Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Our March 23rd Question caused a lot of commotion. Less than half (43%) of respondents chose the best answer, so we wanted to dive deeper into this question of how many pens are needed.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR is 24 years old and uses an insulin pen for their basal insulin injections each evening. JR takes 30 units a night and each insulin pen holds 300 units of insulin.
How many insulin pens would JR need for one month?
Answer Choices:
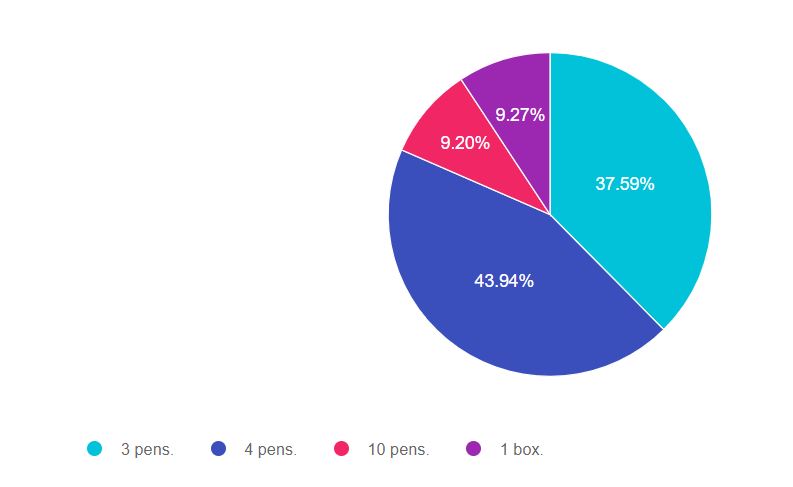
As shown above, the most common choice was option 2, the second most common answer was option 1, then option 4, and finally option 3.
We had over 1,500 attempts at getting to the best answer. If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to make sure the answer matches the key intent of the question. This is also a word problem. Setting up the problem correctly before doing the math is very important.
In this situation, we are asked to answer, “How many insulin pens would JR need for one month?” The main goal of this question is to make sure that test-takers incorporate the 2 unit air shot into calculating how much insulin is needed for the month.
Answer 1 is incorrect, 37.59% chose this answer, “3 pens.” JR takes 30 units of basal insulin a night. However, we know that JR needs to prime their insulin pen with a 2 unit air shot before each injection. To make sure the insulin pen and needle are working correctly, we instruct people to use a new pen needle and to prime the pen before injection. This means that JR will use 32 units of insulin each night (30 units for the injection, 2 units to prime the pen).
32 units x 30 days = 960 units. If each pen holds 300 units, 3 pens only hold 900 units. JR would run out of insulin at least 2 days ahead of time. For this reason, this answer is not correct.
Answer 2 is correct, 43.94% of you chose this answer, “4 pens.” Great job. You considered that JR needs to prime their pen before each injection.
JR takes 30 units of basal insulin a night. We know that JR needs to prime their insulin pen with a 2 unit air shot before each injection. To make sure the insulin pen and needle are working correctly, we instruct people to use a new pen needle and to prime it before injection. This means that JR will use 32 units of insulin each night (30 units for the injection, 2 units to prime the pen).
32 units x 30 days = 960 units. If each pen holds 300 units, JR will need 4 insulin pens for the month.
Answer 3 is incorrect, 9.20% of you chose this answer, “10 pens.” This was a juicy answer. Respondents who chose this probably looked quickly at the question and divided 300 by 30 to get 10 pens. In this question, paying attention to the details before diving into math is really important.
Each pen holds 300 units and JR takes 30 units of insulin a night. When you add in the 2 units to prime the pen, JR needs 4 insulin pens a month.
Answer 4 is incorrect, 9.27% of you chose this answer, “1 box.” This is another juicy answer. But, it doesn’t match the unit of measure of the question. The question asks, how many insulin pens and this response answers with a different unit, 1 box. The question also doesn’t ask how the prescription would be written. It only asks for how many pens. For this reason, this is not the best answer.
However, in the clinical setting, the prescription would be written for a box of 5 pens, since that is the usual dispensing unit.
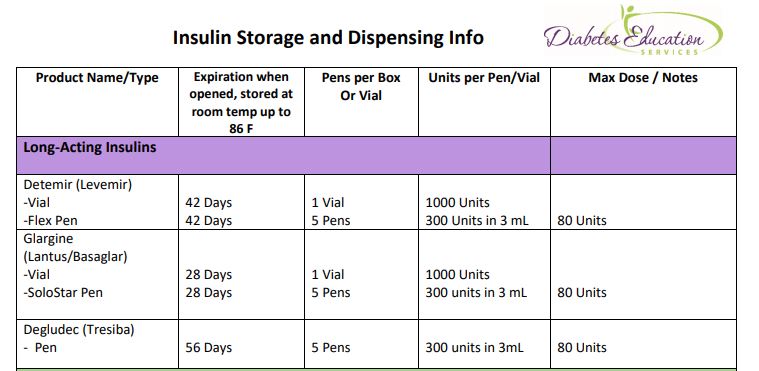
Insulin Storage Cheat Sheet – Download for FREE. Provides all kinds of important details on the storage of different types of insulin pens, vials, and more!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We interviewed the founder of Diabetes Education Services to discover her personal and professional motivations to go from a floor nurse to a leader in the field of diabetes.
Question: Why Did You Become a CDCES?

Coach Beverly: Over 20 years ago, as the Manager of our Health Education Department at CIGNA (an HMO), our team decided that we wanted to become a magnet site for diabetes care and education in our community. To achieve this, we encouraged our entire team to study for their CDE (now CDCES) to showcase our dedication to providing the best diabetes care.
Question: Has Holding the CDCES Credential Provided You with Additional Professional Opportunities? Please share one or two examples.
Coach Beverly: Holding this credential has been the best professional decision of my career. Having a master’s degree plus my CDCES opened the door for me to be hired as the Diabetes Nurse Specialist at Stanford Hospital in 1994. Working at Stanford provided me the opportunity to initiate bold strategies to improve diabetes care and outcomes in a busy, demanding, and innovative teaching hospital. I learned how to manage very complex patients and build interdisciplinary professional teams to provide the best care from admission to discharge and beyond.
My experience as a Diabetes Specialist at Stanford Hospital gave me the confidence, clinical knowledge and courage to launch my own company.
In 1998, I applied for my first business license as Diabetes Education Services. Our company is dedicated to helping health care professionals realize their dream of becoming certified diabetes specialists. In operation for over 20 years, our small but mighty organization is laser-focused on providing high-quality resources and services for our community of health care professionals.
I love coming to work every day and figuring out new ways of delivering content that is meaningful, evidence-based, and infused with compassion.
Without my CDCES, none of these life-changing opportunities would have been possible.
Question: What Would you Say to Someone Who is Considering Becoming a CDCES in the Future?
Coach Beverly: Welcome to our awesome community! Every day that I show up to work as a diabetes specialist, I feel that I am a part of something bigger. This community passionately and collectively works toward improving the care and quality of life for people living with diabetes. Diabetes specialists also have the opportunity to work in a variety of settings, to teach individuals or groups, or on a community level to advocate for excellence in diabetes care. Even though I have worked in this field for over 20 years, I am challenged, I have the opportunity to role-model compassionate care and I love the people I get to work with.
Question: Share an Achievement or Special Moment You’ve had working as a CDCES?

Coach Beverly: An achievement that I am particularly proud of is the LifeChanger of the Year Award. I was nominated by a person with diabetes who attended our hospital’s diabetes self-management program we called “Diabetes Survival Camp.” She was an enthusiastic participant and brought her husband to each class. After graduation, she started attending our monthly support group and shared a lot of helpful information. When I received the letter that she had nominated me for this prestigious national award and I had won, I was overjoyed and deeply touched.
Her nomination reminded me that the everyday work we do touches people profoundly.
We listen, help with problem-solving, and we lift people up who are discouraged. We celebrate their victories and we let them know through our words and gestures that we believe in them. There is no better job in the world.

This course will transform your test anxiety into calm self-confidence and test-taking readiness.
We will review sample test questions and the reasoning behind choosing the right answers. After registering, you will receive a confirmation email containing information about joining the webinar.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator who has passed her CDCES Exam 6 times. She is a nationally recognized diabetes expert for over 25 years.
Virtual DiabetesEd Specialist Conference | April 15-17, 2021
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice. If you are interested in taking the CDCES or BC-ADM exam or are seeking a state-of-the-art review of current diabetes care, this course is for you.
Entire Program Fee: $399
Dates: April 15-17, 2021
3 Expert Speakers
CEs: 30+ CE hours
Live Webinar Schedule: All webinars start and end times are in Pacific Standard Time
Come join our Virtual DiabetesEd Specialist Program.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.
This virtual program includes:
3 day live webinar courses from April 15th-17th (20 CEs) + enrollment in our Bonus Bundle (14.0+ CEs) from now through December 2021.
View full Conference Schedule and Faculty.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our March 16th Question of the Week, over 86% of respondents chose the best answer!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: PZ arrives for their diabetes appointment with their food diary and glucose log book. PZ’s blood glucose levels have improved since last visit by about 20 points, with morning glucose levels in the 130 range and bedtime glucose in the 180 range. When you ask PZ about what changes they have made, PZ shrugs their shoulders and says, “I quit eating tortillas because my children said they are bad for me.”
What is the best response?
Answer Choices:
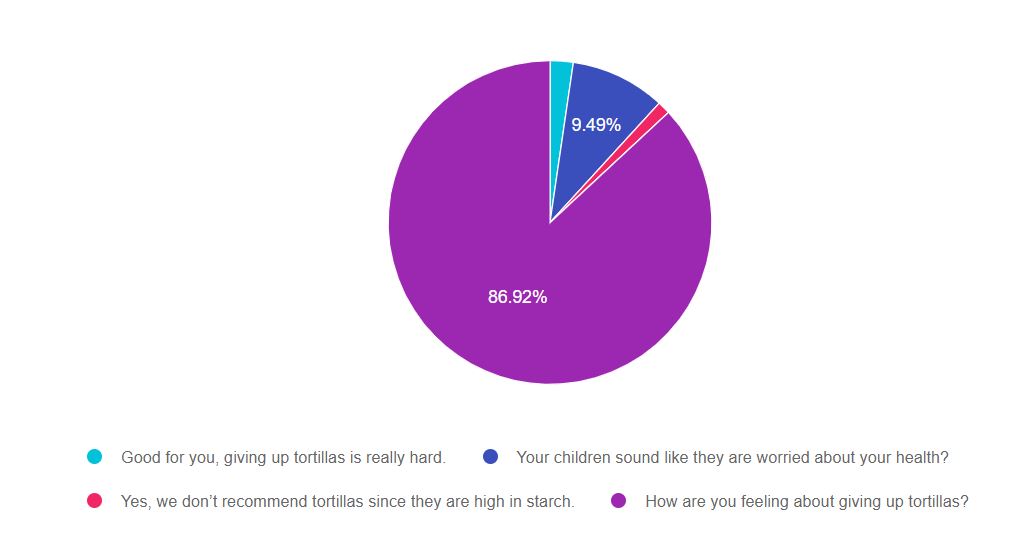
As shown above, the most common choice was option 4, the second most common answer was option 2, then option 1, and finally option 3.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to apply a blend of science coupled with psychosocial awareness to determine the best answer.
Answer 1 is incorrect, 2.31% chose this answer. “Good for you, giving up tortillas is really hard”. We notice that PZ shrugs their shoulders when they tell us they have given up tortillas. In addition, PZ states that they have stopped eating tortillas, not because they think it is best for them to stop, but because their children advised them that tortillas are bad. The word “bad” is loaded with judgment and perhaps PZ is feeling ashamed for eating this traditional food that has been part of their everyday life for decades. For this response, instead of affirming giving up tortillas, a better choice would be to explore this choice further.
Answer 2 is incorrect, 9.49% of you chose this answer. “Your children sound like they are worried about your health?” This seems like an accurate response, but is it the BEST response? The goal of DSME is to provide a person-centered approach. This question puts the emphasis on the children’s belief that tortillas are bad instead of exploring how the person with diabetes is responding to this drastic behavior change.
Answer 3 is incorrect, 1.28% of you chose this answer “Yes, we don’t recommend tortillas since they are high in starch.” One corn tortilla has 15gms of carbohydrate, plus fiber and other micronutrients. Tortillas can absolutely be included as part of a healthy meal plan. In addition, tortillas are more than a serving of starch, they are a central and traditional part of the meal for many cultures.
Answer 4 is correct, 86.92% of you chose this answer. ” How are you feeling about giving up tortillas?” GREAT JOB. Most of you chose this person-centered response which gives us an opportunity to see how giving up tortillas is impacting PZ from an emotional standpoint. As diabetes specialists, we know that eliminating tortillas completely may not be the best choice from an evidence-based and emotional perspective.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our March 9th Question of the Week, over 67% of respondents chose the best answer!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR wants to lose weight in the next 30 days by drinking less juice. There are 100 calories per glass of juice and JR usually drinks 3 glasses a day.
How much weight would JR lose by only drinking 1 glass a day?
Answer Choices:
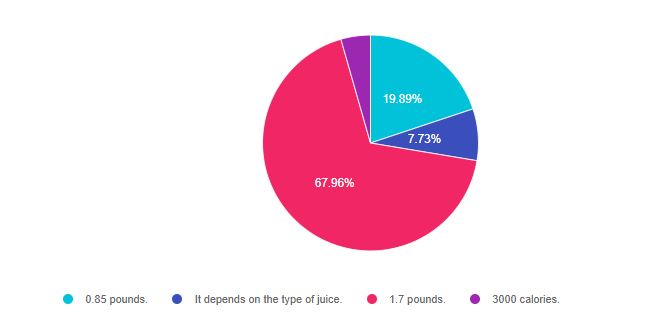
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to apply their math skills to a word problem and choose the BEST answer. If you see a question that requires math, just take a deep breath, read the question carefully and call upon your abundant common sense. For this particular question, we also need to know that 1 pound equals 3,500 kcals.
Answer 1 is incorrect, 19.89% chose this answer. “0.85 pounds”. This was the juicy answer designed to distract test takers from the best answer. JR was drinking 3 glasses of juice and is reducing their intake by 2 glasses of juice. Their net calorie reduction, therefore, is not one glass a day, but 2 glasses a day. Each glass contains 100 calories, leading to a 30-day calorie deficit of 6,000 calories a month (not 3,000 calories).
Answer 2 is incorrect, 7.73% of you chose this answer. “It depends on the type of juice”. Since we are given the caloric content of the juice, we don’t need to know what kind of juice to get the best answer.
Answer 3 is correct, 67.96% of you chose this answer “1.7 pounds”. Good job. JR was drinking 3 glasses of juice and is reducing their intake by 2 glasses of juice. Each glass contains 100 calories. This leads to a 200 calorie a day deficit, and a 30-day calorie deficit of 6,000 calories. 6,000 calories divided by 3,500 calories (1 pound) equals 1.7 pounds.
Answer 4 is incorrect, 4.42% of you chose this answer. “3,000 calories”. If you go back to the root of the question, it asks the test taker, “How much weight” would JR lose. Weight is expressed in kg or pounds, not calories. By making sure the answers’ unit of measure matches the questions’ unit of measure, test takers can eliminate wrong answers.
Special note: I want to acknowledge that weight and weight loss are complicated. It is so much more than a function of calories consumed or deprived. There are hormones, genetics, set-points, co-conditions, and a whole range of other influencing factors that contribute to weight at any given time. This sample test question does not address these factors since its main focus was providing a word problem with math calculations.
I would encourage you to check out this blog on Diabetes and Diet Culture, which interviews Megrette Fletcher, M.Ed., RD, CDCES, co-founder of The Center for Mindful Eating, co-founder of WN4DC Symposium, and author of five mindful eating books. Megrette is a trailblazer in the field and offers a new approach that values the individual first and encourages us to address our own weight biases.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 24 years old and uses an insulin pen for their basal insulin injections each evening. JR takes 30 units a night and each insulin pen holds 300 units of insulin.
How many insulin pens would JR need for one month?
Click here to test your knowledge!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
It’s National Nutrition Month!

We have compiled a list of plant-based therapy articles and resources to celebrate the importance of nutrition.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 64 years old, in hospital with type 2 diabetes and COVID. JR normally manages their diabetes with metformin, but during this inpatient stay, JR is on prednisone therapy which has spiked sugar levels into the 250 mg/dl to 350 range. JR is receiving bolus insulin sliding scale with meals and bedtime glargine, but blood sugars are persistently elevated. To improve outcomes for JR, it is important to keep blood glucose levels less than 180 mg/dl, but what should we recommend to get glucose to goal?
What are some strategies to get blood sugar to target while on steroids?
There is no consensus on the best approach to manage this situation. Up until this point in history, steroid-induced hyperglycemia was mostly found in people with diabetes in COPD, those undergoing chemotherapy or in post-transplant situations.

With the COVID pandemic, many people with diabetes in hospitals and at home, are on steroids. Health care professionals are trying to figure out how to lower glucose levels.
For people with type 2 diabetes and COVID, the latest research indicates that sitagliptin (Januvia) not only helps maintain blood glucose but also decreases the inflammatory response associated with COVID infections. If not contraindicated, sitagliptin can be used in conjunction with insulin, to treat the extreme insulin resistance and hyperglycemia caused by steroid therapy.
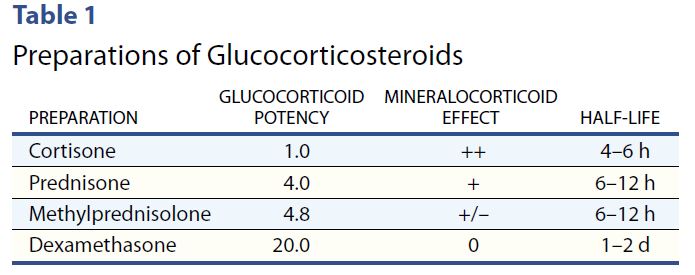
To treat steroid induced hyperglycemia, we are going to call on our old insulin friend, NPH. Neutral Protamine Hagedorn (NPH) is an intermediate acting basal insulin. NPH insulin is made by mixing regular insulin and protamine in exact proportions with zinc and phenol such that a neutral-pH is maintained and crystals form.
NPH insulin is cloudy and has an onset of 1–4 hours. Its peak is 6–10 hours and its duration is about 10–16 hours.
Steroids have their highest potency at 4-12 hours, with the exception of the very potent dexamethasone, which has a half life of 1-2 days.
However, with all steroids, including dexamethasone, people will experience elevated glucose values after breakfast, lunch, dinner, and at bedtime but will have a significant drop toward normal glucose overnight.
Therefore, hyperglycemia is greatest 1–2 hours after a meal, with persistent elevation until the following meal, followed by a return to normal overnight.

NPH Insulin Dosing Strategies
There are several articles (see below) that recommend a variety of NPH dosing strategies. Generally, insulin dosing is based on a combination of steroid dose and body weight. For those on lower dose steroid (ie less than 40 mg prednisone daily) a starting NPH insulin dose of 0.1 – 0.2 units per kg is reasonable. If JR weighs 100 kg, that means 10 to 20 units of NPH daily.
If JR is on a higher steroid dose, or blood sugars are extremely elevated, JR may need 0.3 units/kg or 30 units of NPH daily. Of course, we also need to keep nutritional status in mind as we determine best dose. People who are not eating or NPO, will require less insulin, even in the presence of steroids.
The timing of NPH administration matches the timing of the steroid therapy.
In addition, coverage for carbohydrates at meals and correction insulin bolus for hyperglycemia can help prevent post-prandial hyperglycemia.
A simple getting started strategy – 70/30 Insulin
A simple strategy I have used over many years, that I find safe and effective, is giving the basal-bolus premixed 70/30 insulin with the morning dose of steroid. A safe starting range is around 10 units in the morning and gradually increases 10-20% daily to get glucose to target. In addition, bolus coverage for carbs and hyperglycemia can be given at lunch and dinner.
Since blood sugars trend down overnight, nighttime NPH insulin is not usually needed.
Keeping it flexible
As the person starts recovering and steroid doses are gradually tapered down, it is important to also decrease the NPH insulin dose and bolus insulins to prevent hypoglycemia.
In conclusion:
Keeping blood sugars on target improves outcomes. For people with diabetes, steroids can cause a hyperglycemic crisis. Thoughtful and progressive management using NPH and bolus insulins can turn the tide and help get blood glucose levels to goal.
Join Coach Beverly at our Virtual Conference for more information on COVID and Diabetes Management Strategies.
Glycemic Control in Hospitalized Patients with Diabetes Receiving Corticosteroids Using a Neutral Protamine Hagedorn Insulin Protocol: A Randomized Clinical Trial. Khowaja A, Alkhaddo JB, Rana Z, Fish L. Diabetes Ther. 2018 Aug;9(4):1647-1655.
How to Manage Steroid Diabetes in the Patient With Cancer
David S. Oyer, MD, FACE, Ajul Shah, BS, and Susan Bettenhausen, APRN, CDE, 2006
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
If you are interested in taking the CDCES or BC-ADM exam or are seeking a state of the art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.