Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Tirzepatide approved for weight loss

The U.S. Food and Drug Administration approved tirzepatide (Zepbound) injection for chronic weight management in adults with a BMI of 30 or with a BMI of 27 or greater with at least one weight-related condition (such as high blood pressure, type 2 diabetes, or high cholesterol) this November. Tirzepatide is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist.
Up to 25% body weight loss
The SURMOUNT clinical trials demonstrated that tirzepatide therapy not only improved glucose levels but also had a substantial impact on body weight reduction. At the highest dose (15 mg), people taking Zepbound lost on average 48 lb., while at the lowest dose (5 mg), people lost on average 34 lb. (compared to 7 lb. on placebo).
Additionally, 1 in 3 clinical participants taking Zepbound at the highest dose lost over 58 lb. (25% of body weight), compared to 1.5% on placebo, according to data not controlled for type 1 error. The average starting weight was 231 lb. Zepbound is recommended along with healthy eating and increased activity.
About the SURMOUNT clinical trial program
The SURMOUNT phase 3 global clinical development program for tirzepatide in chronic weight management began in late 2019 and has enrolled more than 5,000 people with obesity or overweight across six registration studies, four of which are global. SURMOUNT-1 and SURMOUNT-2 were submitted to the FDA and demonstrated tirzepatide significantly reduced body weight compared with placebo in people living with obesity or overweight, with or without type 2 diabetes.
The dual action of tirzepatide on both GIP and GLP-1 receptors allows for a comprehensive approach to blood sugar regulation with substantial weight loss. Tirzepatide, the active ingredient in Zepbound, is already approved under the trade name Mounjaro to be used along with diet and exercise to help improve blood sugar in adults with type 2 diabetes. With this new FDA approval for weight loss, people who meet the BMI and risk criteria qualify to use this novel medication class, whether or not they have diabetes.
Cost
Zepbound is expected to be available in the U.S. by the end of the year in six doses (2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg) at a list price of $1,059.87
Side effects:
Zepbound may be associated with gastrointestinal adverse reactions, sometimes severe. The most commonly reported adverse events (observed in ? 5% of clinical trial participants) were nausea, diarrhea, vomiting, constipation, abdominal pain, dyspepsia, injection-site reactions, fatigue, hypersensitivity reactions, eructation, hair loss, and gastroesophageal reflux disease. In studies, most nausea, diarrhea, and vomiting occurred when people increased their dose – but the effects generally decreased over time. Zepbound may cause tumors in the thyroid, including thyroid cancer. Watch for possible symptoms, such as a lump or swelling in the neck, hoarseness, trouble swallowing, or shortness of breath, and avoid using if there is a family history of medullary thyroid carcinoma (MTC).
For more information, see FDA Approval Information.
Want to learn more about Diabetes Medications?
Meds Management Update for Type 2 Diabetes
Airs live on December 21, 2023, at 11:30 am PST
Topics:
- Describe the role of Diabetes Care & Education Specialists in advocating for optimal therapeutic approaches.
- Discuss the application of the new ADA/EASD Guidelines to improve glucose and reduce CV and renal risk.
- List strategies to initiate & adjust oral & injectable therapy using a person-centered approach.
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Question of the Week | Best approach with Low Literacy?
Which of the following strategies is most effective when working with someone with low literacy skills?
- Be concrete and focus on problem solving.
- Speak slowly and clearly.
- Direct the teaching to the support person and encourage reinforcement.
- Underline key points on educational materials.
Click Here to Test your Knowledge
Want to learn more about this question?
How to Assess Well-Being | From Populations to Individuals
Airs live on December 19th, 2023, at 11:30 am PT
Topics:
- State strategies to assess & address social determinants of health.
- Discuss healthcare delivery systems using a person-centered approach.
- List screening tools that can help detect depression, trauma, & cognitive decline.
- Describe psycho-social & emotional barriers to diabetes self-management.
- Provide strategies for healthcare professionals to identify & overcome barriers to self-care.
Providing exceptional diabetes care and education begins with our first meeting with an individual with diabetes. Coach Beverly will delve into person-centered interview approaches, including assessing social determinants of health, motivational interviewing & practical communication approaches. This course offers critical content that will help with certification exam success.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Meds Management Update for Type 2 Diabetes
Airs live on December 21st, 2023, at 11:30 am PT
Topics:
- Describe the role of Diabetes Care & Education Specialists in advocating for optimal therapeutic approaches.
- Discuss the application of the new ADA/EASD Guidelines to improve glucose and reduce CV and renal risk.
- List strategies to initiate & adjust oral & injectable therapy using a person-centered approach.
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Upcoming webinars | Hyperglycemic Crises, DKA & HHS Standards & CDCES or BC-ADM – Which Certification is Right for me?

Be a part of our diabetes community while learning about the latest in diabetes care. Plus, Coach Beverly provides an interactive question and answer session at the end of each live webinar.
Join us for our upcoming Hyperglycemic Crises, DKA & HHS Standards webinar
Airs live on December 12th, 2023, at 11:30 am PT
Topics:
- Discuss the common causes of hyperglycemic crises.
- List the differences & similarities between DKA and HHS and treatment strategies.
- Describe the causes & treatment of hyperglycemic crises.
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
CDCES or BC-ADM – Which Certification is Right for me?
Airs live on December 13th, 2023, at 11:30 am PT

Are you considering pursuing certification in diabetes care, but are not sure which certification is right for you and how to get started?
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Webinar Topics
- Discuss the similarities and differences between the CDCES and BC-ADM credentials
- CDCES or certified diabetes care and education specialist
- BC-ADM or board certification in advanced diabetes management
- List the academic and experiential qualifications to take both exams
- Explore which certification best match your personal and professional goals
- Describe the steps to study and prepare for exam success for both certifications
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Euglycemic ketosis – How to best detect?

For last week’s practice question, we quizzed participants on how to best detect euglycemic ketosis. 53% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
According to recent research by the ADA/EASD, about 10% of people admitted to the hospital in diabetes crisis have euglycemic diabetes ketoacidosis.
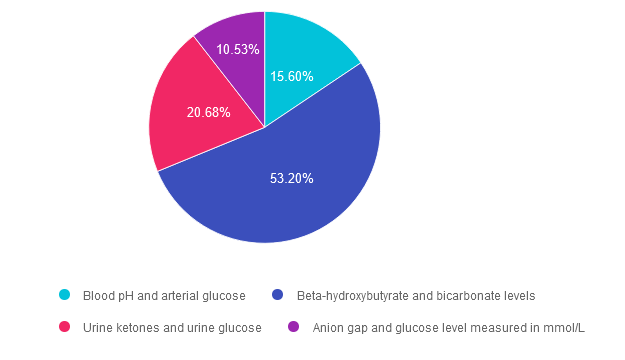
Since blood sugars are at normal levels or only slightly elevated, which of the following lab tests most accurately evaluate for euglycemic ketosis?
Answer Choices:
- Blood pH and arterial glucose.
- Beta-hydroxybutyrate and bicarbonate levels.
- Urine ketones and urine glucose.
- Anion gap and glucose level measured in mmol/L.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 15.60% chose this answer. “Blood pH and arterial glucose.” Since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL, checking arterial glucose levels won’t provide additional clarity on diagnosis. However, checking pH levels is recommended, since a pH less than 7.3 is a clear clinical indication of ketosis.
Answer 2 is correct. 53.20% of you chose this answer. “Beta-hydroxybutyrate and bicarbonate levels.” YES, this is the best answer. Beta-hydroxybutyrate evaluation with a low cutoff equal to or greater than 3.0 mmol/L, whether by lab or point-of-care-testing, is one of the most accurate measurements to evaluate if a person is in ketosis. Bicarbonate level concentration < 18 mmol/L also helps to provide confirmation of ketosis. Ketoacidosis in diabetes is due to inadequate circulating insulin, so the body switches to burning fat for fuel (instead of glucose), which leads to a build up of ketones or ketosis.
Answer 3 is incorrect. About 20.68% of respondents chose this. “Urine ketones and urine glucose.” Urine ketone testing can be used if Beta-hydroxybutyrate evaluation is not available. A urine ketone strip value of 2+ or greater indicates ketosis. However, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
Finally, Answer 4 is incorrect. 10.53% chose this answer. “Anion gap and glucose level measured in mmol/L.” he anion gap has long been a clinical measure of acidosis; however it is not considered to be a key indicator in the new guidelines. Metabolic acidosis is now defined as a pH < 7.3 and a bicarbonate concentration < 18 mmol/L. The anion gap can still be used in settings where ketone testing is unavailable. In addition, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this question?
Join our Annual Webinar
Airs live February 1, 2024 at 11:30 am PT
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Question of the Week | What is the difference between CDCES vs. BC-ADM?
What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
- A bachelor’s degree or higher is required to obtain a CDCES.
- BC-ADMs are responsible for increased complexity in decision making.
- With an advanced degree, BC-ADM’s are qualified to set up an independent practice.
- The main difference is that BC-ADM’s prescribe medications based on diagnosis.
Click Here to Test your Knowledge
Want to learn more about this question?
CDCES or BC-ADM, Which Certification is Right for Me?
Airs live on December 13th, 2023, at 11:30 am PT
Topics:
- Discuss the similarities and differences between the CDCES and BC-ADM credentials.
- CDCES or certified diabetes care and education specialist
- BC-ADM or board certification in advanced diabetes management
- List the academic and experiential qualifications to take both exams.
- Explore which certification best match your personal and professional goals.
- Describe the steps to study and prepare for exam success for both certifications.
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
How Much insulin to Cover for Allulose? The Answer might Surprise you.
JR lives with type 1 diabetes and is excited to eat a stack of blueberry pancakes with a new type of maple syrup sweetened with allulose. The syrup label reads that there are 28 grams of carbs in 2 Tablespoons of Zero Sugar Maple syrup. JR adds up the total carbs in the pancakes and syrup, and takes 6 units of bolus insulin (4 for the pancakes and 2 units for the syrup). Within a half hour, JR realizes their blood sugar is dropping fast and grabs some glucose tabs to treat the sudden low. Trying to figure out what went wrong, JR double confirms the nutrition in the pancakes and then takes a closer look at the Maple Syrup label.
Is the Maple Syrup to blame for the Unexpected Low Blood Sugar?
Looking at the label, JR confirms that there are 28 gm of carbs per serving of this unique maple syrup and 26 of those carb grams come from Allulose. Allulose is a low-calorie sugar that is Generally Recognized As Safe (GRAS) approved by the FDA in 2022. Allulose is considered a rare sugar found naturally in figs, raisins, wheat, maple syrup, and molasses or it can be commercially produced and added to foods. It’s roughly 70% as sweet as sugar and it tastes very similar. Allulose is hardly digested or absorbed, so it provides very few calories – approximately 0.4 calories per gram, compared with 4 calories per gram in table sugar.
Because very little of ingested allulose is absorbed, the impact on post-meal glucose levels is negligible.

Allulose labeling Can Cause Confusion for People Matching Insulin to Carbs
In 2019, US Food and Drug Administration (FDA) issued guidance, allowing food manufacturers to exclude allulose from total and added sugar counts on Nutrition and Supplement Facts labels. Like sugar alcohols and dietary fiber, allulose still counts towards total carbohydrates on the nutrition label.
The fact that allulose hardly raises blood sugar may lead people who match insulin to carbs to take more insulin than needed.
FDA Labeling Rule for allulose:
• Not included in “Total Sugars” or ”Added Sugars”
• Included in Total Carbohydrates
• Calories calculated with 0.4 kcals/gram
• Must be in the ingredient list
Take home message for People Counting Carbs for Accurate Insulin Dosing
Look on labels to see if allulose is listed under carbohydrates or included in the ingredient list. If it is, subtract allulose carbs from the total carbs to get an accurate carbohydrate measurement.
For other people, allulose may be a sweet-tasting alternative to sugar that provides few calories and doesn’t raise blood sugar.
CDCES Deluxe Prep Bundle
30+ Online Courses + Bonus Items | 50+ CEs
Beverly has custom-designed this course bundle to prepare you for your CDCES Exam. This bundle includes our CDCES Online Prep Bundle (featured above) plus the ADCES (formerly AADE) Review Guide – 6th Edition. This bundle includes Levels 1 through 3 (AKA Boot Camp), toolkits, plus the ADCES Review Guide.
Included in this bundle is:
- Level 1 focuses on the fundamentals and introduces each topic area for the exam.
- Level 2 deep dives into the ADA Standards of Care,
- Level 3 AKA Boot Camp is a more accelerated level that focuses on test simulation for finding the best answer to get you to the finish line of your study path.
- Technology Toolkit which gives information on pumps, sensors, and calculations,
- Test Taking Toolkit includes over 220 practice questions for test simulation plus a webinar where Coach Beverly provides test-taking tips based on her experience taking the certification exam six times.
- ADCES Review Guide for the Diabetes Care and Education Specialist Exam – 6th Edition – The ADCES Review Guide is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam. This book includes 475+ multiple-choice questions and strategies for preparing for and taking the exam with an answer key with rationales for all questions!
- Medication PocketCard – Our four-sided medication accordion Pocketcards were designed by Coach Beverly Thomassian to assist in clinical practice and exam preparation.
- Tote Bag
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Rationale of the Week | How much does Diabetes Cost the U.S?
For last week’s practice question, we quizzed participants on how much does Diabetes Cost the U.S? 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
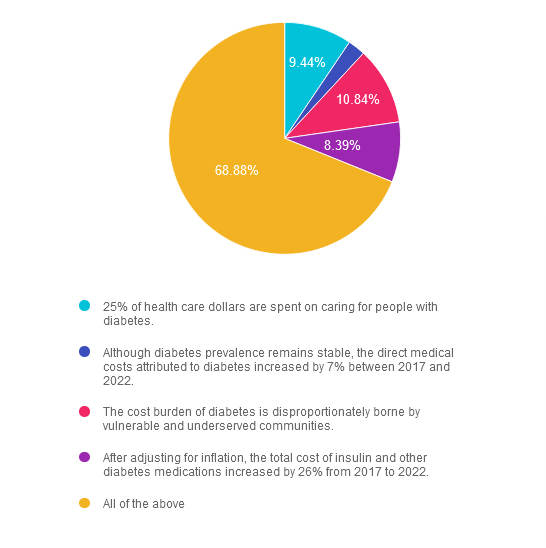
Question: According to the recently published ADA report on the 2022 Economic Costs of Diabetes in the U.S., which of the following statements is most accurate?
Answer Choices:
- 25% of health care dollars are spent on caring for people with diabetes.
- Although diabetes prevalence remains stable, the direct medical costs attributed to diabetes increased by 7% between 2017 and 2022.
- The cost burden of diabetes is disproportionately borne by vulnerable and underserved communities.
- After adjusting for inflation, the total cost of insulin and other diabetes medications increased by 26% from 2017 to 2022.
- All of the above
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 9.44% chose this answer. “25% of health care dollars are spent on caring for people with diabetes.” Yes, a quarter of all health care dollars are spent on diabetes, with the majority of money spent on hospitalizations due to cardiovascular complications and medications. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 2 is incorrect. 2.45% of you chose this answer. “Although diabetes prevalence remains stable, the direct medical costs attributed to diabetes increased by 7% between 2017 and 2022.” The cost of treating diabetes keeps increasing, putting additional financial strain on people living with diabetes. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 3 is incorrect. About 10.84% of respondents chose this. “The cost burden of diabetes is disproportionately borne by vulnerable and underserved communities.” People who earn the least amount of money and live in under-resourced areas, continue to have the highest rates of diabetes and other chronic health conditions. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 4 is incorrect. About 8.39% of respondents chose this. “After adjusting for inflation, the total cost of insulin and other diabetes medications increased by 26% from 2017 to 2022.” Yes, the cost of medications keeps increasing, which may prevent many people from accessing optimal diabetes treatment. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022
Finally, Answer 5 is correct. 68.88% chose this answer. “All of the above” YES, GREAT JOB. Most of you chose the BEST Answer. Thank you for participating in our Question of the Week. All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
Join us for our upcoming Hyperglycemic Crises, DKA & HHS Standards webinar
Airs live on December 12th, 2023, at 11:30 am PT
Topics:
- Discuss the common causes of hyperglycemic crises.
- List the differences & similarities between DKA and HHS and treatment strategies.
- Describe the causes & treatment of hyperglycemic crises.
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
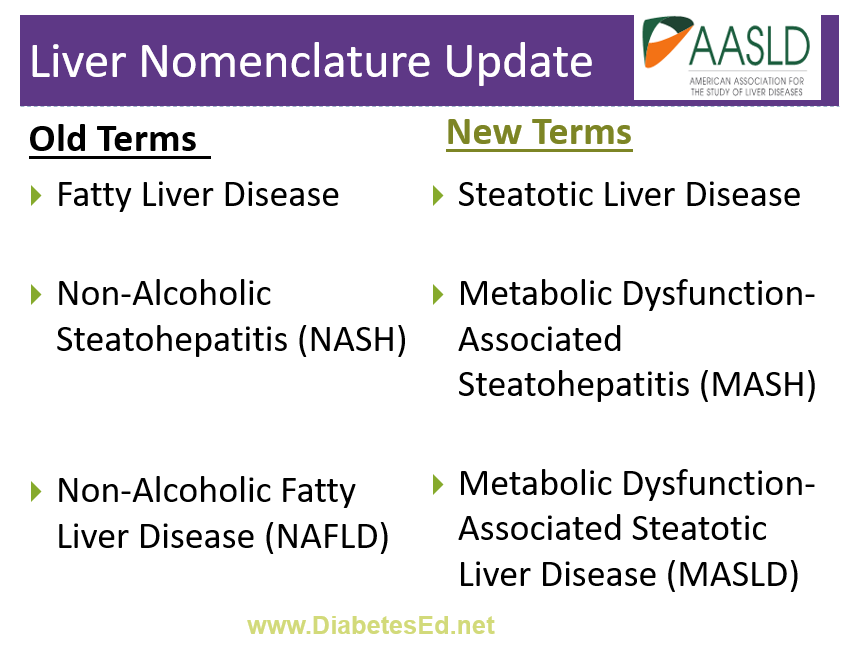
Ditch NASH and Replace with MASH
The American Association for the Study of Liver Diseases recently announced that they are updating their terms for Non-Alcoholic Steatohepatitis (NASH) and Non-Alcoholic Fatty Liver Disease (NAFLD).
Since NAFLD is considered the “hepatic manifestation of metabolic syndrome,” the organization wants the terminology to better reflect this metabolic inflammation and update the language to remove the stigma associated with the terms “fatty” and “non-alcoholic.”
According to the American Diabetes Association, NAFLD is prevalent in more than 70% of people living with diabetes. Early detection and intervention can decrease fat accumulation in the liver and lead to improved health. As diabetes care and education specialists, we can increase awareness and screenings while promoting lifestyle changes and medication therapy to save lives. One way to start the conversation is to share this updated Liver Nomenclature List with your colleagues.
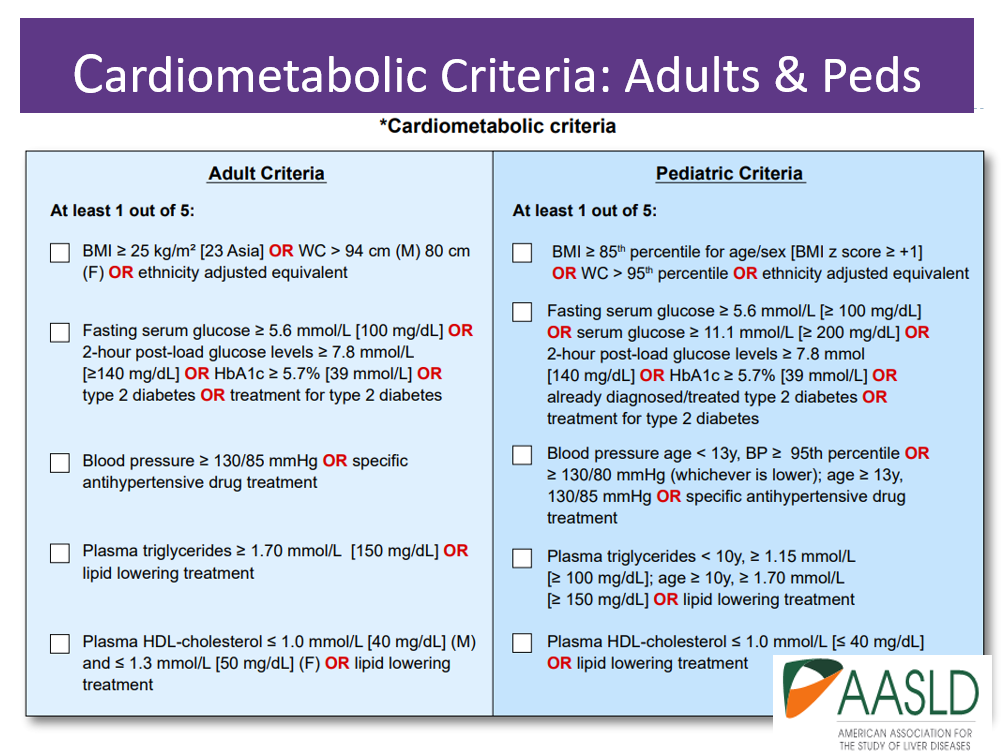
The new names, MASH and MAFLD, take into account the presence of liver disease along with cardiometabolic risk factors such as body weight, glucose levels, blood pressure, triglycerides, and HDL cholesterol levels (see CardioMetabolic table below).
Updated Liver Nomenclature List:
- Say goodbye to “Fatty Liver Disease”. The new overarching term to encompass the various presentations of liver steatosis is Steatotic Liver Disease (SLD)
- Instead of “Fatty Liver” use the term Hepatic Steatosis. This is a more technical and less stigmatizing term that simply means that the liver has an excessive amount of fat.
- The term NASH is now MASH – MASH stands for Metabolic Dysfunction-Associated Steatohepatitis. This name emphasizes that the condition is a metabolic condition not related to alcohol consumption.
- No more NAFLD. The updated term is MASLD (pronunciation: Ma-zuld), which stands for Metabolic Dysfunction-Associated Steatotic Liver Disease. This term recognizes the various risk factors beyond alcohol consumption, such as body weight, insulin resistance, and other cardiometabolic risk factors.
- The alcohol intake threshold for Alcohol-related Liver Disease ALD starts with a weekly intake of 140 g (10 drinks) for females and 210 g (15 drinks) for males.
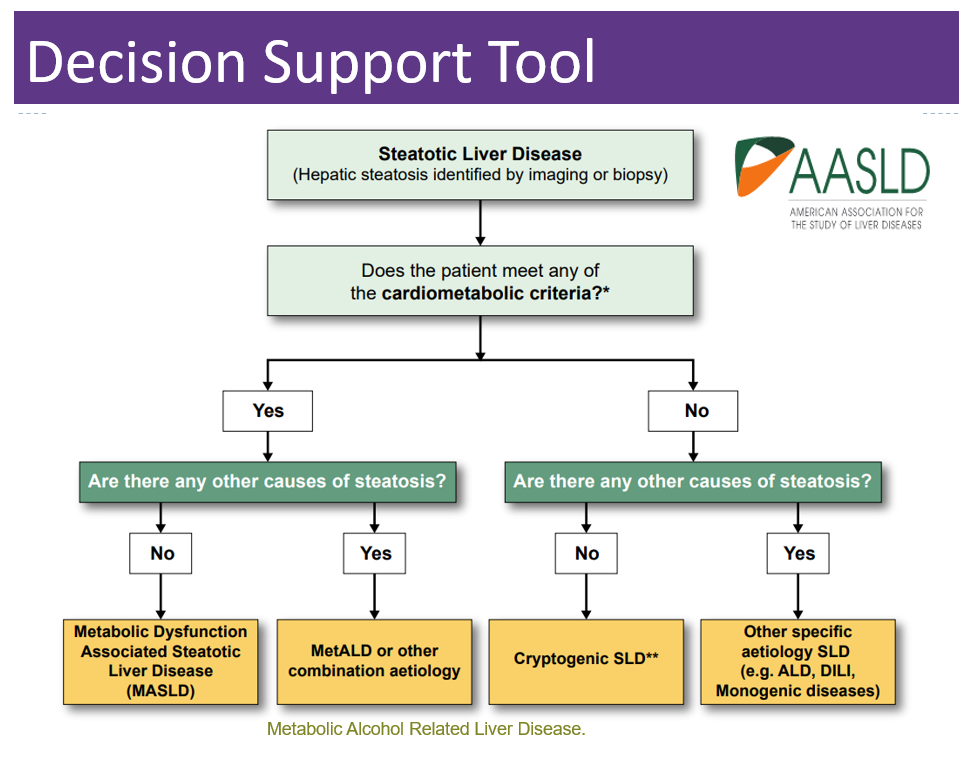
- Someone can have MASLD and it can be due to metabolic factors (MASLD) or it can be considered MetALD (pronunciation: Met A-L-D) predominant if they meet the alcohol intake threshold.
- There are other factors that can cause Steatotic Liver Disease (SLD), including drug-induced, genetic conditions and other unknown reasons (see algorithm below).
Below is a summary chart from the AADSL that reflects these important changes.
These new terms may not be universally accepted at first and the choice of name may vary by region and among healthcare professionals. Regardless of the name used, the management and understanding of the condition remain crucial to screening, identifying, and treating Steatotic Liver Disease.
Want to learn more about the GI System and Diabetes?
From the Gut to the Butt – Exploring the GI System FREE Webinar
Now Recorded & Ready to Watch
Coach Bev invites you to join this 60-minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Getting to the Gut Topics:
- From the Mouth to Intestines: Periodontal disease, Gastroparesis, Fatty liver disease, pancreas disorders
- Intestine as an Endocrine Organ & Bacterial Host
- NASH Treatment Options including lifestyle and pharmacotherapy
- State the relationship between gut health, microbiome and diabetes and inflammation
- Describe 3 strategies to get our microbiome back to better health.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.