Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App


People with diabetes experience a myriad of feelings as they utilize new technologies and try to make sense of all the data and new information. As diabetes healthcare providers, we can learn to address these feelings through person centered coaching and help individuals take steps to get to their best health. This approach not only acknowledges the individual’s feelings but also empowers them to take steps towards their optimal health.
This article equips healthcare professionals with a dozen practical coaching strategies. These strategies are designed to instill confidence in individuals with diabetes, fostering their belief in their ability to successfully self-manage their condition.

Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting a person-centered approach may require a significant adjustment for some healthcare providers. In traditional care, the provider assumes the role of the captain, steering the ship, providing the fuel, and plotting the course. However, in person-centered coaching, the provider becomes the rudder, guiding the individual while they steer their own course towards better health.
For this conversation, we imagine someone struggling with technology-related diabetes distress after switching from checking blood sugars using a meter to trying to make sense of the data being generated by their new CGM.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this:
“Taking insulin each meal is hard for you because you are worried about taking too much.” OR
“It’s hard not to constantly check your blood sugar on your CGM because you are worried that it is going above range.” OR
“It sounds like you blame yourself for having blood sugars that are above target.”
Listening and reflecting on the individual’s struggles is the first phase of energizing the visit.
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask the person who feels worried about elevated blood sugars, “I am curious to learn more about your feelings when blood sugars go above target.”
As care providers, we may be slightly overanxious to get to the “action” phase, which involves action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
Curiosity can provide comfort and open the door to insights.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers, we ask, “What are your ideas about how you can improve this situation?” Then, the provider listens carefully to what the person shares.
Along with the struggles and barriers, the individual might say,
“I will try only to check my blood sugar levels before meals and two hours after a meal instead of twenty times a day” or
“I could try adjusting my insulin dose for a week to see how that affects my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming ways to change behavior, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a tiny step by saying,
“So, you think you could limit checking your blood sugars to about eight times a day?” or
“You think you could adjust your insulin dose for a week to see if that lowers post-meal blood sugars?” Let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any prescription or declaration and stick with asking questions.
If they volunteer—”I will limit checking my blood sugars on my CGM to eight times a day.” Or
“I will adjust my insulin dose to see if it lowers my post-meal blood sugars.”
We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel we have these great ideas that will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
Let’s stop “Shoulding” on people.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
In the short term, people are usually willing to make changes when they’re terrified—when they first get diagnosed—but that willingness wanes in a relatively short period. The question is how to energize the person when the initial fear has worn off.
In conclusion, Celebrate and Recognize Each Person’s Efforts.
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they decreased their CGM checks to eight times a day or adjusted their mealtime insulin, we can say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem but will help the person feel that their effort was well spent. It will help them feel heard instead of us just “fixing it.” Over time, your empathy will build bridges and trust, leading to long-term collaboration and better health.
Download a PDF of this Person Centered Step-By-Step Approach
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about these effective communication approaches in our ReVive 5 Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont
A diagnosis of diabetes often carries a significant emotional response. A person with diabetes might report shame, fear, and guilt as they come to terms with their diagnosis and anticipate their future. As diabetes healthcare providers, we can learn to address these feelings while helping people move forward!

This cheat sheet provides a dozen simple coaching strategies for providers to help people believe in their ability to self-manage their diabetes successfully.
Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting this style of communication can be a dramatic shift for some providers. Think of it this way: In usual care, the diabetes healthcare provider steers the boat, brings the fuel, and charts the course. Using the person-centered approach, the provider is simply the rudder, serving as a guide, and the individual steers.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle, and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this: “Taking medications is hard for you because you are not sure if they are really working.” Or, “It’s hard to eat more vegetables because you are a long-haul truck driver.” Or, “It sounds like you blame yourself for having diabetes.”
Listening and then reflecting back on the struggles of the individual is the first phase of energizing the visit.
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask, “As a truck driver, I am curious to learn more about your food choices when driving.” As care providers, we may be slightly overanxious to get to the “action” phase, which involves aspects such as action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
Curiosity can provide comfort and open the door to insights.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers we ask, “what are your ideas about how you can improve this situation?” Then the provider would listen carefully to what the person shares. Along with the struggles and barriers, the individual might say, “I could buy a veggie tray before heading out in my truck,” or “I could try taking my medication every day for a week to see how they affect my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming on ways to make behavior changes, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a very small step by saying, “So, you think you could buy a vegetable tray before heading out?” or “You think you could take your diabetes meds for a week to see if they work?” and let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any form of prescription or declaration and stick with asking questions. If the person volunteers—”I will monitor my blood sugars for a week to see if these diabetes meds work.” Or “I think I could pick up veggie trays on driving days.” We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel like we have these great ideas that we are sure will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
Let’s stop “Shoulding” on people.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
Short-term, people are usually willing to make changes when they’re terrified—when they first get diagnosed–but that wanes in a relatively short period of time. The question is how to keep the person energized when the initial fear has worn off.
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they took their medications daily or ate their vegetables, we say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem, but it helps the person feel that their effort was well-spent. It helps them feel heard instead of just “fixing it” and saying, “Okay, we’ll try a new medication.” Over time, your empathy builds bridges and trust, leading to long term collaboration and better health.
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about effective communication approaches in our ReVive 5 Diabetes Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont
You are welcome to Download Effective Person-Centered Communication Approaches Cheat Sheet to share with your colleagues.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-donts

We asked Dr. Susan Guzman (see bio below), lead trainer and clinician in the Embark Trial to share insights on providing the best care to people with diabetes. Learn more by joining our ReVive 5 Diabetes Training Program where the team shares evidence-based tools and the step-by step approach utilized in the Embark Study.
Over time, our research has shown that the best way of helping a person with diabetes is to have them define their challenges and come up with their own goals and strategies. They can learn how to become their own ‘fixers”.
Dr. Guzman

In hindsight, this sounds like the opposite of what we might have expected. With much of our focus on diabetes technology and the use of new and varied medications, all of which are important, it seems we may not be listening to what people are asking for; what their goals and targets are, how they define their problems, what the impact of diabetes on their life has been, and how they want to address these difficulties.
We clinicians are trained as “fixers” and “doers.” We see a problem and we jump to fix it – and in most cases we have the skills and knowledge to do just that. But an exclusive focus on being a “fixer” means an exclusive focus on numbers, targets and mechanisms – we often forget to acknowledge the expertise the person with diabetes brings to the table.
“Over the years of being a diabetes clinician and researcher we have learned to spend more time listening and less time “doing.”
We can get started by encouraging them to identify problems and goals on their terms that are defined by their language. We can help by adding to or modifying the direction they suggest and by providing helpful tools, techniques, and information to reach the goals that they set.
Ultimately, it is the person with diabetes who must make it all work. The key take-away is to move away from being a “fixer” and shift to becoming a “curious coach” by asking the right open-ended questions and really listening to the response.
Reinvisioning our role as a “coach” instead of a “fixer” also enables the clinician to identify the often-hidden underpinnings of barriers and the problematic emotional narratives that drive management difficulties – like feeling like a failure, pounding oneself with self-blame, believing that their glucose levels are unmanageable, feeling like a burden on their family, and feeling hopeless.
How can we expect people to make goals and effectively engage in the complex daily management of diabetes when they are experiencing these burdensome feelings and thoughts?
By addressing concerns and helping with the specifics of diabetes management problems while seeing the whole person in their life context (person-centered care), we can help people with diabetes discover that they are truly their own best fixer.
Listen to Susan address a new innovative approach to diabetes distress by joining our ReVive 5 Program.
ReVive 5 Diabetes Training Program Expert Faculty
Susan Guzman, PhD is passionate about helping to change the conversations in diabetes away from shame, blame and judgment to those based on facts, empathy, and engagement. She has been part of a joint ADA/ADCES effort to address problematic language and messages in diabetes.
Dr. Guzman is a clinical psychologist specializing in diabetes. In 2003, Dr. Guzman co-founded the Behavioral Diabetes Institute (BDI), the first non-profit organization devoted to the emotional and behavioral aspects of living with diabetes.
At BDI, she serves as the Director of Clinical Education, developing and leading programs for people with diabetes and healthcare professionals. She has helped develop and facilitates diabetes distress group interventions for two NIH-funded research studies for adults with type 1 diabetes.
A diagnosis of diabetes often carries a significant emotional response. People with diabetes experience a myriad of feelings as they come to terms with their diagnosis and anticipate their future. As diabetes healthcare providers, we can learn to address these feelings through person centered coaching and help individuals take steps to get to their best health.
This Coaching Cheat Sheet provides a dozen simple coaching strategies for providers to help people believe in their ability to self-manage their diabetes successfully.

Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting this style of communication can be a dramatic shift for some providers. Think of it this way: In usual care, the diabetes healthcare provider steers the boat, brings the fuel, and charts the course. Using the person-centered approach, the provider is simply the rudder, serving as a guide, and the individual steers.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle, and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this: “Taking medications is hard for you because you are not sure if they are really working.” Or, “It’s hard to eat more vegetables because you are a long-haul truck driver.” Or, “It sounds like you blame yourself for having diabetes.”
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask, “As a truck driver, I am curious to learn more about your food choices when driving.” As care providers, we may be slightly overanxious to get to the “action” phase, which involves aspects such as action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers we ask, “what are your ideas about how you can improve this situation?” Then the provider would listen carefully to what the person shares. Along with the struggles and barriers, the individual might say, “I could buy a veggie tray before heading out in my truck,” or “I could try taking my medication every day for a week to see how they affect my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming on ways to make behavior changes, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a very small step by saying, “So, you think you could buy a vegetable tray before heading out?” or “You think you could take your diabetes meds for a week to see if they work?” and let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any form of prescription or declaration and stick with asking questions. If the person volunteers—”I will monitor my blood sugars for a week to see if these diabetes meds work.” Or “I think I could pick up veggie trays on driving days.” We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel like we have these great ideas that we are sure will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
Short-term, people are usually willing to make changes when they’re terrified—when they first get diagnosed–but that wanes in a relatively short period of time. The question is how to keep the person energized when the initial fear has worn off.
In Conclusion: Celebrate and Recognize Each Person’s Effort
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they took their medications daily or ate their vegetables, we say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem, but it helps the person feel that their effort was well-spent. It helps them feel heard instead of just “fixing it” and saying, “Okay, we’ll try a new medication.” Over time, your empathy builds bridges and trust, leading to long term collaboration and better health.
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about effective communication approaches in our ReVive 5 Diabetes Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont
You are welcome to Download Effective Person-Centered Communication Approaches Cheat Sheet to share with your colleagues.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-donts
 By Christine Craig, MS, RD, CDCES
By Christine Craig, MS, RD, CDCES
As more and more people are using glucose sensors as a tool to improve their blood sugars, they may feel frustrated or confused about the mismatch between their sensor and glucose meter readings. Some many even ditch this new fangled sensor, thinking that their old friend, the meter, provides more reliable information.
AW called the clinic to report an issue with the accuracy of their continuous glucose monitor (CGM). They stated that their blood glucose (BG) and sensor glucose (SG) have been 60-100 points different for the past 24 hours. They are concerned about this difference and want help troubleshooting what could have gone wrong.
In this article, Christine Craig, MS, RD, CDCES outlines strategies to explore this glucose mismatch and provides practical problem solving actions to clear up the confusion. In addition, we invite you to download a CGM Troubleshooting Cheat Sheet that provides specific information on different interfering substances and other factors that can affect the accuracy of continuous glucose monitor (CGM).
Assessment of accuracy within CGM or flash glucose monitors in studies uses mean average relative difference or MARD. (For simplification, we will refer to both as CGM or sensor for the remainder of this article). CGM values, also called sensor glucose values, are compared with a standard reference, often the lab-measured Yellow Springs Instrument (YSI) analyzer, and are reported as a percent of the mean or median absolute error between CGM and reference values.
Almost 20 years ago, the MARD values for CGM were about 20%, and now most CGMs have MARD values near or under 10%.1
As CGM accuracy improves, we now see non-adjunctive indications for many CGMs on the market. This term means the FDA has approved the use of CGM for treatment decisions without BG confirmation. In studies, we can see MARD differences within specific populations, in different CGM site placements, or between different sensor glucose values. For example, a sensor glucose range between 70 and 180 may have a different MARD than a sensor glucose range of less than 54 mg/dl.
As an individual living with diabetes in the real world, MARD can be impacted by factors specific to the sensor or factors of daily living. Day of sensor wear, sensor-to-sensor variation, or insertion factors such as body site selection, skin integrity (thin or loose skin), scar tissue, or body movements can impact sensor glucose accuracy. 2
If the sensor is compressed due to positioning, lack of perfusion to the sensor site can cause the sensor glucose to be temporally lower than actual glucose values.3 In this case, during CGM data interpretation, you may see a fall and then a return of trend within the sensor glucose readings. Often, compression lows occur overnight due to sleeping directly on the sensor, but during the day, compression can occur with other situations such as placement around a beltline, other very tight clothing restrictions, or if positioned within the interior of the upper arm.
In studies, body site selection between arm, abdomen, and buttocks has shown differences in accuracy, and in the real world, for each individual, this actual difference can be more significant than for others. Using recommended site selection can improve sensor accuracy, but it is essential to consider each individual living with diabetes to determine the best placement for optimal sensor accuracy.
A blood glucose meter measures capillary blood glucose, and CGM sensors measure interstitial fluid, a thin layer of fluid surrounding the cells just below the skin. These values correlate well, but they measure two different types of fluids.
This difference in BG vs. SG at one point in time can be alarming at first and is a commonly reported concern related to sensor accuracy. Education about the difference in measure and understanding that this difference is most significant during rates of change (a rise or fall in glucose values) can help address this concern. Blood glucose values change first, followed by sensor glucose.
The lag time between BG and interstitial glucose (what the sensor measures) can be from 2 to 20 minutes.
We may notice this difference most during increased rates of change (such as >2 mg/dl per min) and during circumstances such as after a meal, after treating a low glucose event, during and immediately after exercise, or after taking diabetes medications that have a more rapid effect on glucose such as meal/correction insulin or sulphonylurea.1
Educating about the difference between BG and SG and how to interpret glucose trends, sensor glucose trend arrows, and monitoring change over time can improve understanding.
Interfering Substances
The 2024 ADA Standards of Care recommends that for ALL people who wear CGM devices, education and assessment of potential interfering substances occur. Many of these interfering substances can be a common over-the-counter supplement or pain reliever. The effect for all reported interfering substances is a false elevation in sensor glucose versus actual blood glucose values. 4 It is cautioned that this could cause missing a severe glucose event.
Each manufacturer has different identified interfering substances.
Studies and reports of interfering substances are not comprehensive, so it is recommended that if suspicion occurs that a medication or supplement is contributing to erroneous CGM values, they should contact the manufacturer’s technical support team.9
For sensors requiring calibration, poor quality of the blood glucose test can also create inaccuracies with the glucose sensor readings. Most manufacturers with CGM calibration requirements recommend ensuring a “clean calibration,” having individuals wash their hands, taking the second drop of blood when hand washing is unavailable, and calibrating when glucose values are more stable, such as before a meal, insulin, or exercise. Luckily, most devices no longer require calibration, but it is important to review technique when applicable.
AW reported no recent changes with medications, supplement intake, or fortified food sources, and no changes were noted at the sensor site. However, they did report that the CGM was on the last day of manufacturer recommended sensor wear. Sensor integrity variation based on day of sensor was determined to be the main consideration of cause. After changing to a new sensor, AW’s general range of BG to SB differences were observed. This event served as an important reminder to AW to check BG when SG values were not reading as expected and different than any symptoms.
As educators, we can support individuals concerned with CGM accuracy by providing education about the differences between SG and BG values. Assessing individual factors such as medical conditions, movement and activity, site integrity and placement, issues of compression, and medication and supplement use (assessing for potential inferring substances). We can educate individuals to check BG anytime symptoms do not match SG readings and report any concern of a faulty sensor to the manufacturer. Reporting can often lead to the replacement of faulty sensor.
Since the arrival of CGM, benefits including improved quality of life factors, A1c reduction, increased Time in Range, and prevention of hypoglycemia have been found.4 We know from working in diabetes care and through real-world studies the overall value of CGMs. Unlike BG, CGMs provide a complete picture showing trends for direction, personalized alerts, and supporting pattern recognition.
Although not ideal for all, growth of users will continue to rise with approval of over-the-counter product options and understanding accuracy issues is essential to ensure safety and support user experience.


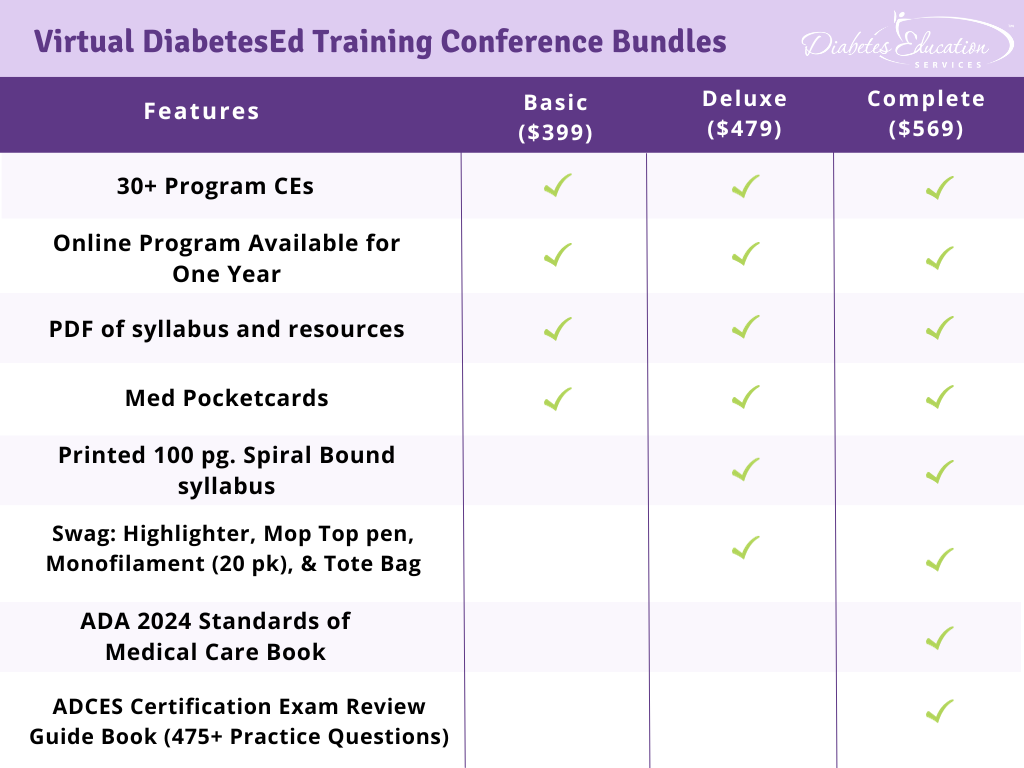
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
Registration Options