share their diabetes stories with me, it feels like there is an invisible burden they are carrying on their backs. This burden is reflected in tears or embarrassment for elevated blood sugars. For many, that burden is best described as shame.
They somehow believe it is their fault they have diabetes.
I reassure them, that diabetes is not their fault. It is a complex interplay between genetics, environment, access to healthy foods, stress, inequities, body weight, and age.
Each one of us knows people who don’t eat healthfully, have extra weight and don’t exercise, who never get diabetes.
Let’s help people let go of the shame so they can move toward engaging in self-care that improves their sense of self and well-being.
Let’s remind them that they are worth it!
The outstanding thing I so appreciate is the grace that my Spanish-speaking clients show me.
So many times I can’t remember a vocabulary word, or I will say a phrase in a funny way. There are moments where I stumble and feel bad that I don’t have the ability to accurately express what I am thinking.
No one has ever made me feel bad about my mistakes. They are respectful and just politely ask, “Mande?”, letting me know that they did not understand what I was trying to communicate.
They are simply grateful that I am trying to communicate in their language.
It reminds me to be patient with people who are trying to acquire the English language. Let’s acknowledge the courage it takes to tackle a language that you did not grow up speaking. Let’s offer them grace and the opportunity to practice speaking this new language.
We can also let them know they are safe to make mistakes with us.
Gracias! Coach Beverly
| Please enjoy these FREE resources that we have put together for you: |
|---|

See Full Free Resource Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Unsure about updates for the 2020 exam?
Coach Beverly offers this FREE webinar to help get you to prepare for the CDCES Exam. All her tips and tricks are meant to ease your mind and reflect the updates to the CDCES content outline.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 6 times. She is a nationally recognized diabetes expert for over 25 years.
See our Preparing for CDCES Resource Page >>
Test Taking Toolkit (220+ practice questions)
Whether you are preparing for the updated CDCES or BC-ADM exam, this test-taking toolkit is designed to prepare you for success.
This toolkit includes two courses with over 220 practice questions to help you prepare and simulate the exam.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
As we enter fire and storm season, it’s always a good idea to think ahead and be prepared for disaster. In addition to the items listed below, make sure to pack hand sanitizer, wipes, and masks due to the current pandemic. Also, bring your own pillow and bedding in case you need to spend time in a shelter.
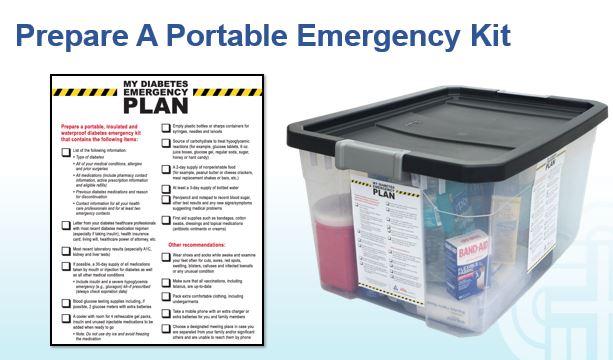
For any emergency scenario, it’s important to have an emergency preparedness plan. For people living with diabetes, a “diabetes kit” is an important part of emergency preparedness. Diabetes Disaster Response Coalition (DDRC) has put together great resources to help people with diabetes be prepared so that no one is caught unaware without medication.
DDRC’s Diabetes Kit checklist includes needed supplies, but more importantly, information that should be written down and kept in a waterproof container for emergency situations where a health care provider could find it and make informed emergency treatment decisions.
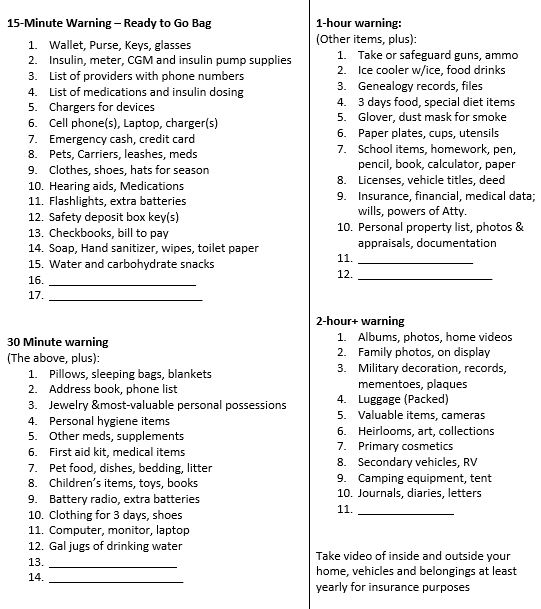
Emergency Evacuation-Items to Gather for People with Diabetes
We thought this list was a helpful way to prioritize what items to grab given different time frame limitations. We found it online, and customized it for people with diabetes. It is available in Word or PDF. Thank you for sharing with your colleagues and community.
1-800-DIABETES (800-342-2383) is an excellent referral resource for people with diabetes to call toll free for updates on accessing medical support during an emergency.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
On my 40th birthday, I was gifted a Mission Fig tree that was no taller than my 5″ 7″ self.
The tree loved her new home and grew quickly, spreading out her limbs and gifting us with buckets of sweet fig fruit within a few years.
She is a strong and sturdy tree. My teenagers do pull-ups on her limbs and she has survived all kinds of weather events.
She rebounded after an intense wind storm, where her largest limb snapped off. Overburdened with figs, her trunk broke in half one season. We worried she wouldn’t make it, but that summer she produced even more figs.
When we were planning to build my office eight years ago, the architects told us our fig tree would need to be cut down to make room.
We altered our building plan and moved the location of my office to make room our beloved fig tree.
As a gesture of gratitude, our tree has blessed us with fig “over-abundance” year after year.
With my office doors open in the summer, I hear the birds fighting for the juiciest figs that thrive on her crown. During work breaks, we go outside, stand in her shade and search for the plumpest and biggest figs to eat on the spot and later to bake and top with a dab of goat cheese.
To extend our fig enjoyment through winter and beyond, we collected over 7 lbs of figs and made 9 jars of buttery fig jam.
With virtual coaching from my Aunt Hedy in Canada, I cut up 7 pounds of figs, added some sugar, fresh lemon juice and a generous cup of brandy. I cooked on low for at least four hours to blend flavors and reduce the jam to the perfect thickness. The brandy adds a smokey, caramel flavor to the jam, that my family loves. However, it also tastes great without it.
Here is the recipe for fig jam that I modified by cutting the sugar by one – half and then adding it back as needed for thickening.
Drunken Fig Jam (Coach Beverly’s modified recipe)
You can easily google a recipe with more detailed instructions, but here is the basic idea.
Put all of the above into a thick pot and mix. Let sit for an hour, stirring occasionally. Then put on a low heat and let simmer for 4-6 hours to reduce to desired thickness. You may need to add a little more sugar for thickening and lemon juice for the right balance of sweet and “lemonyness”.
Then put into sterilized jars and follow usual canning procedures. I always save one jar as a refrigerator jam that we can start enjoying right away.
With all that is going on in the world, I wanted to write a post that is life affirming and voices my gratefulness for the generosity of nature and my fig tree in particular.
Coach Beverly
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our August 4th Question quizzed test takers on CV Disease risk management and diabetes. Although 49% of respondents chose the correct answer, 51% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: RJ is 67 years old with a 40+ year history of type 1 diabetes. GFR is 62, UACR is < 30, A1c is 6.7%, B/P is 132/72, LDL cholesterol is 98, RJs BMI is 28.6. RJ uses multiple daily injections and CGM to manage RJs diabetes.
RJ’s other medications include: Levothyroxine 100mcg daily, atorvastatin 40mg daily, Aspirin 81 mg daily and a multivitamin.
Based on your assessment, which of the following interventions would improve RJs outcome?
Answer Choices:
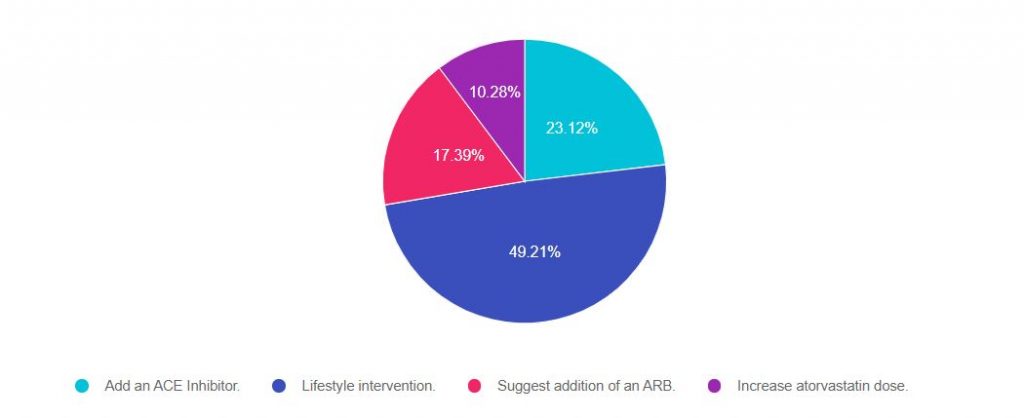
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers will ask about the guidelines for specific ADA Standards of Care. This question is pulled from section 10 of the Standards on CV Disease and Risk Management. To purchase your own ADA Standards, visit our store.
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
Answer 1 is incorrect. 23% chose this answer. “Add an ACE Inhibitor.”
Many people chose this juicy answer. It is true that in the past, people with type 1 would be automatically started on an ACE Inhibitor because it was thought starting an ACE would offer renal protection. However, based on extensive research, the American Diabetes Association stopped recommending adding an ACE for people with type 1 without the diagnosis of hypertension a few years back.
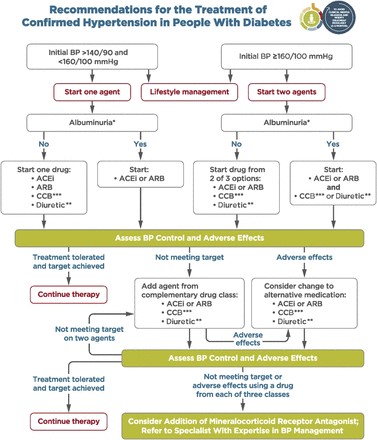
The current blood pressure goal for people with diabetes is 140/90.
If a person with type 1 diabetes has hypertension, defined as either systolic greater than 140 or diastolic more than 80, repeated on 2 different occasions, initiate blood pressure therapy.
Lower blood pressure goal of 130/80? It is recommended to do a cardiovascular risk assessment using the CV Risk Calculator on all people with diabetes. If the 10 year risk of having a CV event is greater than 15%, the blood pressure goal is 130/80 may be appropriate, if it can be safely attained. The choice of blood pressure therapy is further refined by presence or absence of microalbuminuria.
We don’t have enough information to calculate his CV Risk, so based on the information we have, adding an ACE Inhibitor is not indicated at this time. And of course, since we only have one blood pressure, we need to collect more data before taking action.
Answer 2 is correct. 49% of you chose this answer. “Lifestyle intervention.”
This is the best answer. Looking at this profile, we can see that RJ’s BMI is above 25 and LDL is slightly elevated. Let’s refer RJ to a Registered Dietitian. By coaching RJ on healthy food choices, increased whole foods and fiber, and taking a look at animal protein consumption, there is an opportunity to improve not only RJs blood pressure but also RJs LDL cholesterol. In addition, we can evaluate RJs activity level and encourage 150 mins a week of activity plus strengthening that would contribute to his overall health.
Answer 3 is incorrect. About 17% of you chose this answer. “Suggest addition of an ARB.” See rationale under answer 1.
Finally, Answer 4 is incorrect. 10% of you chose this answer. “Increase atorvastatin dose.” Currently, RJ is on high intensity statin therapy with RJs atorvastatin dose of 40mg. He does not present with any concerning CV risk factors or events that would kick RJ into high risk category. We could calculate RJs 10 year risk of CV disease and if it is more than 20% or if RJ doesn’t response to lifestyle changes, we could consider a further increase in the statin dosing. Based on the info we have at this moment, this is not the BEST answer (but it is a consideration : -).
Download our FREE Lipid and Hypertension Cheat Sheets – great resource and invaluable test study tool too!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Click here to test your knowledge!

Join us Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
Many of you are curious about the steps involved in becoming a BC-ADM. Thank you for reaching out to us with your questions about eligibility and study strategies. Coach Beverly will be providing answers to your questions interwoven with her own journey to achieve her Board Certification in Advanced Diabetes Management (BC-ADM).
Becoming Board Certified in Advanced Diabetes Management (BC-ADM) is an excellent professional goal for diabetes specialists with an advanced degree in their field and a professional license as an advanced practice nurse, registered dietitian, or registered pharmacist or provider.
The person holding the BC-ADM credential skillfully manages complex patient needs and assists patients with their therapeutic problem-solving. Within their scope of practice, healthcare professionals who hold the BC-ADM certification:
The scope of advanced diabetes practice includes clinical management skills such as medication adjustment, medical nutrition therapy, exercise planning, counseling for behavior management, and psycho-social issues. There is a focus on research, national standards, medical management of diabetes, and co-conditions, with a person-centered care approach.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Join us Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
Many of you are curious about the steps involved in becoming a BC-ADM. Thank you for reaching out to us with your questions about eligibility and study strategies. Coach Beverly will be providing answers to your questions interwoven with her own journey to achieve her Board Certification in Advanced Diabetes Management (BC-ADM).
Becoming Board Certified in Advanced Diabetes Management (BC-ADM) is an excellent professional goal for diabetes specialists with an advanced degree in their field and a professional license as an advanced practice nurse, registered dietitian, or registered pharmacist or provider.
The person holding the BC-ADM credential skillfully manages complex patient needs and assists patients with their therapeutic problem-solving. Within their scope of practice, healthcare professionals who hold the BC-ADM certification:
The scope of advanced diabetes practice includes clinical management skills such as medication adjustment, medical nutrition therapy, exercise planning, counseling for behavior management, and psycho-social issues. There is a focus on research, national standards, medical management of diabetes, and co-conditions, with a person-centered care approach.

This free webinar will review BC-ADM requirements for the current year.
Coach Beverly will discuss:
She will also review sample test questions and reasoning behind choosing the right answers. We hope you can join us.
Aug 20, 2020 @ 11:30 – 12:40 p.m. PST
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
**To satisfy the requirement for renewal of certification by continuing education for the Certification Board for Diabetes Care & Education (CBDCE), continuing education activities must be applicable to diabetes and approved by a provider on the CBDCE List of Recognized Providers (www.ncbde.org). CBDCE does not approve of continuing education. Diabetes Education Services is accredited/approved by the Commission of Dietetic Registration which is on the list of CBDCE Recognized Providers.”
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]We are off to College!

Good morning everyone, Beverly won’t be at work today. She will be taking the next step in moving her son toward independence.
In 2002, Beverly brought her firstborn into the world.
Now she is bringing him to college.
After surviving the first 18 years of motherhood (barely), Coach Beverly is ready to kick (gently) her oldest little fledgling, Robert, out of her nest and into the much bigger nest of the collegiate world.
Robert shows all the signs of readiness to leave his home of origin behind and move to the dorms to start college at SMU (Go Mustangs) in Texas.
Robert’s signs of readiness to move out and move on include:
These are all signs that we have succeeded at our job as parents. Now with a mixture of joy and a twinge of longing, I will deliver him to the next stage of his journey.
Our prayers are with him. We will keep you posted!