
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
MS has type 1 diabetes and is on a low carb diet to help her keep her weight on target. She has a BMI of 24.3. MS has a friend with type 1 who is taking a SGLT-2 in addition to insulin to help with weight management. MS wants to know if she could add on a SGLT-2 to her insulin treatment plan.
What is the Diabetes Specialist’s best response?
Click here to test your knowledge!

Our May 19th Question of the week was a question about carb counting. Although 58% of respondents chose the correct answer, 42% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LS uses an insulin pump and the 500 rule for carbohydrate coverage. For breakfast, LS plans to eat ½ cup of oatmeal, 3/4 cup of blueberries, a cup of skim milk, a tablespoon of peanut butter, and a cup of coffee with a packet of Splenda. Her insulin to carb ratio is 1 to 12 for breakfast and lunch. Her insulin to carb ratio is 1 to 15 for dinner.
How much insulin does LS need for breakfast?
Answer Choices:
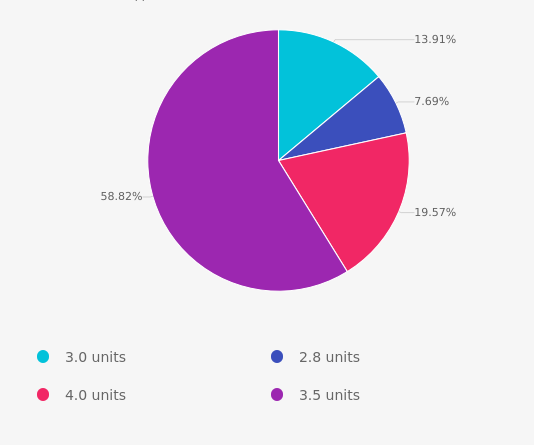
As shown above, the most common choice was option 4, the second most common answer was option 3 then option 1 and finally option 2.

Answer 1 is incorrect. 14% chose 3.0 units as the answer. This answer was juicy but wrong. Maybe this group thought the total carb count was 45 gms and then divided by insulin to carb ratio of 1:15? If yes, read the question again to see what insulin to carb ratio is a better choice. Also, rethink the total carb count.
Answer 2 is incorrect. Only 8% of respondents chose 2.8 units as an answer. This group got the carb count correct but may want to read the question again to see which insulin to carb ratio is a better choice.
Answer 3 is also incorrect. About 20% of respondents chose 4.0 units. This group might need to reassess the carb count, keeping in mind that milk is 12gms of carb. And, more importantly, keep in mind that LS uses an insulin pump that can deliver very precise insulin doses. No need to round up for this question.
Finally, Answer 4 is correct. 58% of test takers chose this correct answer.
First, lets count up the carbs for breakfast:
Now, let’s do the math:
LS’s insulin to carb ratio is 1 to 12 for breakfast. She is going to eat 42 gms of carb. 42/12 = 3.5 units of insulin to cover breakfast.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
This course is an essential review for anyone in the field of diabetes. This course summarizes the 2021 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for health care professionals involved in diabetes care and education.
Earn 2.0 CEs and get ready to lead the charge to implement best care practices for the New Year.
Topics Include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
What we say matters.
As educators, advocates, spouses, friends, and providers, our use of language can deeply affect the self-view of people living with diabetes every day.
Intentional communication is a powerful tool that can uncover trauma, identify barriers, and move both the provider and person with diabetes toward a greater understanding of the issues involved.
The language used in the health care setting is immensely important in determining trust, mutual respect, and meaningful long term relationships.
Watch 2020 Lifting People Up with Language 33 minute Webinar Now
Language and Diabetes Powerpoint Handout
FREE Diabetes & Language | Quiz
Topics covered include:
This mini-webinar is free, and no CEs are provided, but there is lots of great info!
Articles and Resources
Use of Language in Diabetes Care and Education – 2017 ADA & AADE
Language is powerful and can have a strong impact on perceptions as well as behavior. This article provides recommendations for the language used by health care professionals and others when discussing diabetes through spoken or written words whether directed to people with diabetes, colleagues, or the general public, as well as research questions related to language and diabetes.
Quick Guide on Diabetes and Language for Health Care Professionals – AADE
Empowerment vs. Compliance Model
Action for Happiness – Excellent website filled with actions we can all take to feel better every day.
Adverse Childhood Experiences (ACE) Resources
ACE Screening Tool and Resilience Inventory
Becoming ACE-Aware Training Program
Nadine Burke Harris, MD TED Talk on How Childhood Trauma affects health
NPR Article – Take the ACE Score and Learn what it does and doesn’t mean
Trauma-Informed Care Fact Sheet

College-aged men who play video games consumed less healthy foods than their non-gaming peers, according to data presented at Nutrition 2020 Live Online.
“Video game usage has been studied extensively in children and adolescence, less in adults, and to our knowledge not at all in college students. Because college students are presented with a unique experience compared to other adults and children, it is important to understand how video game users in this specific population behave,” stated Dustin G. Moore, a graduate student at the University of New Hampshire, told Healio Primary care.
Male college students who were moderate or heavy video game players ate more saturated fat than those who did not play video games. While those who were moderate gamers consumed more salt than those who did not play video games, according to the data presented at Nutrition 2020 Live Online.
Heavy video game playing was also associated with consuming more discretionary calories when compared with those who don’t play. Men who were moderate and heavy video game users consumed fewer fruits and vegetables.
There appeared to be no significant differences in alcohol consumption, sugar, total dietary fat, and waist circumferences.
“This is a concerning finding because previous research has shown that lifestyle habits in early adulthood tend to continue later in life,” Jesse S. Morrell, PhD, principal lecturer for the nutrition program at the University of New Hampshire, said in an interview. “If these poor lifestyle habits continue, this population will be at higher risk for [above target weight] and chronic disease.”
It would be interesting to track video game time vs outdoor physical activity time in this same group, and comparing eating habits.
As diabetes specialist invested in the health of future generations, it is important to encourage physical activity and healthy eating in all age groups, but especially in the college-age group.
College is often the first time teens are living away from home, and making independent choices on food and meals.
To read more, click here.
Written by Catherine Cullinane RN, CDCES, our resident Tech Thursday Content Writer
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
If we consider why certain groups are at increased risk for diabetes, heart attack, stroke, cancers and other health issues, we can look back in time to their childhood for answers.
Children who experience more Adverse Childhood Experiences, also referred to as ACEs, are more likely to suffer with chronic health issues as adults.

Research has show that adverse childhood experiences (ACE) do not affect all children equally.
In the United States, those from marginalized identities are much more likely to have experienced early childhood trauma, which can have lasting effects on one’s health.
The more adverse experiences that happen before the age of 18, the more likely adults are likely to express a wide array of chronic health problems including: diabetes, overweight, cancers, hypertension, stroke, heart attack, mental health issues, substance use, and more.
Due to the complex intersections identity, socioeconomic status, and healthcare access, marginalized individuals are much more impacted by ACE.
This puts certain individuals at higher risk of future chronic conditions in adulthood, like diabetes. These inequities are a by-product of social determinants of health and the impact on individuals and communities. As diabetes advocates, we are compelled to reflect on these intersections to improve health outcomes.
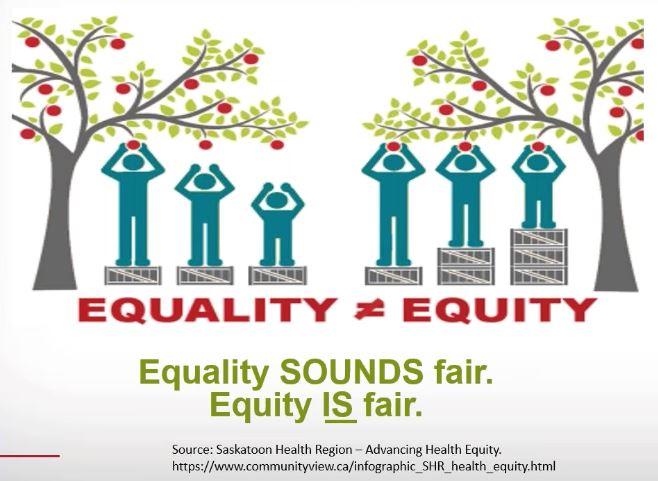
The World Health Organization describes the social determinants of health as “the conditions in which people are born, grow, live, work, and age. These circumstances are shaped by the distribution of money, power, and resources.”
This unfair distribution of access and services results in the unfair but avoidable differences in health status seen between different neighborhoods, zip codes, and even states.
Achieving equity will take time and is complicated by a long history of institutionalized racism, sexism, and other prejudices. We need to make legislative adjustments that compel corporations, educational systems, health care agencies, and local governments to assure equitable access to services to those who have been historically excluded.
Start with our children. If societies are structured to help children feel safe and protected, they will enter adulthood healthier and more prepared to perpetuate health for future generations. I highly recommend all those involved in diabetes education listen to this groundbreaking video which explores the science between childhood trauma and health: Nadine Burke Harris, MD TED Talk on How Childhood Trauma affects health.
ACE-Aware Training Program: The other obvious place to direct our energy is with our adult clients who are living with prediabetes or diabetes. We know that many of them may be having difficulty making behavior changes and engaging with their health care due to adversity experienced in childhood. Let’s set up or health care facilities to provide Trauma-Informed Care. If you would like to learn more about this topic, I encourage you to get started in this free training worth 2.0 CEs. Becoming ACE-Aware Training Program. I completed this program a few months ago and found it compelling and instructive.
A Practitioner’s Guide to Advancing Health Equity CDC PDF
Thank you for reading this post and we invite you to send us comments or additional resources to [email protected]. We read each email and appreciate your contributions.
COVID-19 & Diabetes: Examining the impact of health disparities in a time of crisis(link is external) – This live event, posted on the ADA website, was recorded Thursday, April 23. It provides an excellent exploration of health equality vs. health equity with honest and insightful discussions by a panel of experts. As the nation grapples with the COVID 19 health crisis, communities already experiencing social, economic, and health disparities face even more severe challenges combatting this disease. Join us for an information-packed webinar exploring the nexus of COVID-19, diabetes, and health equity.
Daniel E. Dawes, JD, Author, The Political Determinants of Health, and Director, Satcher Health Leadership Institute at Morehouse School of Medicine.
Adverse Childhood Experiences (ACE) Resources
Nadine Burke Harris, MD TED Talk on How Childhood Trauma affects health
Becoming ACE-Aware Training Program
ACE Screening Tool and Resilience Inventory
Posted on www.AcesAware.org A Health Problem and An Opportunity: Screening for Adverse Childhood Experiences
Dr. Dayna Long, Director for the Center for Child and Community Health at UCSF Benioff Children’s Hospital Oakland, discusses the pervasiveness of Adverse Childhood Experiences (ACEs) and why screening for ACEs is critical to providing trauma-informed care.
NPR Article – Take the ACE Score and Learn what it does and doesn’t mean
Trauma-Informed Care Fact Sheet
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LS takes 20 units 70/30 insulin twice daily with an insulin pen. LS states that blood sugars are usually on target, but over the past week, blood sugars have suddenly increased. LS confirms that they are taking insulin on a regular basis.
Which factor could be contributing to this sudden blood glucose rise?
Click here to test your knowledge!
Want more practice questions?
Try our Test Taking Toolkit!
$49 | 220+ Questions
In this course, Coach Beverly details the content of the exam and test-taking tips. Plus, she reviews a sampling of the questions, and explains how to dissect the question, eliminate the wrong answers and avoid getting lured in by juicy answers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We are excited to invite you to our upcoming webinar series. Coach Beverly is offering FREE access to our Level 2 | Standards of Care Intensive Series Live Stream Webinars.
This intensive series is designed to engage students in deciphering and exploring the ADA Standards of Care from top to bottom.

Our first course of the Level 2 Series, Microvascular Complications – Preventing Eye Kidney and Nerve Disease, is recorded and ready for viewing. You can watch for FREE or purchase to earn CEs. See information below.
Join Options to view Live Stream Level 2 Webinars
DiabetesEd Services Online University Courses are an excellent way to study for your exam anytime and anywhere that is convenient. You have immediate access to your courses for 1 year after your purchase date.
This 90-minute course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines.
Topics include:
Click here for FREE recorded webinar (no CEs).
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Some brands of long acting Metformin are being recalled since they contain higher than acceptable levels of NDMA (see list below).
The U.S. Food and Drug Administration has recommended recalls of certain metformin products that may contain the impurity N-nitrosodimethylamine (NDMA) above the acceptable intake limit.
Patients taking recalled metformin should continue taking it until a doctor or pharmacist gives them a replacement or a different treatment option. It could be dangerous for patients with type 2 diabetes to stop taking their metformin without first talking to their health care professional.
Remind patients not to stop medication until they check with their provider.
Find more info on the FDA Website here
For a complete listing of diabetes medications and insulin, download our DiabetesEd Medication PocketCards