Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Question of the Week | Why did 16 year old stop taking meds?


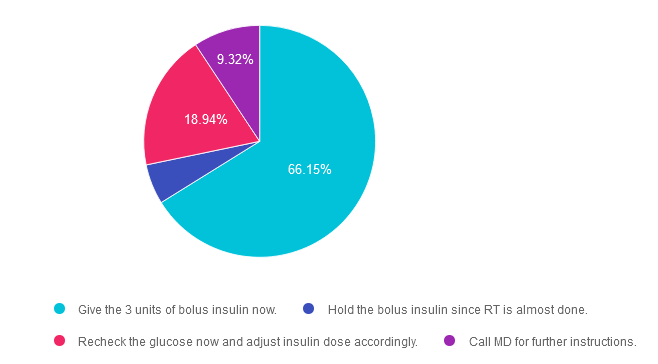
Rationale of the Week | Inpatient didn’t get bolus insulin before lunch. What is best action?

Save $100 on Most Popular Online Bundles

Visit Our Online Store Today to Save $100
The Imperfections of BMI

Question of the Week | What does Medicare Cover?

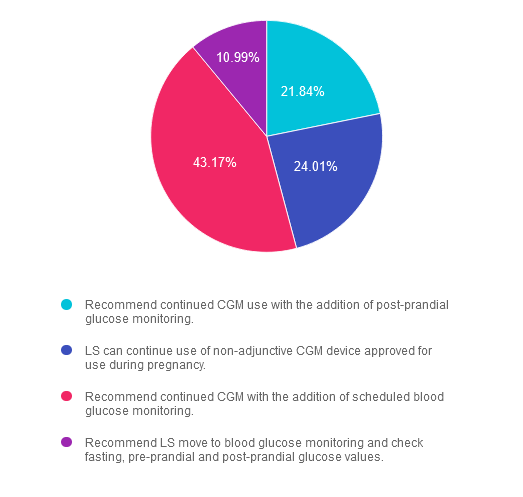
Rationale of the Week | ADA Standards for Gestational Diabetes

Question of the Week | Inpatient didn’t get bolus insulin before lunch. What is best action?
June 2024 eNews | Weekly Insulin, BMI, Updated CDCES Exam, 5 Activity Activators
Happy June
|
When I started in diabetes, we had two injectables, NPH and regular insulin. Fast forward to last month, the FDA evaluated the safety and efficacy of a once-a-week basal insulin called icodec. Citing safety reasons, the FDA denied the approval of icodec for people living with type 1 diabetes based on the data results. While researching this article, I discovered a concerning statistic: about 30% of people with type 1 still use multiple daily injections, especially in under-resourced communities. This statistic highlights the significant gap in access to diabetes technology and access in the U.S., and I consider it a call to action. In addition to detailing icodec insulin in this newsletter, we explore BMI as a health indicator and contemplate if communities would benefit from a more predictive and less stigmatized weight assessment. We prepare for the updated CDCES exam and highlight the significant changes starting July 1st. These changes reflect crucial knowledge needed to promote the best diabetes care. You are invited to check out our targeted resources to support CDCES success and promote excellence in diabetes care. With summer around the corner, we provide strategies to help people move forward with their activity goals and PLAN for setbacks. Plus, we have created a handy activity cheat sheet. Lastly, we are excited to announce that we are opening up the first session of ReVive 5 for FREE. This is a unique opportunity for you to join two experts in the field as they provide concrete strategies to evaluate and address diabetes distress. The session is designed to provide valuable support and care, and we believe it’s an opportunity you won’t want to miss. Our San Diego Scholarships are still open, and we would love to see you at this fun and intensive conference. This is a valuable experience to enhance your knowledge and skills in diabetes care, and we encourage you to consider applying. |
|
|
|
Sending notes of joy and health, Coach Beverly, Bryanna, and Christine |
Featured Articles
- Once a Week Insulin Denied by FDA
- Is BMI the Right Measurement?
- CDCES Exam Updates – Begins July 1st
- 5 Activity Boosters
- Question of the Week
- Rationale of the Week
Upcoming Webinars
- Pregnancy & Diabetes – June 11th
- Hospitals & Hyper- June 13th
- ReVive 5 – June 17th & 24th
- Setting up a DSME Program- June 20th
- Prep for NEW CDCES Exam – June 25th