
Our April 31st Question of the week was a question about aerobics, hypothyroidism, cholesterol, and type 2 diabetes. Although 58% of respondents chose the correct answer, 42% did not. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
You are working with KS, a 57-year-old with type 2 diabetes, who wants to join the water aerobics program at their local YMCA. KS has a history of hypothyroidism and has an LDL cholesterol of 98 mg/dl. KS’s medications include levothyroxine and metformin XR 1000 mg BID.
According to the ADA and the American College of Sports Medicine, what would be the best recommendation?
Answer Choices:
- Encourage KS to join the water aerobics program.
- Recommend that KS get an EKG before starting this new activity.
- Ask KS’s provider to order a stress test.
- Make sure KS monitors blood glucose before and after exercise class.
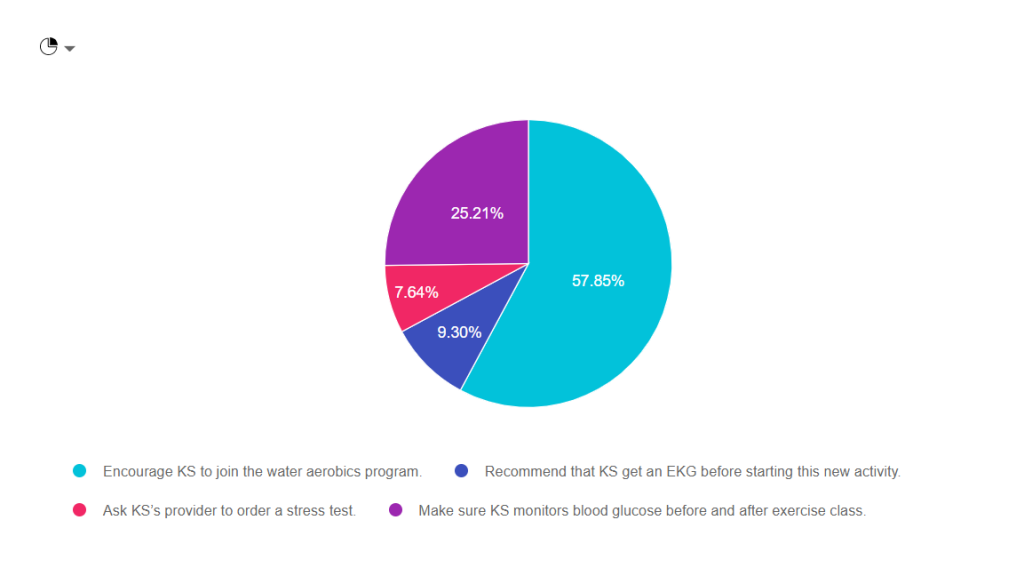
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.

Answer 1 is Correct! Encourage KS to join the water aerobics program. Based on the information provided, she would benefit from adding activity to her routine. Exercise decreases visceral adiposity, improves mood, lower glucose by enhancing insulin sensitivity. See our Exercise Resource Page for helpful info.
Answer 2 is incorrect. About 10% of respondents chose “Recommend that KS get an EKG before starting this new activity.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting an EKG for those with risk factors for cardiovascular events.
Answer 3 is also incorrect. About 10% of respondents chose “Ask KS’s provider to order a stress test.” In the past, we would recommend that people with diabetes get a stress test or EKG before starting any new exercise. The new guidelines only recommend getting a stress test for those with risk factors or symptoms of cardiovascular events.
Finally, Answer 4 is incorrect. “Make sure KS monitors blood glucose before and after exercise class.” Having diabetes is a lot of work. As diabetes specialists, it is important that we don’t unnecessarily increase the burden of daily self-care. While KS may gain interesting information by checking BG levels before and after exercise, it is NOT necessary to monitor glucose before and after.
Why not? Since KS is not on any medication that causes hypoglycemia, her risk of low blood sugar is almost none. In addition, most people on oral medications are only allotted one strip a day to monitor blood sugars. Asking KS to check twice on water aerobics days may translate to extra out of pocket expenses that can also add to the financial burden of diabetes.
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
Resources for Pre-exercise Evaluation
This article on page 154 Exercise and Type 2 Diabetes American College of Sports Medicine /American Diabetes Association joint position statement on exercise and type 2 diabetes.
Pre-exercise Evaluation- 2020 Standards Of Care
The ADA consensus report “Screening for Coronary Artery Disease in Patients With Diabetes” (172) concluded that routine testing is not recommended. However, providers should perform a careful history, assess cardiovascular risk factors, and be aware of the atypical presentation of coronary artery disease in patients with diabetes. Certainly, high-risk patients should be encouraged to start with short periods of low-intensity exercise and slowly increase the intensity and duration as tolerated. Providers should assess patients for conditions that might contraindicate certain types of exercise or predispose to injury, such as uncontrolled hypertension, untreated proliferative retinopathy, autonomic neuropathy, peripheral neuropathy, and a history of foot ulcers or Charcot foot. The patient’s age and previous physical activity level should be considered. The provider should customize the exercise regimen to the individual’s needs. Those with complications may require a more thorough evaluation prior to beginning an exercise program (171).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]