
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

We celebrate love in February, which is central to diabetes care and education. We open our hearts as we carefully listen to people share their stories about living with diabetes. We celebrate successes and grieve losses alongside the individuals we serve every day. We speak our hearts when we advocate for evidence-based care that enhances well-being and improves outcomes.
In recognition of these daily contributions of diabetes care and education specialists, we are excited to announce our “Spreading the Love” Sale during the week of Valentine’s Day. Enjoy 15% off all our online courses, including program extensions.
This month’s newsletter includes a breaking post on the most significant change to the CDCES Exam in the past 30 years (besides moving to computer testing from scantrons). We also explore how chronotype can impact glucose levels and disease risk.
As our company continues to flourish, we have expanded our team to maintain top-tier customer service. We are delighted to introduce our new customer advocate, Brent McMenomey. If you call in, you might catch his cheerful voice on the other end of the phone. In addition, he will be helping Bryanna answer chat questions and emails. Welcome Brent!
We provide two rationales of the month based on the ADA Standards. We decided to post these questions with the rationales to include additional insights into the new and updated guidelines.
As part of our commitment to foster inclusivity, diversity, and accessibility, we are offering FIVE “Making a Difference” Scholarships for our Virtual DiabetesEd Training Course on April 17-19th. Thank you in advance for considering applying and sharing with your colleagues.
In the next few weeks, you will notice updates on our homepage that will make navigation and finding your favorite resources easier. Plus, we will be popping in some new informational videos.
With love and appreciation,
Coach Beverly and Bryanna
Featured Articles
FREE Webinars & Resources
Upcoming Events – See the complete calendar listing

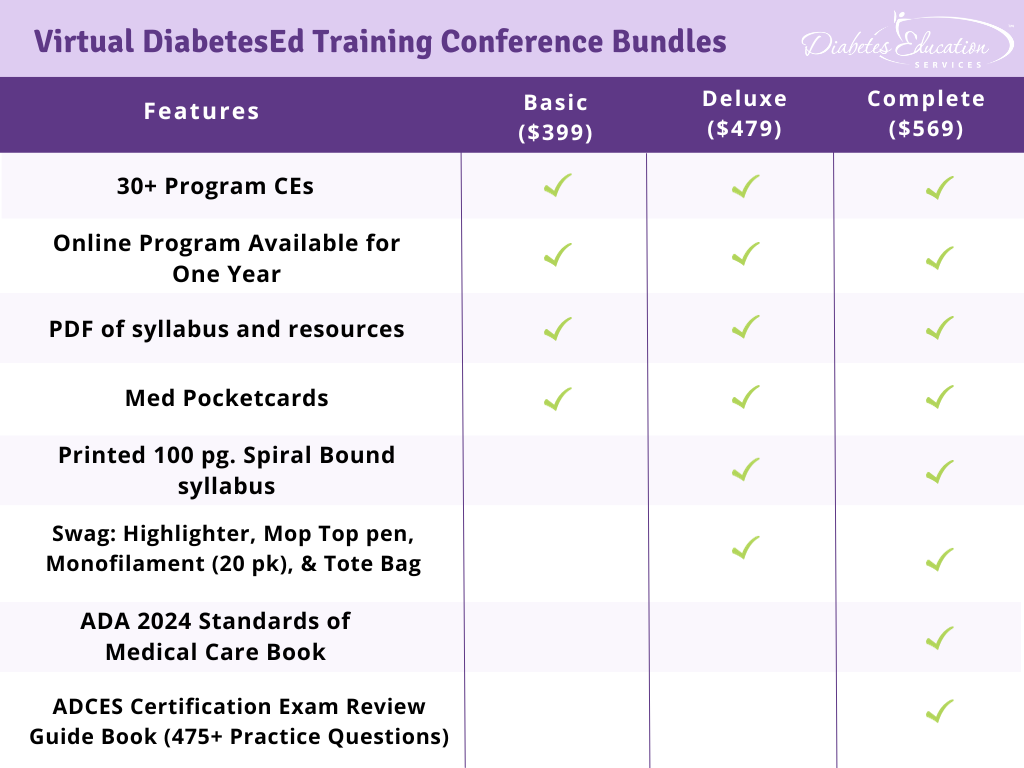
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

For last week’s practice question, we quizzed participants on the best intervention to address elevated LDL. 40% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
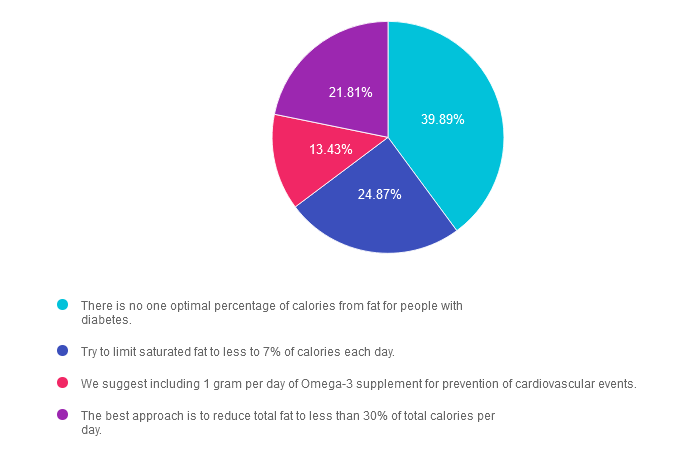
MK is 67 years old and is concerned about cardiovascular disease risk and diabetes. Their last lab result showed an A1C of 6.8%, HDL of 38 and LDL of 132. MK started reading food labels and is concerned about their total fat intake each day and wants to make diet changes to reduce CVD risk.
According to the 2024 ADA Standards of Care, which evidence-based statement is most accurate when counseling MK about their fat intake?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is correct. GREAT JOB! 39.89% chose this answer, “There is no one optimal percentage of calories from fat for people with diabetes.” The Standards of Care 2024 states, “There is no optimal percentage of calories from fat for people with diabetes or at risk for diabetes, and macronutrient distribution should be individualized.” In addition, there is no optimal percentage of calories from fat or saturated fat for people with diabetes and CVD prevention goals; however, they recommend to “limit” daily saturated fat consumption. The type of fat consumed is more important than the total amount of fat from calories.
Answer 2 is incorrect. 24.87% of you chose this answer. “Try to limit saturated fat to less to 7% of calories each day.” The standards of care do not have a recommended limit for saturated fat consumption but suggest that “people with diabetes or at risk for diabetes follow recommended guidelines for the general population.” The Dietary Guidelines for Americans 2020-2025 recommends less than 10% of calories from saturated fat. Even if considering tighter American Heart Association recommendations, they allow 5-6% of calories from saturated fat. Some eating patterns, such as the TLC diet from 2005, the DASH diet, or the Mediterranean diet, may include food choices where saturated fat is less than 7% of calories, but this is not a general population guideline.
Answer 3 is incorrect. About 13.43% of respondents chose this. “We suggest including 1 gram per day of Omega-3 supplement for prevention of cardiovascular events.” There is no recommendation for omega-3 supplementation in all persons with diabetes. Current evidence within the standard of care states that 1 gram of Omega 3 supplementation showed no benefit in preventing cardiovascular disease; however, within the REDUCE-IT trial, supplementation of pure EPA at 4 grams each day did lower cardiovascular events.
Answer 4 is incorrect. 21.81% chose this answer. “The best approach is to reduce total fat to less than 30% of total calories per day.” There is no specific recommendation for total fat amount to limit in a meal plan. The standards of care state, “The type of fat consumed is more important than the total.” They recommend following a Mediterranean-like eating pattern, which includes foods like fatty fish, nuts, and seeds and is rich in polyunsaturated and monounsaturated fats.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructors: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 15 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert.
Christine Craig, MS, RD, CDCES, winner of the 2023 Impact on Diabetes Award, is a leader in the field of nutrition, technology, and diabetes care. Her years of expertise combined with her person-centered approach and work ethic, make her a perfect speaker for this nutrition and activity focused content.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Since people with diabetes are at increased risk of fractures, the 2024 Standards have an increased focus on preventing bone fractures.
Which of the following is an accurate statement regarding diabetes and bone fractures?
Click Here to Test your Knowledge
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

For last week’s practice question, we quizzed participants on the best treatment for hospitals & heart failure. 73% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has newly discovered type 2 diabetes and is admitted to the hospital with heart failure. Their A1C is 7.9% with negative ketones and a GFR greater than 90 mg/g.
According to the 2024 ADA Standards of Care, which of the following is a recommended intervention during JR’s hospital stay?
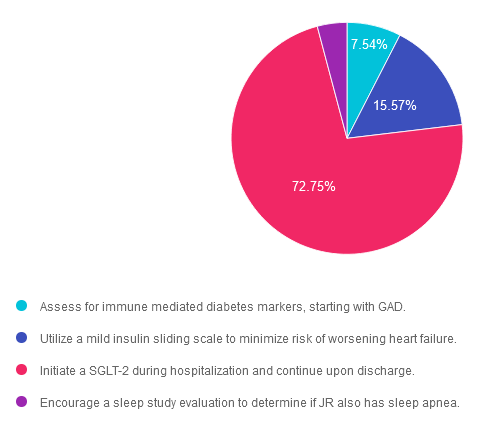
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 7.54% chose this answer. “Assess for immune mediated diabetes markers, starting with GAD.” Given that JR’s A1C is 7.9% and their ketones are negative, it seems unlikely they might have undiscovered immune mediated diabetes. The most pressing issue in addition to their diabetes is addressing the CHF.
Answer 2 is incorrect. 15.57% of you chose this answer. “Utilize a mild insulin sliding scale to minimize risk of worsening heart failure.” Based on the ADA Standards of care, insulin sliding scale as the only treatment approach is not recommended. In addition, insulin therapy doesn’t aggravate heart failure.
Answer 3 is correct. About 72.75% of respondents chose this. “Initiate a SGLT-2 during hospitalization and continue upon discharge.” YES, this is the best answer. Given that JR has diabetes and heart failure, using a SGLT-2 will lower their blood sugar plus provide a “glucoretic” effect, which will promote diuresis.
Finally, Answer 4 is incorrect. 4.14% chose this answer. “Encourage a sleep study evaluation to determine if JR also has sleep apnea.” From the information provided, there is no indication that JR is experiencing sleep apnea. The most pressing issues are the CHF and new diabetes diagnosis.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Objectives:
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
MK is 67 years old and is concerned about cardiovascular disease risk and diabetes. Their last lab result showed an A1C of 6.8%, HDL of 38 and LDL of 132. MK started reading food labels and is concerned about their total fat intake each day and wants to make diet changes to reduce CVD risk.
According to the 2024 ADA Standards of Care, which evidence-based statement is most accurate when counseling MK about their fat intake?
Click Here to Test your Knowledge
Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructors: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 15 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert.
Christine Craig, MS, RD, CDCES, winner of the 2023 Impact on Diabetes Award, is a leader in the field of nutrition, technology, and diabetes care. Her years of expertise combined with her person-centered approach and work ethic, make her a perfect speaker for this nutrition and activity focused content.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

Be a part of our diabetes community while learning about the latest in diabetes care. Plus, Coach Beverly provides an interactive question and answer session at the end of each live webinar.
Topics:
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Class Topics & Webinar Dates:
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.