
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

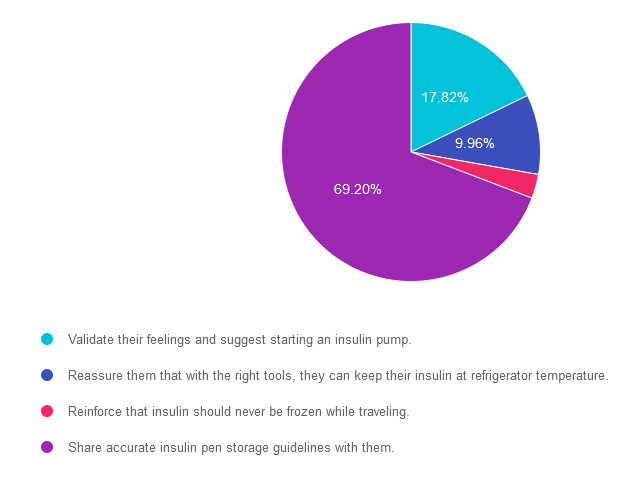
For last week’s practice question, we quizzed participants on carrying insulin. 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JL has new type 1 diabetes and their time in range is about 40%. They tell you that carrying insulin pens around on ice is such a hassle that they don’t give insulin before eating out.
What is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 17.82% chose this answer. “Validate their feelings and suggest starting an insulin pump.” Although this answer is tempting, it’s not the best answer. The first part of the answer that suggests validating their feelings is accurate. However, we would want to explore accurate insulin pen storage options before suggesting switching over to an insulin pump. Please see our insulin storage guidelines cheat sheet for more information.
Answer 2 is incorrect. 9.96% of you chose this answer. “Reassure them that with the right tools, they can keep their insulin at refrigerator temperature.” Once the person uses the insulin pen for the first time, it no longer needs to be refrigerated. Each type of insulin pen has storage guidelines for insulin kept at room temperature. Please see our insulin storage guidelines cheat sheet for more information.
Answer 3 is incorrect. About 3.01% of respondents chose this. “Reinforce that insulin should never be frozen.” It is true that insulin should never be frozen, but this is not the best answer. We also want to follow up with accurate and safe insulin pen storage information.
Finally, Answer 4 is correct. 69.20% chose this answer. “Share accurate insulin pen storage guidelines with them.” Yes, this is the best answer! Once insulin pens are used for the first time, they can be stored at room temperature. Of course, users have to avoid letting them overheat at temperatures of 86 degrees Fahrenheit or greater or getting too cold. Either situation can damage the insulin molecule. Please see our insulin storage cheat sheet for more information and feel free to share this info with colleagues and people with diabetes alike.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.

Addressing diabetes distress can be challenging, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
Susan Guzman, PhD
Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
At the recent gathering of the American Association of Clinical Endocrinology meeting, a provider shared a surprising case study of life-threatening hypoglycemia in a 33-year-old without diabetes.

Unknowingly, this individual thought they were purchasing “street Valium”, but was sold the potent sulfonylurea, glyburide, instead. As a result, their blood sugar dropped to 18 mg/dL, causing unconsciousness and the need for emergent medical assistance. This individual had purchased two unmarked, light blue pills on the street, which they thought were Valiums but turned out to be glyburide. Since sulfonylureas aren’t detected in urine toxicology screens, the symptoms of hypoglycemia may be mistakenly attributed to other causes or drugs. The only way to detect the presence of sulfonylureas is through blood tests.
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Florida, and colleagues say in a poster presented at the American Association of Clinical Endocrinology (AACE) Annual Meeting 2023.
Glyburide has a similar appearance to street valium. It is cheaper and easier to acquire than Valium (a controlled substance) which explains its appearance in illicit drug sales over the past two decades. However, since glyburide stimulates sustained insulin secretion, consumption can lead to life-threatening prolonged hypoglycemia. In addition, the person consuming it may attribute their symptoms to the “Valium” they thought they were taking and is vulnerable to severe hypoglycemia.
If hypoglycemia is detected, D50W is commonly used to immediately raise glucose levels. But, since sulfonylurea has a long half-life, blood sugars may plummet again. The most effective treatment to sustain blood sugars for those with glyburide toxicity is the administration of octreotide. Octreotide, a long-acting somatostatin agonist, reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion.
Cases like these have been reported for the past two decades. But how many incidents are we missing? Sharing this information with first responders, emergency department staff, and our communities can save lives.
Read more here

This exclusive Everything Bundle provides access to ALL of our Online University Courses and Training Programs. This bundle is perfect for those who need CEs to renew their license or diabetes certification or are looking for a comprehensive update on all topics of diabetes.
Subscribers enjoy over 40 courses taught by Coach Beverly and her team of experts on topics ranging from Diabetes Distress to MNT, Technology to Pattern Management with a focus on providing evidence-based, person-centered diabetes care.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 73 years old and has Medicare Part A and B insurance. JR completed a Diabetes Self-Management Program at a local hospital when they were in their late 60s and tells you they want to repeat the group sessions since they have forgotten much of the information.
What is the most accurate response?
Click Here to Test your Knowledge
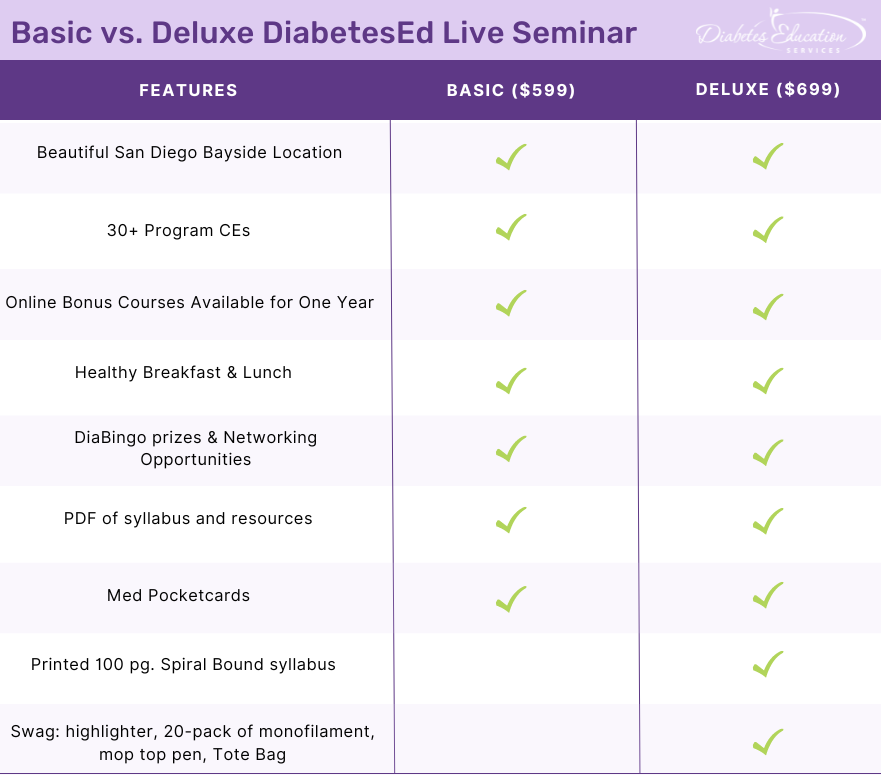
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JL has new type 1 diabetes and their time in range is about 40%. They tell you that carrying insulin pens around on ice is such a hassle that they don’t give insulin before eating out.
What is the best response?
Click Here to Test your Knowledge
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.
Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
This bundle is specifically designed for healthcare professionals who are studying for the Certified Diabetes Care and Education Specialist (CDCES) exam.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus online Technology & Test-Taking Toolkits.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
This bundle includes our Level 2, Level 3 (Boot Camp), and Level 4, plus online Technology & Test-Taking Toolkits.
This exclusive Everything Bundle provides access to ALL of our Online University Courses and Training Programs. This bundle is perfect for those who need CEs to renew their license or diabetes certification or are looking for a comprehensive update on all topics of diabetes.
Subscribers enjoy over 40 courses taught by Coach Beverly and her team of experts on topics ranging from Diabetes Distress to MNT, Technology to Pattern Management with a focus on providing evidence-based, person-centered diabetes care.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.

We love putting together our monthly newsletters. Even though they are a lot of work, they give our team a chance to share important clinical information and connect with our community of diabetes advocates and educators.
For this 25th year edition, we look at new requirements to renew your CDCES, recently approved medications for pediatrics, and the importance of emotional connection to decrease diabetes distress.
To celebrate our 25th anniversary, we are taking $100 off our most popular bundles through July. Plus, we are including a limited edition 25-year sticker in each product purchase. Keep an eye out for more swag in August too!
I am looking forward to connecting LIVE in person with you at the National ADCES meeting where I will be presenting on, “Strategies to Revitalize Your Diabetes Program.” Plus, our team is providing a LIVE three-day training program in San Diego in October.
There is nothing like being together in person to make those meaningful connections and I can’t wait.
My goal for the next decade is to keep giving back to my community. To package and share what I have learned over the past quarter of a century as an educator and CEO with all of you. I can’t think of anything more important than opening doors and sharing information with the next generation of diabetes professionals.
We encourage you to apply for our Diabetes Scholarship and challenge yourself with our Question and Rationale of the Week.
We hope you are keeping cool and we look forward to the next decade of ongoing connection.
With gratitude and appreciation,
Coach Beverly and Bryanna
Featured Articles
Upcoming Events – See the complete calendar listing
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on in-patient diabetes care. 42% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR was admitted to the hospital with an infection and newly discovered diabetes. To get glucose to ADA target range for hospitalized individuals, JR was started on 12 units of basal insulin plus bolus insulin with meals. JR experienced a morning BG of 87 mg/dL, so the provider decreased the basal insulin to 9 units. JR’s morning blood sugar the next day was 157 mg/dL.
What is the best action?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
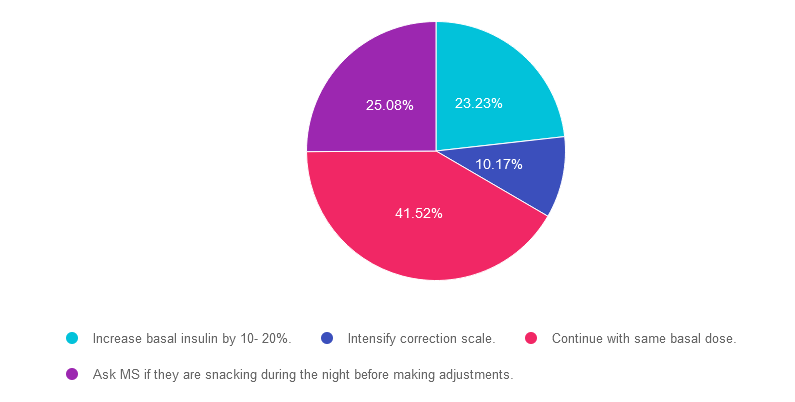
Answer 1 is incorrect. 23.23% chose this answer. “Increase basal insulin by 10- 20%.” This is a juicy answer because we typically consider the target glucose range 80-130 fasting and before meals. However, according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to increase basal insulin since JR’s morning glucose of 157 is right on target.
Answer 2 is incorrect. 10.17% of you chose this answer. “Intensify correction scale.” Another juicy answer because we typically consider the target glucose range 80-130 fasting and before meals. However, according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to intensify the correction scale since JR’s morning glucose of 157 is right on target. In addition, correction insulin doesn’t have much impact on fasting glucose. That’s the job of basal insulin.
Answer 3 is correct. About 41.52% of respondents chose this. “Continue with same basal dose.” YES, this is the BEST answer. According to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to intensify the basal insulin since JR’s morning glucose of 157 is right on target.
Finally, Answer 4 is incorrect. 25.08% chose this answer. “Ask MS if they are snacking during the night before making adjustments.” Another juicy answer. It doesn’t really matter if MS was snacking, since according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, regardless of whether or not they were snacking, JR’s morning glucose of 157 is right on target.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control & outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provide links to resources & inpatient management templates.
Objectives:
Intended Audience: A great course for healthcare professionals seeking strategies to manage and improve inpatient diabetes care.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on patient-centered care for hypoglycemia. 93% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
During your visit, you discover that MR is struggling with diabetes distress, especially around their fear of low blood sugar.
Which of the following is the most appropriate intervention?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
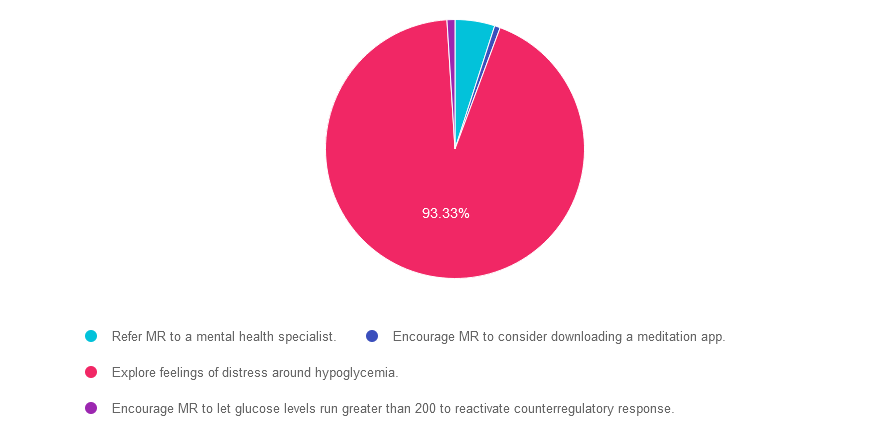
Answer 1 is incorrect. 4.69% chose this answer. “Refer MR to a mental health specialist.”
Although this answer is tempting, based on the information provided, MR doesn’t necessarily need to be referred to a mental health specialist. We expect that people with diabetes will have some degree of distress around fear of hypoglycemia. However, we can explore it further with MR and help with problem-solving to prevent hypoglycemia and make sure they have appropriate treatment strategies. If this is not successful, and MR still has on going distress, then we could consider referral to a mental health specialist with knowledge about diabetes management.
Answer 2 is incorrect. 0.71% of you chose this answer. “Encourage MR to consider downloading a meditation app.” It is true that meditation can be very helpful for people needing to decrease their stress levels. However, MR is dealing with a specific type of distress, resulting from fear of hypoglycemia. This generalized approach of suggesting a meditation app doesn’t acknowledge the distress MR is feeling specifically around hypoglycemia. Since it is not a person-centered approach, it is not the best answer.
Answer 3 is correct. About 93.33% of respondents chose this. “Explore feelings of distress around hypoglycemia.” Great job. Most of you chose this best answer! Hypoglycemia distress is real and helping people with problem-solving to prevent hypoglycemia, explore their feelings and fears, and make sure they know appropriate treatment is the best first approach. If that is not successful, referral to a mental health specialist might be indicated.
Finally, Answer 4 is incorrect. 0.99% chose this answer. “Encourage MR to let glucose levels run greater than 200 to reactivate counterregulatory response.” While it is true that people who have hypoglycemia unawareness can increase their feelings of low blood sugar by allowing their blood sugars to run a little higher, this response does not address the emotional distress MR is feeling. Plus, there is no mention that MR has hypoglycemia unawareness. For that reason, it is not the best answer.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.

Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Dates and Times for ReVive Virtual Training
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
During your visit, you discover that MR is struggling with diabetes distress, especially around their fear of low blood sugar.
Which of the following is the most appropriate intervention?
Click Here to Test your Knowledge
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.