Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Diabetes in the US: Could we be doing better?

I felt pretty discouraged reading through the New England Journal of Medicine (NEJM) summary of the state of diabetes treatment and control in the U.S. from 1999-2018. We have stalled in improving diabetes outcomes in spite of exciting new therapies and dazzling technologies.
Based on this “Diabetes Report Card” for the U.S it seems pretty clear that changes in our care delivery system are urgently needed. First, let me share the data, then we consider how Diabetes Care Specialists (you and me) can drive the improvement arrow in the right direction.
The data summarized below is extracted from the National Health and Nutrition Examination Survey (NHANES) which assesses national trends in diabetes care and outcomes for the past decade.
Summary of the major findings of the Diabetes ABC’s. A1C, Blood Pressure and Cholesterol.
Data is compared from the 2007 -2010 period to the 2015-2018 time period.
Reaching A1c Target of less than 7%?
- The percentage of people with diabetes and an A1c of less than 7%, declined from:
- 57.4% in 2007-2010 to
- 50.5% in 2015 to 2018
Coach Bev’s Report Card Comment: Blood glucose levels trended up. GRADE C-
Reaching LDL target of less than 130 mg/dL?
- The percentage of people with diabetes and an LDL of less than 130 leveled off, with slight movement in the right direction.
- 52.3% in 2007-2010 to
- 55.7% in 2015 to 2018
Coach Bev’s Report Card Comment: Lipid levels improved slightly. GRADE B-
Reaching blood pressure goal of less than 140/90 mm Hg?
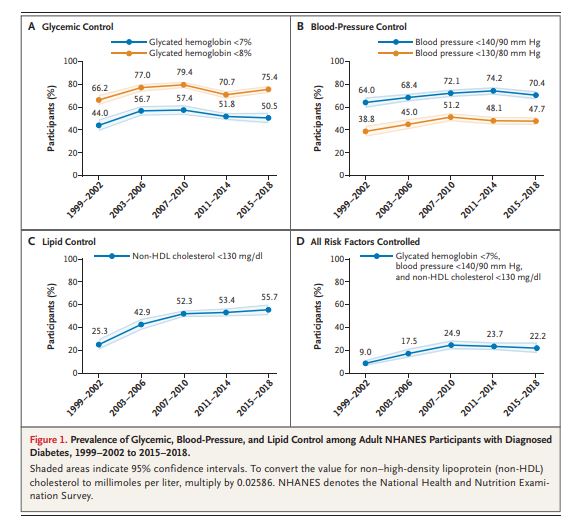
- The percentage of people with diabetes and blood pressure below the target of 140/90 worsened.
- 74.2% in 2007-2010 to
- 70.4% in 2015 to 2018
Coach Bev’s Report Card Comment: Blood pressure control achievement dropped slightly. GRADE C-
The percent of participants who achieved all 3 targets of A1C, BP, and lipids?
- The percentage of people who reached all 3 targets declined slightly.
- 24.9 % in 2007-2010 to
- 22.2% in 2015 to 2018
Coach Bev’s Report Card Comment: ABC’s of diabetes control dropped slightly. GRADE C-
Data and Graph from Trends in Diabetes Treatment and Control in U.S. Adults, 1999–2018 | NEJM
What are the barriers and how can Diabetes Care and Education Specialists help improve the grade?
The year 1999 got off to a good start with improved diabetes control but stalled and declined as the decade moved forward. There are several possible reasons as cited by the authors.
Sluggish initiation of first-line therapies. In 2015–2018, only 56.3% of adults with diabetes were using statins, 59.5% were using metformin, and 60.3% were using an ACE inhibitor or ARB.
These results are consistent with those of previous studies and point to clinical inertia as a potential culprit.
In addition, achieving glycemic and blood-pressure control often entails the use of multiple agents. However, the study found that only 60.6% of participants with an A1C level of 7% or higher and 52.8% of those with a blood pressure of 140/90 mm Hg or higher were treated with more than one glucose-lowering or blood-pressure-lowering medication, respectively.
Coach Beverly suggested action: Diabetes Care and Education Specialists can continue to raise awareness of the ADA Standards of Care for Diabetes and advocate for initiating first-line and add-on therapies in their work settings. Plus, we can encourage a streamlined referral process to facilitate participant access to DSMES and to RD/RDN for initial and ongoing lifestyle and nutrition counseling.
Care Gaps for Young People, Ethnic Groups and Uninsured Populations
The study found that younger people, Mexican Americans, and persons without health insurance were more likely to be untreated when risk-factor targets were not achieved. These gaps are especially magnified in under-resourced areas.
In addition, given that the rates of diabetes-related complications are higher in people of color and uninsured populations and that type 2 diabetes discovered in young adulthood have a more aggressive clinical course than diabetes, immediate action is required to improve outcomes.
Coach Beverly suggested action: Diabetes Care and Education Specialists continue to take a leadership role in intentional and unrelenting outreach to provide DSMES and MNT to under-resourced communities using novel and evidenced-based approaches. Since prediabetes rates are also higher in many of these communities, establishing easily accessed Diabetes Prevention Programs and networking with community health workers and leaders can contribute to improved health outcomes.
Medications are too expensive for many people
Even though we have a slew of new and highly effective classes of diabetes medications, they are out of the financial reach for many. As patents expire and the medications are available as generics, access and affordability will increase. In the meantime, a realistic approach to providing affordable diabetes treatment is needed.
Coach Beverly suggested action:
Diabetes Care and Education Specialists can help craft a medication plan that is realistic and affordable. For people with no insurance or large co-pays, consider using available generic diabetes medications. These medications often cost $10 or less for a 3-month prescription. They include: metformin, sulfonylureas, and pioglitazone. In addition, Walmart offers Reli-On insulins including Regular, NPH, and 70/30 insulin for $25 a vial. There are also online resources like GoodRx.com that help people find discounts on their usual medications and the different pharmaceutical companies also offer discount programs based on need.
See Insulin Cost Savings Guide for an abundance of resources and useful links.
In conclusion, Diabetes Care and Specialists are perfectly positioned to influence health delivery systems and advocate for best clinical practices. We can be catalysts for establishing DPP and DSMES programs in under-resourced communities and advocate for access to affordable medications and technologies to help participants reach their targets for A1C, Blood Pressure, and Cholesterol while improving quality of life.
With a concentrated effort, maybe our next report card will be a little bit better!
With hope, Coach Beverly
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
July eNews | A Radical New Approach to Diabetes Care Needed
Happy July!
Did you know that only about 50% of people in the U.S. are reaching the A1C target of less than 7%?
And only 22% of Americans reached all 3 targets for A1C, blood pressure, and lipids.
Unfortunately, the percentage of people reaching these goals has declined or stalled over the past ten years. These disappointing results are based on an analysis of the most recent data from the National Health and Nutrition Examination Survey (NHANES) published in NEJM this June.
But I have hope for several reasons!
First, Diabetes Care and Education Specialists can continue to raise awareness of the ADA Standards of Care for Diabetes and advocate for initiating first-line and add-on therapies in their work settings. Plus, we can encourage streamlining of the referral process to facilitate participant access to DSMES and to RD/RDN for initial and ongoing lifestyle and nutrition counseling. Plus, we discuss lots more ideas to improve care in the article below.
Second, I am excited to highlight our interview with a health care visionary and leader, Dr. Avni Shah, who is moving forward with a radical approach to providing diabetes care to our most vulnerable populations designed to improve outcomes.
Third, to improve care, we need more CDCES’s and taking the exam just got a little bit easier. By the end of the year, we will be able to take the CDCES exam from our home or other remote locations.
In this newsletter, we also dive into a Pediatric Question of the Week and explore Preparation for Surgery with our Rationale of the Week. We are thrilled by the interest & response to our Live San Diego Course in October and look forward to gathering together again in person.
Keep cool everyone,
Coach Beverly, Bryanna, Jackson, and Robert
Click here to read our full July 2021 newsletter.
Featured Blogs
- Diabetes Care in the US
- Interview with Dr. Avni Shah from Vayu Health – A Radical Approach to Diabetes Care
- Take Your CDCES Exam at Home?!
- Bev Renews her BC-ADM for the Fifth Time
- Question of the Week – What are Pediatric Glucose Targets?
- Rationale of the Week – How to Prep for Surgery
Upcoming Events & Resources
- DiabetesEd Course in San Diego, Oct 6-8, 2021
- ADCES Exam Desk Reference + Review Guide
- Pancreas Partner + DiaCell Teaching Tools
- Tots to Teen Webinar
- Diabetes and Pregnancy Webinar
- Free Resources Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
June eNews | DiabetesEd Scholarships & 7 Reasons for Gratitude
June eNews | DiabetesEd Scholarships & 7 Reasons for Gratitude

Happy June!
Coach Beverly is feeling grateful
For this newsletter, I am practicing my gratitude out loud and sharing it with you all.
Here are 7 things I am grateful for:
- My birthday is in early June.
- June kicks off Pride Month.
- We welcome a new team member and blog contributor, Monique Jackson.
- A new glucagon treatment is available, with updated Glucagon Cards you can download for FREE or check out on our CDCES Coach app.
- We are holding our first LIVE DiabetesEd Specialist Course in San Diego in over a year, which will include; Diabetes Flash Mob, DiaBingo, Prizes, fantastic meals, networking, laughing, and learning together.
- There are 2 scholarships available for our Diabetes Ed Live Seminar.
- Lastly, I am deeply grateful for my remarkable family, friends, my Diabetes Ed Team, all of YOU, and this opportunity to live and contribute every day.
In this newsletter, we address topics ranging from hemoglobinopathies to inclusion to new glucagon meds.
Bryanna and I had a lot of fun putting this newsletter together because it rings so true to the mission of our company; to be inclusive and welcoming, to celebrate each individual while leaving judgment behind. To lift each other up, especially during hard times. To offer hope, promote curiosity, and let you always know that we believe in you.
Happy June everyone,
Coach Beverly, Bryanna, and Jackson
Click here to read our full June 2021 newsletter.
Featured Blogs
- Theresa Garnero on Inclusive Practices for LGBTQ+ community
- African American’s at Risk for falsely low A1Cs
- Meet Monique Jackson, new blog contributor
- New Glucagon Rescue Med
- Rationale of the Week
- Question of the Week
- 2 Scholarships Available
Featured Items
- Live Seminar in San Diego
- Live Webinar Updates
- Preparing for CDCES FREE Webinar – July 8th
- Preparing for BC-ADM FREE Webinar – July 15th
- On Sale: ADA Standards of Care Book
- Free Resources Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
May Newsletter | Diabetes Ed Celebrates Nurses Week
May eNews | Diabetes Ed Celebrates Nurses Week
Happy National Nurses Day and Week!
When I was considering college as a teenager, my dad offered me some simple advice, “Why don’t you become a nurse?” I rolled my eyes and said, “Nah, I am going to be a social worker.” Four years later, I stood proudly with my white cap and nursing pin securely fastened as an RN graduate.
As I reflect on my years in this noble profession, I have witnessed the most unselfish acts of love and pure heroism by my nursing colleagues. 2020 -2021 have been rough times for the four million nurses in the United States.
Nurses have not wavered from their commitment to providing care to even the sickest among us.
Like the founder of nursing, Florence Nightingale, nurses are “Holding the Lamp” and shining it in dark places that are scary and unknown to provide comfort to those who need it most.
In this newsletter, we celebrate Nurses.
Has a nurse touched your life? Check out our blog on 5 ways you can show thanks. Did you know that in addition to founding nursing, Florence Nightingale was a statistics whiz? You can discover more about this trailblazer in the blog below.
This newsletter also offers a fresh perspective on using the plate method to encourage healthy eating while promoting the pleasure of eating.
Also, we all know that living with type 1 diabetes isn’t easy. We are hopeful that you can help us get the word out about a study geared toward not only supporting people with type 1 but providing them with excellent information and problem-solving coaching. Read more about the Embark Study below and thank you for sharing this unique opportunity with those living with type 1 diabetes.
Finally, we are excited to share an updated approach to managing diabetes in the hospital setting and encourage you to take a look at our question and rationale of the week.
Thank you nurses for the love and care you provide every day!
Coach Beverly, Bryanna, and Jackson
Click here to read our full May 2021 newsletter.
Featured Blogs
- Remembering the “Lady with the Lamp” on Nurses Week
- A Diabetes Nurse Takes a Fresh Look at the Plate Method
- Type 1 Diabetes can be Tough – Embark Can Help
- Hospital Diabetes Care Update
- Question of the Week- Type 1 & Surgery
- Rationale of the Week Mystery Condition
Featured Items
- New! Solving Glucose Mysteries for Type 1 Webinar | 1.0 CE – Recorded & Ready for Viewing!
- New! Solving Glucose Mysteries for Type 2 Webinar | 1.0 CE – May 19th
- New! Insulin Calculation Workshop | 1.0 CE – May 27th
- Preparing for CDCES FREE Webinar – July 8th
- Preparing for BC-ADM FREE Webinar – July 15th
- Free Resources Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Remembering the “Lady with the Lamp” – Happy Nurses Week
May 6th kicks off the seven-day celebration of Nurses Week and culminates on May 12th, the birthday of the founder of the field of nursing, Florence Nightingale.
Florence established the first professional training school for nurses, the Nightingale Training School at St Thomas’ Hospital in 1860. The school is now part of King’s College London. She published over 200 books, reports, and pamphlets on hospital planning and organization which are still widely read and respected today. Her most famous work is pictured above, Notes on Nursing: What It Is and What It Is Not which still offers nurses relevant content almost two centuries later.
In nursing school, Florence Nightingale‘s history was required reading. But, in my early twenties, I didn’t really grasp the significance of “the Lady with the Lamp” and her contributions until I visited the Florence Nightingale Museum in London, England.
My most meaningful experience as a tourist in London was my stop at the Florence Nightingale Museum.
Even 200 years after her birth, we are still building upon the messages and framework that Florence established. Florence had an aptitude for statistics and applied research. She quickly realized that the root of many diseases was the lack of access to clean water, decent working conditions, a safe living environment, healthy food, clean air, and sunshine. In order to improve the health of our communities, Florence campaigned to provide these most basic needs to all people.
Let us keep the light that Florence lit so long ago glowing as we honor and celebrate the over 4 million nurses in the United States.

Florence Nightingale
Florence was ahead of her time
Florence was born in 1820 in Italy Florence Nightingale. Born in an era when middle-class women were expected to simply make a good marriage and raise a family, Florence sensed a ‘calling’ from God at an early age and believed she was destined to do something greater with her life.
At the age of 33 Florence convinced her parents to attend a 3-month ‘nursing’ training and soon she became superintendent of a hospital in London.
In 1854, Florence went to Turkey with 38 other “nurses” to provide care to suffering and wounded soldiers during the Crimean War. She quickly set about organizing the hospitals to improve supplies of food, blankets, and beds, as well as the general conditions and cleanliness.
The comforting sight of her checking on the soldiers at night earned her the name ‘Lady of the Lamp’, along with the undying respect of the British soldiers.
Florence was a champion of sanitation and handwashing. She was determined to avoid the medical mistakes she witnessed during her two-year-long service at the military hospital.
As a skilled statistician, she vividly communicated the need for medical reform using detailed charts which showed that more men had died from disease than from their wounds. She then instigated a Royal Commission into the health of the army which led to a large number of improvements and saved the lives of many.
Early Public Health Advocate
Her attention later turned to the health of the British army in India. Through careful research, she demonstrated that bad drainage, contaminated water, overcrowding, and poor ventilation were causing the high death rate.
She concluded that the health of the army and the people of India had to go hand in hand and so campaigned to improve the sanitary conditions of the country as a whole.
First Nursing School
The Nightingale Training School was established in 1860 in London using donations from the Nightingale Fund. Its reputation soon spread and Nightingale nurses were requested to start new schools all over the world, including Australia, America, and Africa.
Nursing students worked long days and their dorms were often located on the hospital site. Graduates became invaluable leaders in the areas of infection control, comfort, sanitation, and improving quality of life.
The Field of Nursing has Come a Long Way
During her lifetime, Florence Nightingale witnessed the development of the nursing profession and created a standardized curriculum for the development of new nurses. Almost 200 years later, our profession has flourished and taken a leadership role in hospitals, teaching institutions, clinics, public health, military, research, and more. Nurses are four million strong, with a big vision for the future coupled with the art of caring for each individual.
Hat’s off to our Founder and Trailblazer, Florence Nightingale. Our lights keep shining bright forever.
Segments of this article were excerpted from Florence Nightingale Museum. Please feel free to enjoy their video stories and extensive information. And, if you go to London, make sure to stop by and let them know Beverly sent you!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
April eNews | Diabetes Certification Exam Updates You Need to Know
The Steps to Getting Certified Have Changed – A LOT
I remember clutching my calculator and driver’s license as I entered the crowded test site to take my Certified Diabetes Educator (CDE) Exam for the first time 29 years ago.
Back in the early 90s, applicants needed 2000 hours of diabetes self-management practice experience to qualify and a #2 pencil to bubble in the right answers on the exam scantron.
I felt queasy as I opened the test booklet and looked at the first question, which was a long vignette with a complex chart of blood sugar data. A terrifying thought crossed my mind “What if I fail, what would my staff think”?
Over 3 hours later, I gave my bubbled-in scantron to the proctor, stepped out into the sunshine, and took a big breath of relief.
Thinking back on this day, I clearly remember a lack of study tools and resources to prepare for the exam. Our little group studied the “AADE Blue Books” and created practice quizzes, but I still felt extremely unprepared for the exam in front of me.
This profound experience kick started the creation of our company, dedicated to making sure that health care professionals have the tools and resources needed to realize their professional dream of achieving (and maintaining) certification.
In truth, achieving my CDCES is one of the best and most meaningful investments in my professional career!
For this newsletter, we celebrate diabetes certification.
We dive into the modified eligibility requirements for the CDCES exam. We also provide a simplified explanation for certification renewal. Coach Beverly shares her journey to become a CDCES. Plus, we explore our most popular Question of the Week ever and pose a new question regarding Type 1 and Ramadan. To celebrate Spring, the ADA Standards Book is on sale too!
Wherever you are on this journey, we are here to cheer you on each step of the way. Let us know how we can help!
Coach Beverly, Bryanna, and Jackson
Featured Blogs
- CDCES Exam Eligibility Update
- Renewing My CDCES – What is Required?
- Coach Beverly’s Journey to Becoming a CDCES
- Question of the Week – How Many Insulin Pens?
- Rationale of the Week – Get Your Calculators
- CDCES Success Story – Congratulations Sandra!
Featured Items
- Preparing for CDCES FREE Webinar – April 1st
- Preparing for BC-ADM FREE Webinar – April 8th
- Lower Extremity Assessment Webinar – April 21st
- ADA Standards of Care Book
- Free Resources Catalog
On Sale | Now just $24.95
ADA 2021 Standards of Medical Care in Diabetes Book
The ADA Standards of Medical Care in Diabetes is a key resource for healthcare professionals involved in diabetes care, education, and support.
One of the most important pieces of literature to read prior to becoming a Diabetes Care and Education Specialist and for clinical practice, the Standards of Care book is a study must!
The book includes:
- ADA’s standards for diagnosing and treating diabetes
- Nutrition recommendations and principles
- Position statements on managing diabetes and its complications in various settings
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
March eNews | Steroids, Sugar Spikes and Nutrition Month Celebration
March | Steroids, Sugar Spikes and Nutrition Month Celebration

March is National Nutrition Month
This gives us a whole month to celebrate the amazing expertise and abundant knowledge of our nutrition colleagues.
We will be focusing on nutrition dilemmas for our Question of the Week and featuring spring recipes along with plant-based resources.
Plus, we are excited to highlight Ashley LaBrier, MS, RD, CDCES, our new dietitian team member and Virtual Conference speaker. Welcome to the team Ashley!
For our feature article, we recognize that many people with diabetes and COVID started on steroids are experiencing hyperglycemic crisis. Coach Beverly summarizes strategies to get glucose to target during steroid therapy.
We are also excited to feature an interview with Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES.
We are thrilled that Diana is providing 8 hours of content for our Virtual Conference in April. She is a pharmacology and technology expert, with a special knack for translating the complex world of diabetes technologies into understandable terms. Read more about this ADCES Educator of the Year in our interview below.
Lastly, we have expanded our FREE Webinar offerings. Coach Beverly explores the different diabetes certification options and provides test-taking skill-building. We hope you can join us!
Happy Nutrition Month everyone.
We wish you all health and an abundance of fiber intake from a variety of whole grains and fresh foods!
With affection and wishes for health,
Coach Beverly, Bryanna, and Jackson
Click here to read our full March 2021 newsletter.
Featured Blogs
- Steroids, Sugar Spikes, & Management Strategies
- Interview with Dr. Isaacs – Keynote for Virtual Conference
- Interview with Ashley LaBrier – Nutrition Expert for Virtual Conference
- Rationale of the Week
Featured Items
- FREE Webinars Ready for Viewing
- Virtual DiabetesEd Specialist Conference – from April 15th – 17th
- ADCES Exam Prep Book Bundle
- Free Resources Catalog
Virtual DiabetesEd Specialist Course
Earn 30+ CEs | April 15-17, 2021
Virtual DiabetesEd Specialist Program
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
DiabetesEd Virtual Conference Flyer 2021
Diabetes Ed Virtual 3-Day Schedule 2021
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
If you are interested in taking the CDCES or BC-ADM exam or are seeking a state of the art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need.
Can’t join live? No worries, your registration guarantees access to the recorded content through Dec 31, 2021!
Team of expert faculty includes:
- Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES – Educator of the Year, 2020
- Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
- Ashley LaBrier, MS, RD, CDCES, Diabetes Program Coordinator
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.
Bonus Courses worth 14 + CEs FREE – When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
ADCES Desk Reference + 5th Ed Review Guide Book Bundle
The 5th Edition ADCES Desk Reference & 5th Edition Review Guide Bundle –our most popular AADE Book Bundle for exam preparation!
What is included in the ADCES Book Bundle?
The Art & Science of Diabetes Self-Management Education Desk Reference – 5th Edition
Major Features:
- practical information educators can use with patients to avoid complications and comorbidities
- risks and benefits of CGM and the educator’s role in working with patients who use CGM
- updated info on incorporating the ADA, AADE, and AND joint position statement and algorithm of care into a DSME program
ADECES Review Guide for the Diabetes Care and Education Specialist Exam – 5th Edition
Includes an answer key with rationales for all questions included in the guide!
Major Features:
- 480 + multiple-choice questions
- Strategies for preparing for and taking the exam
3 self-assessment tests that cover three main content sections on the CDCES Exam:
- Assessment of Diabetes and Prediabetes
- Interventions for Diabetes and Prediabetes
- Disease Management
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
February Newsletter- 5 Myths about Exercise, Sitting & Sleep plus Winter Recipes
February – 5 Myths about Exercise, Sitting & Sleep plus Winter Recipes

New ADA Standards recognize food insecurity and its impact on mental wellness
In the first pages of the ADA 2021 Standards, there is important and detailed information addressing population health. This in-depth focus explores the Social Determinants of Health, acknowledging their impact on diabetes self-care and outcomes.
Our feature article, contributed by Bryanna, draws our attention to the mental toll associated with food insecurity. People with diabetes are at higher risk of not having enough food to eat due to socioeconomics. This is especially true for single mothers and people of color with diabetes.
We explore the social impact and provide resources that diabetes specialists can share with those who are experiencing food insecurity and distress.
In addition, I investigate some potential myths around exercise, sitting, and sleep. Are modern humans lazier and more under-slept than our ancestors? Regardless of the data, I’m not ready to give up my treadmill desk anytime soon!
February kicks off Black History Month and provides me with a perfect opportunity to recognize and celebrate a colleague that I worked with over 30 years ago. Ms. Davis made me feel proud to be a nurse and role modeled professionalism coupled with compassion.
Our rationale of the week quizzed test takers on the latest 2021 ADA Medication Algorithms and addresses a common medication management issue. See what you think.
With chilly weather blanketing much of the United States, it’s a perfect time for some recipes that not only nourish our bodies but warm us up. We’ve put together our most popular winter recipes by Dawn Desoto, RD, CDCES.
We love celebrating our DiabetesEd Online graduates. Most recently we are thrilled to congratulate Susan George for passing her BC-ADM Exam and sharing her story with us.
Lastly, this Monday, I got my second dose of the Pfizer COVID-19 vaccine at 7:30am. One hour later, I was clocking miles on my treadmill (pictured above). I did experience some chills and body aches that evening, but by the end of day 2, I felt great!
With affection and wishes for health,
Coach Beverly, Bryanna, Dawn, and Jackson
Click here to read our full February 2021 newsletter.
Most Popular 2020 Blogs
- Food Insecurity, COVID, & Mental Wellness
- 5 Myths about Exercise, Siting & Sleep, Unpacked
- Celebrating Ms. Davis and Black History Month
- Cozy Winter Recipes
- Rationale of the Week
- Celebrating Susan George passing BC-ADM Exam
Featured Items
- Level 3 – Boot Camp Updates – Starts Feb 9th
- Virtual DiabetesEd Specialist Conference – from April 15th – 17th
- Standards of Care Annual Update 2021 – Ready for On-Demand Viewing
- Level 1 Updates – Ready for On-Demand Viewing
- Free Resources Catalog
FREE Resource Catalog

- Diabetes Cheat Sheets
- Diabetes Blog Bytes
- Medication PocketCards
- Start Your Certification Journey
- CDCES Coach App
- Free Webinars hosted by Coach Beverly
- Question of the Week
See Full Free Resource Catalog
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.