
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
As we enter fire and storm season, it’s always a good idea to think ahead and be prepared for disaster. For people living with diabetes, a “diabetes kit” is an important part of emergency preparedness. We are excited to share a few getting ready checklists and resources that we think are really helpful.
For any emergency scenario, it’s important to have an emergency preparedness plan that includes a meeting point, an exit route, a “get-away” bag, and communication strategies. Identify and inform the people who will be included in the emergency plan ahead of time and make sure everyone clearly knows what to do and what action to take.
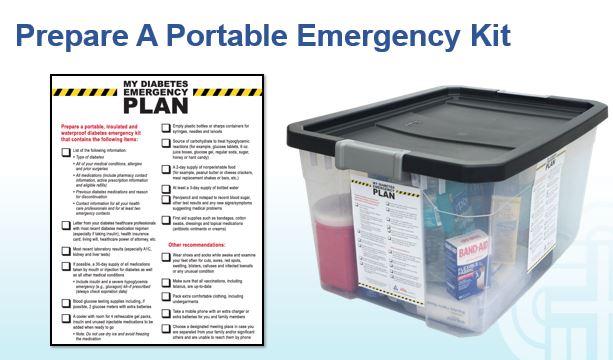
An easy way to get started is to download the Checklist and Plan created by the Diabetes Disaster Response Coalition. We have also created a Disaster Checklist Word document that you can download and customize for yourselves. These checklists can help you start the conversation and commit the details to paper.
Disaster can happen in a moments notice. It’s important to plan ahead and be ready, especially for people living with diabetes.
Resources for People with Diabetes
General information from the Diabetes Disaster Response Coalition (DDRC) on preparedness for people living with diabetes.
Have an Emergency Diabetes Plan and Kit Ready: DDRC’s Diabetes Plan and Kit checklist includes helpful steps to take in preparation for disaster. The checklist details needed supplies and information that should be written down and kept in a waterproof container for emergency situations where is can be found by a health care provider to make informed emergency treatment decisions.
Stay Updated: Visit Breakthrough Type 1 Disaster Relief Resources and Diabetes Disaster Response Coalition includes information on how to access medical support, shelters, and open pharmacies during times of disaster.
Individuals with diabetes who need help: Call 1-800-DIABETES (800-342-2383). The American Diabetes Association Center For Information is open, MON.-FRI. 9 a.m. TO 7 p.m. ET. Representatives are regularly updated with information on how to access medical support, shelters, pharmacies, and more.
American Red Cross Shelters: Contact the American Red Cross directly at 1-800-RED-CROSS.
Resource For Health Care Providers:
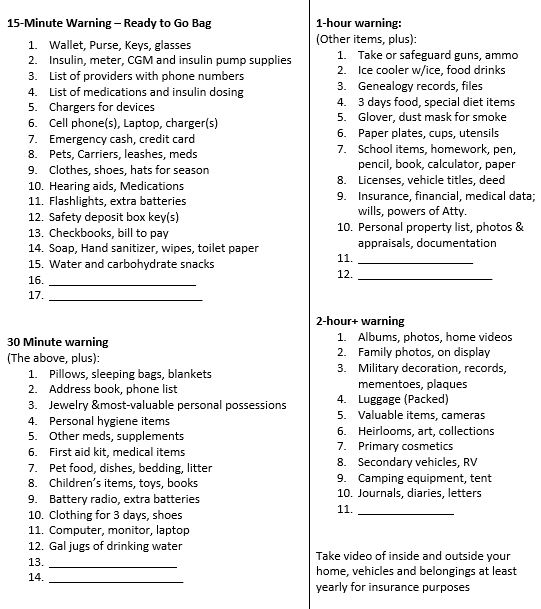
In addition to the items listed below, make sure to pack hand sanitizer, wipes, and masks due to the current pandemic. Also, bring your own pillow and bedding in case you need to spend time in a shelter.
Emergency Evacuation-Items to Gather for People with Diabetes
We thought this list was a helpful way to prioritize what items to grab given different time frame limitations. We found it online and customized it for people with diabetes. It is available in Word or PDF. Thank you for sharing with your colleagues and community.
1-800-DIABETES (800-342-2383) is an excellent referral resource for people with diabetes to call toll-free for updates on accessing medical support during an emergency.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Increasing global temperatures are expected to impact the health of people living with diabetes and lead to worse outcomes, according to an article published in the Journal of Community Hospital Internal Medicine Perspectives,

People with diabetes are at greater risk of experiencing dehydration and cardiovascular events during periods of extreme heat. Several studies reveal that people with diabetes are more likely to need emergency care during heat waves and those with a history of heart disease are most vulnerable.
To keep healthy and reduce risk during heatwaves, we have put a list together of actions people with diabetes can take to stay safe in the heat.
Download PDF Handout of 19 Actions Here


 Once weekly basal insulin, icodec, failed to be approved for use by people with type 1 diabetes by the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee by a vote of 7-4. The significantly increased risk for hypoglycemia on days two through four after administration outweighed its potential benefits. The committee also noted that icodec’s risk of hypoglycemia is higher than the basal insulin degludec, which is commonly used and has a better safety profile. Other committee members expressed concerns that approving icodec based on inadequate data could discourage further trials that are needed to ensure its safe use.
Once weekly basal insulin, icodec, failed to be approved for use by people with type 1 diabetes by the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee by a vote of 7-4. The significantly increased risk for hypoglycemia on days two through four after administration outweighed its potential benefits. The committee also noted that icodec’s risk of hypoglycemia is higher than the basal insulin degludec, which is commonly used and has a better safety profile. Other committee members expressed concerns that approving icodec based on inadequate data could discourage further trials that are needed to ensure its safe use.
In an effort to secure approval, the applicants for icodec suggested the following actions to improve the safety profile of this novel weekly insulin.
Proposed mitigating actions to reduce hypoglycemia risk by the applicant included;
Even though mitigating actions were suggested to decrease this hypoglycemia risk during this two day peak, the FDA panel members still deferred approval, citing safety concerns due to the significant hypoglycemia risk and need for more data..
Surprisingly, about one third of people living with type 1 diabetes are still managing blood sugars with multiple daily injections. This is especially true for people living in under resourced communities and people of color living with type 1 diabetes. Due to barriers and social determinants of health, in addition to struggling with multiple daily injections, they are also less likely to use continuous glucose monitors or check blood sugars on a regular basis. Although, once a week insulin seems ideal for individuals who may be experiencing a variety of barriers to injecting daily insulin, the main issue is the increased risk of hypoglycemia during days 2-4 when icodec is peaking coupled with limited access to glucose monitoring.
In addition, consistent injected insulin therapy in adults with type 1 diabetes was reported to be relatively low (52.6%, 95% confidence interval[CI]: 37.4 to 67.9%) in data from a meta-analysis of eight clinical trials. The probability of missing at least one daily basal insulin dose over any 14-day period is estimated to be 22% (95% CI: 10 to 40%).
Among individuals with type 2 diabetes, using a daily basal insulin, a once weekly basal insulin would reduce the number of insulin injections from 365 per year to 52 per year. In a recent study, 91% of people with type 2 diabetes and 89% of providers had a positive view of taking basal insulin once weekly.
Among individuals with type 1 diabetes, who rely on a basal bolus regimen, a once weekly basal insulin would reduce the number of insulin injections from approximately 28 per week to 22 per week. For those with type 1 diabetes, there is no research to date that evaluates whether a once weekly basal insulin would be preferred over other basal insulin options, or whether use would result in improved adherence and glycemic control.
In ONWARDS 6, weekly insulin icodec was noninferior (but not superior) to daily insulin degludec and was associated with 48 to 89% more level two and three hypoglycemia at Week 26, depending on the method of analysis. The highest risk period for hypoglycemia with insulin icodec coincides with its peak glucose-lowering effect which occurs on days 2 to 4 following each weekly injection. There were also more hypoglycemia-related serious adverse events reported among patients randomized to insulin icodec compared to insulin degludec.
Thus, in the only study conducted in participants with type 1 diabetes, insulin icodec was observed to have a higher risk of clinically meaningful hypoglycemia, in the absence of a lower A1C. Hypoglycemic episodes reported with insulin icodec and insulin degludec in ONWARDS 6 were of the same nature in terms of duration, management, and recovery.
Insulin icodec is an acylated long-acting human insulin analog produced by a process that includes expression of recombinant DNA in yeast (Saccharomyces cerevisiae), followed by chemical modification. In addition to amino acid sequencing changes, a C20 fatty-acid side chain has been added to the peptide backbone via the amino group in the side chain at Lys(B29). When insulin icodec is injected, the C20 fatty acid sidechain derivative binds strongly, but reversibly, to endogenous albumin, which results in decreased renal clearance and protection from metabolic degradation, and consequently prolonged pharmacodynamic activity.
Insulin icodec is a proposed insulin analog with a prolonged duration of action intended to support once weekly (QW) subcutaneous administration. Thus, insulin icodec reduces treatment burden in type 1 diabetes, by reducing the number of basal insulin injections in comparison to daily basal insulins.
However,basal insulin icodec does not have a peakless time-action profile throughout the dosing interval (see chart below).
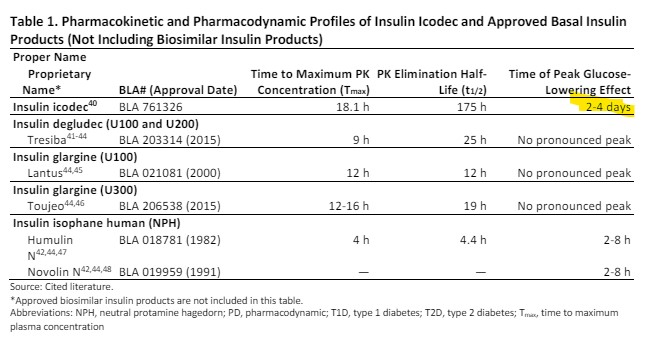
In conclusion, it seems certain that the manufacturers of insulin icodec will be seeking approval for this once weekly insulin for people living with type 1 and type 2 diabetes in the future. Stay tuned for more insulin updates with our monthly newsletter.
Information from this article was obtained from review of the FDA Presentation Document and Slides, May 24, 2024.
In our rural clinic, we are starting more and more individuals on glucose sensors. People’s response to using a CGM device has garnered mixed reactions. Most individuals are thrilled that they can see their blood sugars are at a glance with fewer finger pricks. They feel empowered with this play-by-play blood sugar report.
However, others experience a sense of overwhelm in response to the sudden onslaught of glucose data on their screen. This stress becomes more acute as they hone in on sugar spikes or sudden lows that don’t seem to have a rhyme or reason. In addition, many people are confused by the discrepancy between the meter and sensor glucose, causing even more upset.
These individuals may experience an understandable amount of confusion, frustration, and distress.
This newsletter provides a range of tools and resources to assist you in addressing these distress points, detailed in the following featured articles.
Our first article explores the reasons behind the gap between CGM and meter readings. We also provide a CGM Troubleshooting Cheat Sheet that you can share with your colleagues and clients.
Next, we outline a step-by-step communication approach designed to help individuals adjust to sensor data overwhelm using a person-centered approach.
Finally, we address diabetes distress by interviewing expert Susan Guzman, PhD. You are invited to join Dr. Guzman and Larry Fisher, PhD, who will share their expertise on this topic in June, during our highly popular ReVive 5 training program.
Our last article recognizes the healing relationship we have with our pets. Challenge yourself with our Question and Rationale of the Week and please keep in touch.
Sending notes of joy and health, Coach Beverly, Bryanna, and Christine |
Featured Articles
Upcoming Webinars




Are you a diabetes health care professional or person with diabetes who is ready to get on track with your diabetes?
We want to encourage you to let your community know about an exciting research opportunity.
We are inviting people diagnosed with type 2 diabetes less than 5 years ago, who live anywhere in the U.S., with a most recent A1C of 7.5% or higher to click this link below to see if they qualify for the study.
If so, the Behavioral Diabetes Institute is conducting a research study examining how innovative new approaches to diabetes education might help to improve glucose outcomes and quality of life outcomes. Participants will be randomly assigned to take part in one of two different live, online, group education programs. Each group program will be lively and informative, and will meet once weekly for 5 weeks in a row.
Also, half of the participants will receive a continuous glucose monitor and free testing supplies.
To find out more and see if you might qualify, click below to apply. Or for more information, email them at [email protected] or call us at 858-336-8693.