
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Being a diabetes educator can be challenging. This one-hour presentation by Heather Nielsen, MA, LPC, CHWC will provide diabetes educators with helpful hands-on strategies to incorporate mindfulness and self-compassion into our daily lives and professional practice. As a counselor and a certified wellness coach, Heather has an abundance of wellness wisdom to share with educators who provide lifesaving diabetes education and support to people living with diabetes.
Topics include:
This webinar is free and you can view it at any time, on any device.

Guest speaker: Heather Nielsen, MA, LPC, CHWC – Follow her on her Healthy Connections FaceBook Page
Since 2001, Heather has worked in both medical and behavioral health fields. She is currently a Licensed Professional Counselor and Certified Health and Wellness Coach at Heather Nielsen Counseling and Coaching. Her personal mission is to help people with diabetes find balance, peace, and well-being.“We all need help in managing chronic illness, and I specialize in helping people live well, despite diabetes. With practice and presence, we can learn to transform our brains and our minds, thus finding healthier ways to relate to our disease and to life. I offer a very individualized approach for each client.”
Heather’s passion for mindfulness and diabetes came from her own struggles of living imperfectly with Type 1 since 1997. She is the mother of three teenage daughters, and credits her own practice in mindfulness and self-compassion as a key factor in her good health and happiness in this phase of parenting! She and her husband, an internist, just opened a Functional Medicine clinic in Hood River, Oregon, where they provide team care to people with chronic illnesses of all kinds. Of course, people with diabetes are her favorites.
See more Mindfulness Resources here >>
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
**To satisfy the requirement for renewal of certification by continuing education for the Certification Board for Diabetes Care & Education (CBDCE), continuing education activities must be applicable to diabetes and approved by a provider on the CBDCE List of Recognized Providers (www.ncbde.org). CBDCE does not approve continuing education. Diabetes Education Services is accredited/approved by the Commission of Dietetic Registration which is on the list of CBDCE Recognized Providers.
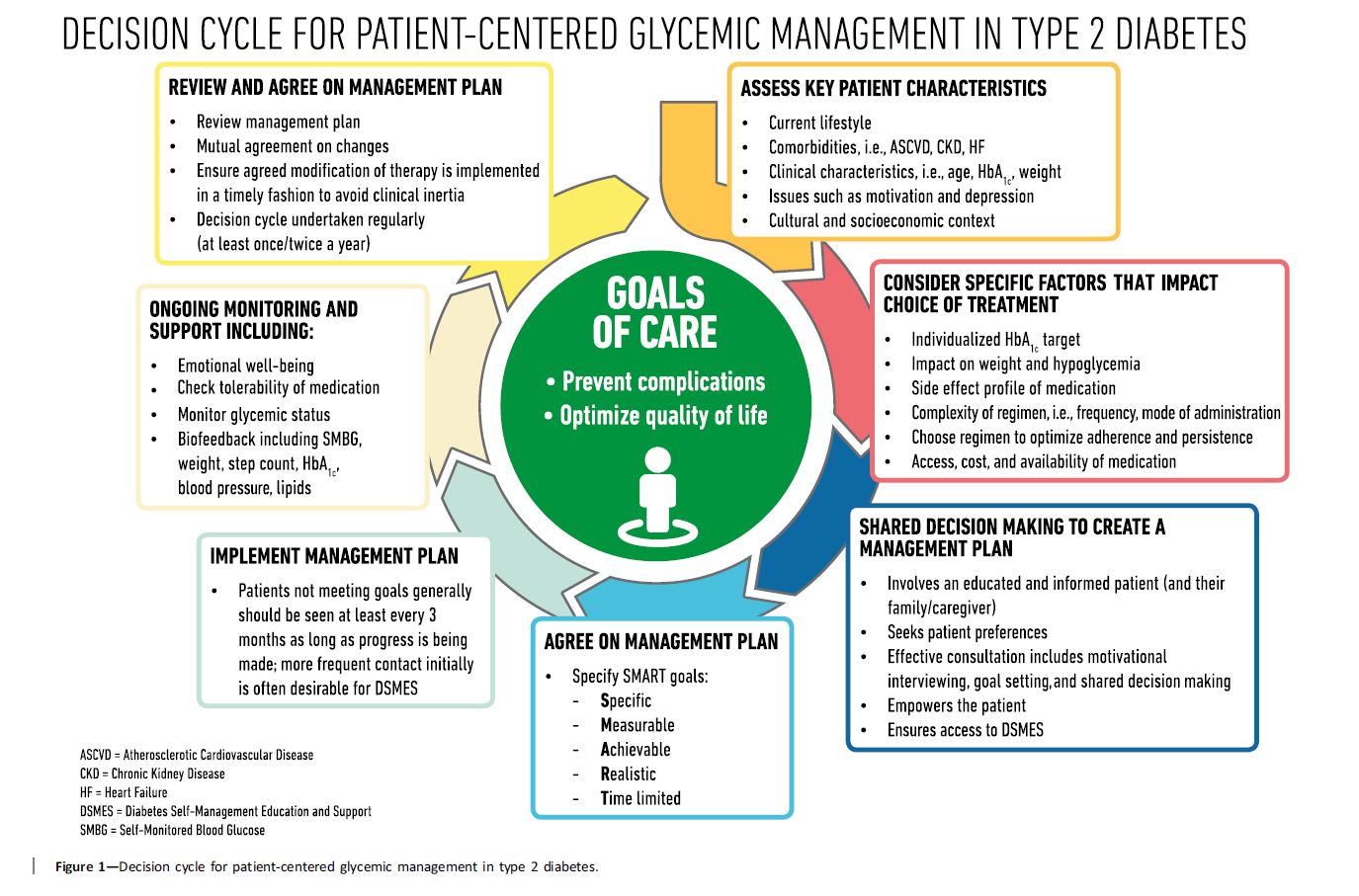
Management of Hyperglycemia in Type 2 Diabetes, 2018. https://doi.org/10.2337/dci18-0033
A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD).
This new consensus statement is a summary of findings based on a comprehensive literature search of peer reviewed articles published from 2014 to February 2018.
Here are some key statements from the Principles of Care Section that really stood out. In addition, the Decision Cycle Chart below, is an excellent summary of person centered considerations to determine the best path to take when deciding upon lifestyle and medication therapy.
Key concepts that I found intriguing and helpful from this section:
Therapeutic inertia, also called clinical inertia, refers to the lack of action even when blood glucose targets are above target. This is something I have frequently seen in my diabetes practice. A common example of this is a PWD on two to three different diabetes medication and basal insulin, with an A1c is greater than 9%, yet no changes in therapy are made for months or years. The causes of this inertia may complex, but can be a result of the provider, person with diabetes or the health care system.
To avoid or stop Clinical inertia, here are recommended strategies:
 Remission of type 2 diabetes: Mission Not Impossible.
Remission of type 2 diabetes: Mission Not Impossible.In the Management of Hyperglycemia in Type 2 Diabetes, 2018.A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), on page 12 and 18, they reference the results of the DiRECT study below. They recommend that all overweight and obese PWD be advised of the health benefits of weight loss and encouraged to engage in an intensive lifestyle program to achieve weight loss reduction.
The DiRECT study, published in the Lancet in February 2018, aimed to assess whether intensive weight management within routine primary care would achieve remission of type 2 diabetes.
Goals of the study were weight loss of 15 kg or more and remission of diabetes, defined as A1c less than 6·5%, after at least 2 months off all antidiabetic medications, from baseline to 12 months.
To evaluate if this was possible, the research team initiated an open-label, cluster-randomised trial (DiRECT) at 49 primary care practices in Scotland and the Tyneside region of England. They recruited individuals aged 20-65 years who had been diagnosed with type 2 diabetes within the past 6 years, had a body-mass index of 27-45 kg/m2, and were not receiving insulin.
All diabetes and hypertension medications were stopped and very low calorie diet was started.
For 12 months, two groups consisting each of 149 participants were followed. The intervention group received weight management support and the control group received no weight loss intervention.
At end of study (12 months), diabetes remission was achieved in 68 (46%) participants in the intervention group and six (4%) participants in the control group
Diabetes remission rates associated with weight status at 12 months:
Other interesting observations:
Nine serious adverse events were reported by seven (4%) of 157 participants in the intervention group and two were reported by two (1%) participants in the control group. Two serious adverse events (biliary colic and abdominal pain), occurring in the same participant, were deemed potentially related to the intervention. No serious adverse events led to withdrawal from the study.
The results show that, at 12 months, almost half of participants in intervention group achieved, with a mean weight loss of 10%, experienced remission to a non-diabetes state without diabetes medications.
The authors conclude that remission of type 2 diabetes through a structured weight loss intervention is a practical target for primary care
Want to read more?
Lancet. 2018 Feb 10;391(10120):541-551. doi: 10.1016/S0140-6736(17)33102-1. Epub 2017 Dec 5.
 Increased knowledge of how gut bacteria ratios change as a marker of inflammation could help delay the development of Type 1 Diabetes. Researchers from the University of Queensland proposed that monitoring the microorganisms living in the gut may aid in understanding the disease better as a whole.
Increased knowledge of how gut bacteria ratios change as a marker of inflammation could help delay the development of Type 1 Diabetes. Researchers from the University of Queensland proposed that monitoring the microorganisms living in the gut may aid in understanding the disease better as a whole.
Participants in the study were all newly diagnosed with Type 1 Diabetes and were asked to provide a stool sample. The researchers analyzed these samples and found that, “certain proteins can be used to differentiate risk levels.”
UQ Diamantina Institute Senior Research Fellow Dr Emma Hamilton-Williams said: “By studying the stool samples of participants, we found that changes in gut bacteria weren’t just a side effect of the disease, but are likely related to disease progression.”
Research on the topic is new and fairly undeveloped. However, there are plans to carry out further research on the bacteria associated proteins, analyzing why they may signify an increased risk of Type 1 Diabetes expression.
The researchers are hoping to use this microbial information to monitor disease progression or develop therapies aimed at restoring a healthy microbiota in people at risk of type 1 diabetes.
For more information, Join our FREE Getting to the Gut, Meet Your Microbiome –
Live Webinar November 14th, 2018 at 11:30am PST
Read original article in Diabetes Care – Intestinal Metaproteomics Reveals Host-Microbiota Interactions in Subjects at Risk for Type 1 Diabetes –
And visit Monitoring gut changes could help delay type 1 diabetes.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
 As diabetes educators, having eye contact and listening carefully without distraction, is a critical part of our assessment. This initial meeting helps us sort out what is working with the person’s diabetes and what barriers might be getting in the way. The words we use, our body language, and how we engage in this encounter sets the stage for our ongoing working relationship. Plus, it can influence the self-perception of the person sitting across from us.
As diabetes educators, having eye contact and listening carefully without distraction, is a critical part of our assessment. This initial meeting helps us sort out what is working with the person’s diabetes and what barriers might be getting in the way. The words we use, our body language, and how we engage in this encounter sets the stage for our ongoing working relationship. Plus, it can influence the self-perception of the person sitting across from us.
However, many providers and educators may rely on computers to review notes and labs and to document the visit. This means there may be moments spent looking at the screen instead of the person sitting across from us.
Unfortunately, people with diabetes may feel that the computer is a distraction and a barrier to effective two-way communication.
Good news! There are strategies to compassionately engage with people with diabetes during the visit, while using the computer.
At the American College of Physicians Internal Medicine Meeting, speaker Wei Wei Lee MD, assistant professor of medicine at the University of Chicago, said utilizing the mnemonic HUMAN LEVEL provide guidance on how to succeed with electronic charting.
The mnemonic HUMAN LEVEL stands for:
H stands for honoring the golden minute. “The first minute of the visit with the patient should be completely technology free. Greet the patient, start with what’s on their mind, what their agenda is and then transition into using the computer,” she said.
U – Use the triangle of trust by placing the computer so that you and the patient can see the screen at the same time.
M – Maximize interaction by engaging the patients as much as possible, as you work on the computer.
A – Acquaint yourself with the patient’s chart before entering the examination room.
N – Not focusing exclusively on the screen during the visit, especially when the patient is talking about sensitive subjects.
For the complete mnemonic and more info on establishing a collaborative relationship, here is the article by Healio – “Doctors, patients benefit when the ‘eyes’ have it”
We have also created a resource page called the ABCs of Language Use in Diabetes, which provides insights on using strength-bases language in the clinical setting.
Within the medical community, we often use the terms “good cholesterol” and “bad cholesterol.” HDL, or high density lipoprotein cholesterol, is most often viewed as “protective from cardiovascular disease and death,” or the “good cholesterol” However, a recent study by the Emory University School of Medicine in Atlanta found that high levels HDL may actually be considered harmful.
The study assessed 60,000 men and women and tracked their cholesterol levels and risk for heart disease over the course of four years. HDL levels ranged, “from a low, less than 30 mg/dL to a high, greater than 60 mg/dL of blood.” Over the duration of the study, about 13% of test subjects either suffered from a heart attack or died.
“Specifically, patients with HDL levels exceeding 60 were found to have a 50 percent greater risk of heart disease death or heart attack, compared with those in the middle-range, the investigators reported.”
At the study’s end, the researchers concluded that patients with HDL levels in the middle-range of the spectrum — meaning between 41 to 60 mg/dL of blood — fared the best, having the lowest risk for heart attack or death from heart disease.
Allard-Ratick, head researcher on this study says concerned patients with high HDL cholesterol, “should continue to address other modifiable risk factors such as high blood pressure, smoking, and obesity to reduce cardiovascular disease”.
To read more about this study, visit Could too much HDL cholesterol be bad for your heart?
To learn more about cholesterol management, visit Cholesterol 101: An introduction.
 Appetite control is often associated with risk of obesity and Type 2 Diabetes. Researchers at the University of California, San Diego have found that leptin resistance may have a significant impact on hunger and satisfaction. In animal studies, a high-fat diet increases the amount of an enzyme named MMP-2, which damages leptin receptors that signal your brain when you’re full. When the hormone leptin’s receptor sites are damaged, the neurons do not send a satiety signal to the stomach to stop eating. This may explain why obese individuals often eat past the point of fullness.
Appetite control is often associated with risk of obesity and Type 2 Diabetes. Researchers at the University of California, San Diego have found that leptin resistance may have a significant impact on hunger and satisfaction. In animal studies, a high-fat diet increases the amount of an enzyme named MMP-2, which damages leptin receptors that signal your brain when you’re full. When the hormone leptin’s receptor sites are damaged, the neurons do not send a satiety signal to the stomach to stop eating. This may explain why obese individuals often eat past the point of fullness.
Leptin is released from white fat tissue, the most predominant form of fat, when a person is eating a meal. “Leptin travels through the bloodstream to the brain, specifically the hypothalamus, where it stimulates neural receptors to signal that the stomach is full.” Individuals who are overweight or obese typically have plenty of leptin in the blood, but due to the abundance of the MPP-2 enzyme, the system fails to send the signal of satiety to the hypothalamus.
This study found the enzyme MMP-2 is responsible for the damage to leptin receptors. Subjects who did not produce the MMP-2 enzyme gained less weight overall. Their leptin receptors still remained in tact. Researchers of this study, believe that, “other membrane receptors may be destroyed in the same way.” Further research must be conducted to determine if this is the case for other receptors as well.
This research team is calling for a large-scale clinical trial to investigate whether MMP-2 inhibitors might help people lose weight
For more information on leptin resistance, check out at the study Leptin Resistance and Appetite Control.
Contributed By: Sofia Sepulveda
 Today we celebrate International Day of the Girl!
Today we celebrate International Day of the Girl!
An important mission of Diabetes Education Services is to inspire girls to feel emboldened to chase their dreams!
Established by the United Nations in 2012, International Day of the Girl, was created to address the challenges girls face all over the world!
“International Day of the Girl promotes empowerment, education, and employment skills, alongside the attainment of basic human rights.
The 2018 theme is “With Her: A Skilled GirlForce”, and it focuses on properly equipping and training the 600 million adolescent girls who will enter the workforce within the next decade.
How can people work now to help these girls obtain secure, safe, and gainful employment within the next few years?”
At Diabetes Education Services we believe in supporting girls and women to realize their potential. We are dedicated to supporting the growth and well-being of our future generations. Today, we continue to celebrate our amazing sister organization, Just One Person.
 Just One Person, is a model sustainable program that prepares girls in rural Kenya for post secondary opportunities, helping them develop economic independence that will guide them on the path out of poverty.
Just One Person, is a model sustainable program that prepares girls in rural Kenya for post secondary opportunities, helping them develop economic independence that will guide them on the path out of poverty.
Diabetes Education Services partners with Just One Person to manufacture our Pancreas Partner. All profits from Pancreas sales are donated to Just One Person to help the girls pursue ongoing education and gainful employment.
Want to get inspired? – Enjoy these “11 Inspiring Quotes For International Day Of The Girl 2018, Because You Could Really Use A Boost Right Now” – Romper