Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

Author: Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
As summer arrives and the season overflows with peaches, berries, melons, cherries, and nectarines, conversations about fruit and blood sugar seem to increase alongside the abundance.
Clients often ask which fruits are “safe,” which are considered “low glycemic,” and whether certain summer fruits should be avoided altogether because of where they rank in the glycemic list.
Social media, nutrition headlines, and even dietary guidelines frequently promote low-glycemic-index dietary patterns, yet in the real world, many other factors can affect glucose response.
Originally developed in the 1980s, the glycemic index (GI) was intended to differentiate glycemic responses among foods that contained the same amount of carbohydrate. It ranks carbohydrate-containing foods by how quickly they raise blood glucose relative to a reference food, usually pure glucose or white bread. In research settings, participants consume a precise amount of carbohydrate from a single food after fasting (occasionally a mixed meal), and glucose responses are measured over time. Foods are then categorized as low GI (55 or less), moderate GI (56–69), or high GI (70 or higher).
Numerous studies have link lower-glycemic-index eating patterns with reduced diabetes risk, improved glycemic management, reduced cardiovascular risk, and better satiety. A 2021 systematic review of 29 clinical trials involving adults with type 1 and type 2 diabetes found that low glycemic eating patterns modestly improved A1c levels by 0.31% compared with higher glycemic load diets.1 The Dyslipidemia guidelines recommend improving carbohydrate quality, not just quantity, through higher-fiber, whole-grain, and lower glycemic index fruit, vegetable, and carbohydrate sources.2
A 2024 meta-analysis, which included over 100,000 participants, confirmed that low-GI dietary patterns were associated with reduced incidence of diabetes, cardiovascular disease, diabetes-related cancers, and all-cause mortality, but also noted that these protective associations were similar to those observed with increased intake of fiber and whole grains.3 This sentiment is emphasized in the 2026 ADA Standards of Care statement that a “low GI or low GL is synonymous with higher-fiber eating patterns”.4
While population-based studies indicate positive health outcomes, glycemic index tables are less reliable at the individual level and mixed outcomes have been found.4People living with pre-diabetes and diabetes can have dramatically different glucose responses to a food, depending on factors such as insulin sensitivity, sleep, stress, activity, gut microbiome composition,5 and even time of day. Ripeness, cooking method, processing, and food combinations can also alter the glycemic response. Portion of the food makes a difference. For example, watermelon is often labeled as a high-glycemic-index food, yet 1 cup of watermelon contains just 11.5 grams of carbohydrate, reducing its glycemic load.
Pairing fruit with cheese, nuts, yogurt, or other protein sources may lead to a lower glucose response; however, this outcome is not consistent across all individuals. Elimination of fruit may not be the best choice either, as summer fruits are rich in fiber, vitamins, and polyphenols and have been associated with improved glycemia when consumed as whole fruits. Jenkins et al. found that the addition of 2 servings of the study-recommended low-glycemic fruits (apples, pears, citrus fruits, berries, and stone fruits) was associated with a significant reduction in A1c, blood lipids, and blood pressure.6 However, a disconnect between the research-tested values and actual eating patterns can make GI feel impractical or overly restrictive.
Glycemic index offers a way to think about carbohydrate quality at the population level but personalization is still needed to guide individual recommendation.
Rather than teaching individuals to memorize glycemic index tables, diabetes educators may find it more effective to use glycemic index as a background concept to inform dietary change. Encourage a variety of whole summer fruits, especially berries, cherries, and stone fruits, while considering individual glycemic responses. Teach food combinations, portion awareness, carbohydrate counting, and overall carbohydrate quality as the foundation of meal planning. Use CGM and/or paired glucose testing to identify personalized glycemic responses to foods, and experiment with different food combinations to provide a more practical next step approach.
Supporting individuals in building personalized eating patterns that emphasize whole fruits, mindful portions, and recognition of individual glucose responses offers a more practical approach to the summer’s best food choices.
Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living

🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00

Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!
Every year, National Nurses Week invites us to pause and honor a profession rooted in compassion, resilience, and an unwavering commitment to care.
This Nurses Week, I encourage you to take a moment to appreciate a nursing colleague, friend or family member. Let them know how their care and compassion has made a difference in your life!
As I reflect on my 40 years as a nurse, I feel both humbled and energized by the extraordinary legacy we carry forward. Nursing is not just a career—it is a calling shaped by human connection, scientific curiosity, and the courage to show up, again and again, for people in their most vulnerable moments.

The history of nursing is rich with pioneers who transformed care through both innovation and heart. Florence Nightingale is often recognized as the founder of modern nursing, bringing sanitation and data-driven care to the forefront. But beyond her statistics and systems, she modeled something deeper—the importance of presence. That legacy continues today in every nurse who sits at the bedside, listens without judgment, and advocates fiercely for those in their care.
The observance recognizes the critical role of nurses in patient care, research, leadership, and education. It raises public awareness of the challenges nurses face, such as staffing shortages and workplace stress – and promotes professional pride and public gratitude. The ANA and partner bodies like the American Association of Critical-Care Nurses host webinars, award ceremonies, and advocacy events to spotlight the profession’s impact
Today, nurses represent the largest group of healthcare professionals specializing in diabetes. Nearly half (46%) of those who hold a CDCES credential are nurses. That’s not just a statistic—it’s a reflection of the profound impact nurses have in shaping how diabetes care is delivered, understood, and experienced every day.
In the world of diabetes care, nurses have been at the center of transformation. From the early days of checking urine glucose to administering pork and beef insulin to today’s advanced technologies, nurses have led the way. As early adopters of continuous glucose monitoring and automated insulin delivery systems, nurses have bridged the gap between complex science and real-life application. We are educators, coaches, and translators—helping people make sense of numbers, medications, and daily decisions that can feel overwhelming.
What makes diabetes nursing uniquely powerful, is the ongoing contact nurses often maintain with individuals over a lifetime. Diabetes doesn’t take a day off, and neither does the emotional weight that often accompanies it. In my work, I’ve learned that the most meaningful breakthroughs don’t come from adjusting a medication or starting a CGM, they come from creating a space where someone feels seen, heard, and supported.
Over the decades, I’ve witnessed incredible advancements in diabetes care—new medications, smarter devices, and more personalized approaches. Nurses, along with their colleagues, are often the steady thread in a fragmented healthcare system. We are the ones who notice subtle changes, ask deeper questions, and advocate when something doesn’t feel right. In diabetes care, this might mean recognizing patterns in glucose trends, addressing social determinants of health, or simply acknowledging the burnout a person feels after years of self-management. These moments matter more than we often realize.
As I reflect on my journey, from bedside nursing to education, from rural clinics to national stages – I am continually reminded that our greatest impact comes not from having all the answers, but from presence. The simple act of sitting with someone, validating their experience, and walking alongside them can be profoundly healing – for them and for us. This mutual growth is at the heart of sustainable, meaningful care.
In hospitals, clinics, schools, and beyond – you show up at every hour of the day and night, bringing skill, compassion, and unwavering dedication. You give of yourselves in ways both seen and unseen, helping others heal, receive comfort, and feel cared for in their most vulnerable moments.
National Nurses Week offers us a moment to pause and honor your service and a profession grounded in compassion, resilience, and an unwavering commitment to showing up for others. Thank YOU!
Coach Beverly, RN and author of Healing through Connection for Healthcare Professionals!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
Cardiovascular disease remains the leading cause of mortality in individuals with both type 1 and type 2 diabetes, emphasizing the importance of risk reduction.
The current Standards of Care in Diabetes from the American Diabetes Association (ADA) recommend comprehensive risk reduction through screening, pharmacologic therapy to achieve individualized blood pressure and lipid goals, and lifestyle interventions focused on diet and physical activity.
The 2026 Dyslipidemia Guideline from the American College of Cardiology and the American Heart Association (ACC/AHA), together with guidance from multiple professional societies, provides updated recommendations for assessing cardiovascular risk assessment and treatment.
Both guidelines emphasize the importance of screening (with new additions within the ACC/AHA guidelines), pharmacologic treatment for primary and secondary prevention and highlight lifestyle management to reduce atherosclerotic cardiovascular disease (ASCVD).
The 2026 ADA Standards of Care recommend individualized medical nutrition therapy (MNT) based on an individual’s eating patterns, preferences, age, comorbidities, treatment plan, and metabolic goals.1 Recommended patterns include Mediterranean-like diet, Dietary Approaches to Stop Hypertension (DASH), and plant-based approaches, all of which are associated with reduced ASCVD risk.
Key strategies include increasing plant-based proteins, reducing saturated fat (replacing it with monounsaturated and polyunsaturated fats), increasing dietary omega-3 fatty acids, increasing fiber rich carbohydrates (particularly soluble fiber), and increasing plant stanols or sterols.1 Limited research exists regarding ASCVD prevention specifically for individuals living with type 1 diabetes, so most recommendations are extrapolated from type 2 diabetes research, including dietary approaches, with implied benefit for both groups.1
The 2026 Dyslipidemia Guideline has comparative recommendations, encouraging a dietary pattern rich in fruits, vegetables, nuts, legumes, whole grains, and fiber, while reducing saturated fat and replacing it with mono and polyunsaturated fats. It noted that dietary patterns that reduce saturated fat and increase unsaturated fat was more effective than restricting dietary cholesterol.2
The guideline reinforces the cardiovascular benefits of the Mediterranean, DASH, and vegetarian eating patterns and highlights the under-recognized Portfolio dietary pattern, which was shown to lower LDL by approximately 26 mg/dL. This dietary pattern emphasizes inclusion of 50 grams of plant-based protein per day, 45 grams of nuts, at least 10 grams of viscous fiber, and 2 grams of plant sterols per day.3
Additional guidelines are given for hypertriglyceridemia depending upon level of elevation2. If triglycerides (TGs) are 150-499, added sugars are limited to 6% of calories, total fat is 30-35%, and alcohol is to be avoided. If TGs are 500-999, added sugars are limited to <5% of calories, total fat to 20-25%, and it is recommended to abstain completely from alcohol. If TGs are over 1000 mg/dl, added sugars are eliminated, total fat is limited to 10-19%, and again, alcohol abstinence is recommended.
For all groups, 150 minutes of activity is recommended, and 5-10% weight loss is considered for individuals who may benefit. Consideration of the amount, type, and quality of carbohydrates shows efficacy in lowering TGs. In addition to LDL and TG lowering, dietary patterns aim to improve overall metabolic health, including weight reduction, reduced inflammation, and improved blood pressure and glucose control.2
45% of CVD-related deaths are linked to poor diet quality4; however, the Dyslipidemia Guidelines call out the conundrum of individual variability in LDL response to dietary changes, particularly reductions in saturated fat intake2. While replacing saturated fats with foods high in monounsaturated and polyunsaturated fats is consistently associated with LDL-C reduction4, individual responses vary widely.5
These individual differences mean that two people on the same heart-healthy diet may see different LDL outcomes.

For example, some genetic variants affect how efficiently the body clears LDL particles.5 Inflammation and insulin resistance may influence dietary LDL lowering, since hyperinsulinemia impacts hepatic lipid synthesis, clearance, and LDL particle composition.6 Variations in bile acid synthesis and reabsorption also contribute, since bile acids play a key role in cholesterol homeostasis. Finally, overall dietary and other lifestyle patterns affect LDL response, highlighting the importance of comprehensive and personalized strategies.
Healthful dietary patterns reflect the synergy of the overall diet, not just a single macronutrient change.
The ADA Standard of Care and the ACC/AHA Dyslipidemia guidelines align in recommending dietary patterns based on whole foods, increased fiber intake, reduced red meat and processed meat consumption, reduced saturated fat intake, and comprehensive lifestyle interventions. However, gaps remain.
More research is needed to clarify how specific individual differences influence dietary needs, how dietary patterns affect emerging lipid markers (ApoB, endothelial function, inflammation, etc.), nutrition interventions impacting cardiovascular risk reduction for individuals with type 1 diabetes, and the long-term impact of nutrition interventions over a lifetime4.
Cardiovascular risk reduction requires team-based care, addressing not only diet but social determinants of health, activity, tobacco cessation, sleep hygiene, and pharmacotherapy to manage cholesterol, blood glucose, blood pressure, and comorbidities increasing risk. As evidence evolves, diabetes health care professionals can help translate these guidelines into practical, personalized strategies to support heart health.
Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
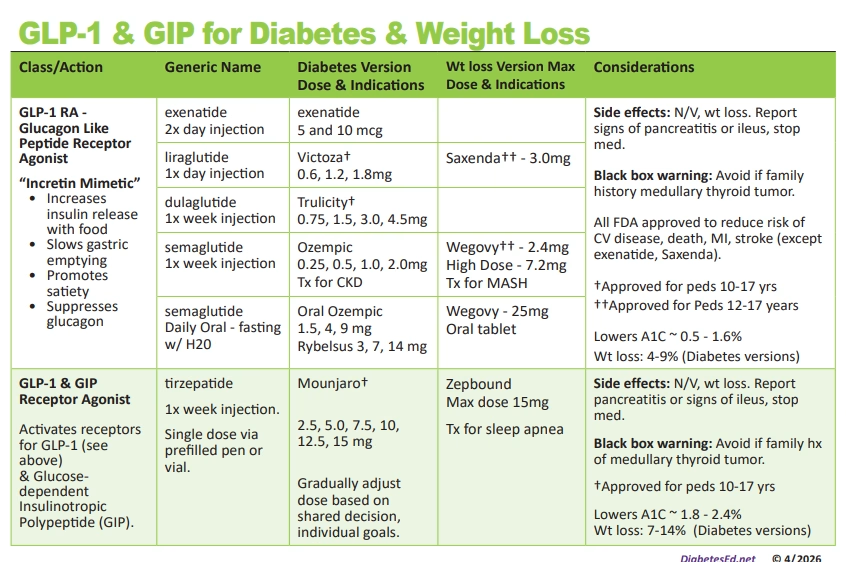
Glucagon-like peptide-1 (GLP-1) receptor agonists and GLP/GIP class of medications have seen significant advancements in the past year and 2026 promises to offer even more advancements.
The FDA granted accelerated approval in March 2026 for a high-dose (HD) injectable version of Wegovy of 7.2 mg once weekly. Until now, the highest approved dose for Wegovy—the weight loss formulation of the GLP-1 receptor agonist semaglutide—was 2.4 mg weekly.
Many individuals on the maximum 2.4 mg dose eventually reach a weight loss plateau, prompting researchers to explore whether higher dosing could extend weight reduction. Clinical trials demonstrate that increasing the dose to 7.2 mg weekly can lead to additional weight loss of up to ~20–21% from baseline, representing a meaningful advancement for those needing further support.
As expected, gastrointestinal side effects increase with higher doses, particularly, nausea, vomiting, diarrhea and early satiety. As with the other incretin medications, encourage smaller, lower fat meals that are high in nutrients. Remind individuals to keep hydrated and if the nausea persists, they may benefit from anti-nausea medications.
A major step forward in pediatric diabetes care is the recent expansion of tirzepatide (Mounjaro) into younger populations. With emerging data and regulatory progress, tirzepatide is being recognized as a potential option for youth with type 2 diabetes and extra weight, offering another powerful new tool to improve metabolic measures for young people with diabetes.
This update reflects a broader shift toward earlier, more effective interventions in youth with diabetes and elevated body weight, aligning with current guidelines that emphasize person-centered, individualized care.
A new advancement in weight management is the availability of Oral Wegovy (oral semaglutide), now with dosing options up to a maximum of 25 mg once daily. This expanded dosing offers a non-injectable alternative for individuals seeking the benefits of GLP-1–based therapy for weight management, while maintaining meaningful efficacy.
As with other oral semaglutide formulations, administration technique is critical—it should be taken on an empty stomach with a small amount of water, with no food, beverages, or other medications for at least 30 minutes to optimize absorption.
Higher-dose oral therapy may help individuals who have reached a weight plateau or who require more intensive pharmacologic support, aligning with evolving treatment strategies that prioritize person-centered care and individualized therapy.
As always, it is important to provide guidance on gradual dose escalation and management of gastrointestinal side effects, ensuring individuals are supported every step of the way.
In an effort to streamline GLP-1 therapy across formulations, Rybelsus (oral semaglutide) 1.5 mg, 4 mg, and 9 mg doses, is being rebranded as Oral Ozempic. The original Rybelsus 3, 7, and 14 doses will eventually be phased out. This naming alignment reflects the same active molecule—semaglutide—used in injectable Ozempic and Wegovy, helping reduce confusion and reinforce class familiarity among individuals and providers.
As with prior oral semaglutide formulations, proper administration remains key: it should be taken on an empty stomach with a small amount of water, with no food, beverages, or other medications for at least 30 minutes to ensure optimal absorption.
This update represents another step toward clarifying and simplifying diabetes treatment options.
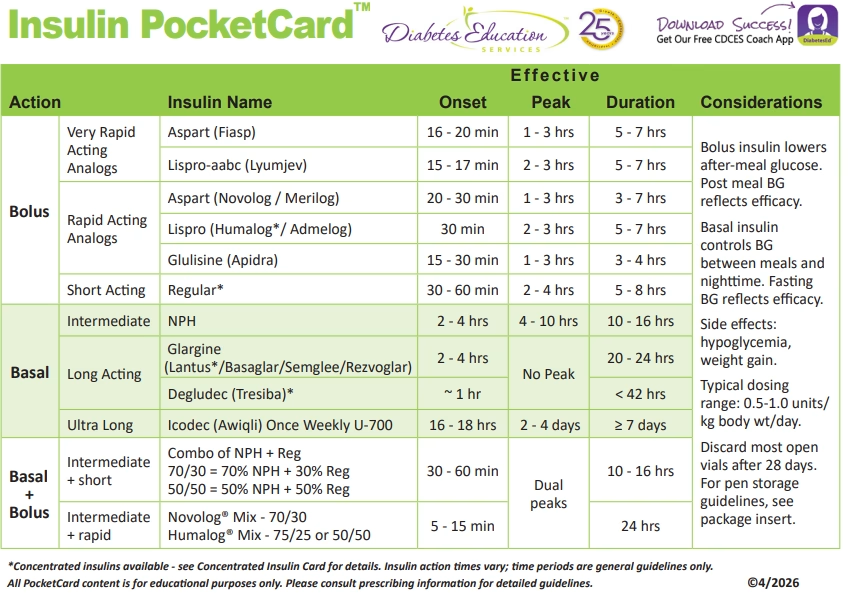
We have also updated our Insulin PocketCard to include the newly approved ultra-long-acting insulin icodec.
This once weekly insulin may be especially valuable for:
This is where your role as a healthcare professional becomes even more powerful—matching the right therapy to the right person.
We have also updated our Insulin PocketCard to include the newly approved ultra-long-acting insulin icodec.
This once weekly insulin may be especially valuable for:
This is where your role as a healthcare professional becomes even more powerful—matching the right therapy to the right person.
As healthcare professionals, staying current with these advancements allows us to:
Join us as we break down the latest in diabetes care, guidelines, and emerging therapies— you can bring confidence, clarity, and compassion to your clinical practice by joining our DiabetesEd Training Conference.
🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00
Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!
That future is no longer theoretical.
With the FDA approval of insulin icodec (Awiqli) for people with type 2 diabetes, we are entering a new era of diabetes care—one that prioritizes simplicity, adherence, and person-centered innovation.
Insulin icodec (brand name Awiqli®) is the first once-weekly basal insulin analog designed to provide steady glucose control over 7 days with a single injection.
Unlike traditional basal insulins, icodec is engineered to:
This innovation reduces injections from 365 per year to just 52, a meaningful shift for many people living with diabetes.
Insulin icodec represents a significant pharmacologic advancement as a once-weekly, ultra–long-acting basal insulin formulated at U-700 concentration (700 units/mL).
This high-concentration formulation allows delivery of a full week’s basal insulin in a single injection while maintaining a manageable injection volume.
Structurally, icodec is designed with strong, reversible albumin binding, creating a circulating depot that slowly releases insulin over approximately 7 days. It has a half-life of about one week, reaching steady state after several weekly doses, which supports consistent basal coverage with minimal peak-to-trough variability.
Because of this prolonged action, dose adjustments must be made thoughtfully, as changes take longer to fully manifest. Understanding this pharmacokinetic profile is essential to safely initiating, titrating, and educating patients about this novel therapy.
The ONWARDS Phase 3 clinical program (≈4,000 participants with type 2 diabetes) demonstrated:
For clinicians, this means:
👉 Similar outcomes
👉 With fewer injections
👉 And potentially happier patients
Download FREE Insulin PocketCard
The following recommendations based on kidney function are suggested.
The following recommendations for missed doses are suggested:
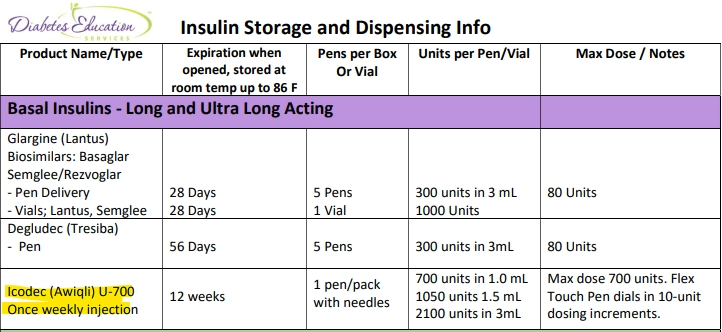
Icodec insulin is available in 3 different pen sizes and has a 12 week shelf life at room temperature. Pens can be dialed in 10 unit increments with a maximum dose of 700 units.
Download our FREE Insulin Storage and Dispensing Info Cheat Sheet below as a helpful reference.
Insulin icodec may be especially valuable for:
This is where your role as a healthcare professional becomes even more powerful—matching the right therapy to the right person.
Insulin icodec represents a transformational step forward in diabetes management. While ongoing evaluation is needed—especially regarding safety and real-world use—this therapy has the potential to reshape how we approach basal insulin. Novo Nordisk plans to launch and release the prefilled icodec (Awiqli) FlexTouch® pens in the US in the second half of 2026.
As healthcare professionals, staying current with these advancements allows us to:
Join us as we break down the latest in diabetes care, guidelines, and emerging therapies— you can bring confidence, clarity, and compassion to your clinical practice by joining our
Virtual DiabetesEd Training Conference.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.


Two out of three individuals with type 2 diabetes are affected by liver steatosis.¹ In May 2025, the American Diabetes Association (ADA) published a consensus report, which emphasized recommendations for early diagnosis, long-term monitoring, and highlighted lifestyle interventions as critical in preventing progression to cirrhosis.¹
In the past year, two medications have been approved for the treatment of MASH; however, lifestyle change remains at the foundation of treatment. These changes focus on improving dietary quality, increasing physical activity, promoting weight loss, and reducing sedentary behaviors.
Nutrition therapy, ideally guided by a registered dietitian nutritionist and reinforced by the entire diabetes care team, needs to be individualized to each person’s social, cultural, and financial needs.¹ Ivancovsky Wajcman et al. ² published a fascinating review of different country’s MASLD management guidelines summarizing recommended lifestyle interventions, their findings indicated many similarities with only a few differences.
Most groups recommended evidence-based eating patterns with the following themes:
The Mediterranean diet eating pattern is recommended in the MASLD/MASH ADA consensus report as well as the EASL–EASD–EASO Clinical Practice Guidelines ¹,²,³ due to its relationship with improving diet quality and evidence of hepatic and cardiovascular health benefits, even without weight loss.
Other dietary patterns, such as the low-fat, low-carbohydrate, Dietary Approaches to Stop Hypertension, high protein, meal replacement, and intermittent fasting, have also been shown to be comparable strategies to improve steatosis due to weight loss.¹
In people with overweight and obesity, the magnitude of weight loss has been associated with improving glycemic management, insulin sensitivity, as well as histological improvements in MASH.¹
Weight reduction over 5% has been associated with reduced steatosis, and greater weight loss of 7-10% has been shown to reverse steatohepatitis and liver fibrosis.¹,²,³ However, it is recognized that achieving long-term weight reduction may be challenging.³
Avoidance of alcohol is recommended for individuals with moderate fibrosis, as even modest use may aggravate injury.
Physical activity, including aerobic and resistance training, has independent effects beyond weight loss: decreasing intrahepatic fat, improving cardiovascular risk, improving insulin sensitivity, and supporting weight‐loss maintenance. Guidelines generally recommend greater than or equal to 150 minutes per week of moderate intensity (or equivalent) and resistance activities 2-3 times per week, with greater benefit when increasing activity.
However, reducing sedentary time and breaking up prolonged sitting bouts can be effective ways to reach this goal.¹,³ Emerging evidence highlights the importance of stress reduction, adequate sleep and treatment of sleep apnea, and management of comorbidities such as dyslipidemia and hypertension, due to their impact on liver steatosis, inflammation, and fibrosis.¹,²
Until recently, there were no FDA-approved medications specifically for MASH; treatment was either off-label or targeted at comorbidities such as weight reduction or lipid and glycemic management. However, in the past 2 years, two different medications have been released to address MASH. In March 2024, the FDA approved resmetirom (brand name Rezdiffra) for adults with noncirrhotic MASH to be prescribed in conjunction with lifestyle therapy. 4 In August 2025, the FDA approved semaglutide (brand name Wegovy) for the treatment of MASH and moderate to advanced liver fibrosis. 5
MASLD and MASH are high-risk health conditions for people with diabetes, with approximately 10-30% progressing to advanced liver disease, including cirrhosis.³ While new FDA-approved medications such as resmetirom and semaglutide offer promising options, lifestyle modification remains a cornerstone treatment.
As diabetes healthcare professionals, we are uniquely positioned to implement evidence-based strategies into the individualized care plan.
We can screen, educate, and empower individuals living with diabetes to take proactive steps that protect liver health, improve metabolic outcomes, and prevent progression to cirrhosis. Through nutrition and lifestyle therapy, pharmacotherapy, and incorporating broad strategies into DSMES services (¹) we can strengthen prevention and outcomes.
References

Explore the magnificent world of diabetes and the gut — from periodontal disease to the microbiome and everything in between.
Join Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM, for a fascinating journey through gastrointestinal health from top to bottom. This course covers fatty liver disease, gastroparesis, intestinal complications of diabetes, the gut microbiome, and more — giving you the knowledge to better support whole-body health.
Cardiovascular-kidney-metabolic (CKM) syndrome represents the interconnected systems of adiposity, metabolic dysfunction, kidney disease, and cardiovascular disease. In 2023, the American Heart Association’s (AHA) advisory panel defined a spectrum of risk by defining five progressive stages.¹ These stages span from stage 0 (no CKM risk factors), stage 1 (excess or dysfunctional adiposity), stage 2 (metabolic risk factors and CKD), stage 3 (subclinical cardiovascular disease in CKM) and Stage 4 (clinical cardiovascular disease (CVD) in CKM). This staging system emphasizes the continuum of risk, the importance of assessment across the lifespan, and the value of early interventions. The AHA advisory emphasized systematic screening (1) across all stages and lifespans to identify risk early. It is predicted that in the US, almost 90% of the population meets stage 1 or higher. (2) In collaboration with the community and medical care teams addressing CKM requires consideration of genetics, behavior, environment, and social determinants of health alongside pharmacotherapy, lifestyle and nutrition interventions. As diabetes educators, we are already skilled in assessing many of the metrics included within the staging assessments, making us well-positioned to implement CKM-based risk interventions.
In June 2025, the Journal of the American College of Cardiology published an expert review of evidence-based lifestyle interventions for CKM syndrome.² Although few studies have examined dietary interventions specifically for CKM syndrome, existing research for metabolic, kidney, and cardiovascular disease ❤️ highlights a consensus of diet quality and whole-diet patterns over single-nutrient approaches. Stage 0 encourages youth interventions to promote health through healthy diet, activity, and multi-component education within schools. In Stage 1, the goal is to prevent the development of metabolic risk factors in individuals with excess or dysfunctional adiposity. While intentional weight loss of at least 5% provides significant cardiometabolic prevention benefits, adopting a heart-healthy diet and increasing physical activity can improve health even without weight loss.¹ Stage 2 is focused on metabolic and CKD risk reduction, with DASH and Mediterranean diets recommended alongside aerobic and resistance training to support glycemic management and reduced blood pressure, hypertriglyceridemia, and progression of CKD.¹ ² Concerns of subclinical CVD modify recommendations in Stage 3 to focus on interventions that can reduce non-calcified arterial plaques and CVD events; however, only one dietary study was included within the review. The DISCO-CT trial² found that a dietitian-led DASH dietary pattern significantly reduced non-calcified plaque in individuals with non-obstructive stenosis. Nutrition should also focus on kidney preservation through individualized protein goals, increased plant-based foods 🥦, and limited processed-food consumption. In addition, medication optimization and high-intensity exercise are recommended. Dietary strategies for individuals with established CVD, Stage 4, focus on improving recovery and secondary prevention. The Mediterranean and low-fat dietary patterns are supported by evidence to reduce the recurrence of cardiovascular events post MI and reduce myocardial ischemia and coronary artery disease progression, respectively. In stage 4, like all stages, evidence-based pharmacotherapy and coordinated care with multi-disciplinary teams complement lifestyle interventions. While more research is needed to tailor strategies to individual needs at each stage, we can see that these stages have many overlapping recommendations. We can use a whole-person, comprehensive assessment approach instead of focusing on dietary interventions that treat diseases in isolation.
Dietary patterns and lifestyle strategies can be implemented using a simplified, patient-centered approach. The DASH and Mediterranean diets both support CKM syndrome outcomes but have slight differences in food patterns. DASH emphasizes fruits, vegetables, whole grains, low-fat dairy, lean protein, and limits on sodium. The Mediterranean diet prioritizes plant-based foods, healthy fats like olive oil, moderate fish and poultry, and limited red meat, with a focus on flavor and traditional eating patterns rather than strict nutrient targets. Both dietary patterns emphasize micronutrient dense, antioxidant rich and high fiber foods. By using these evidence-based dietary patterns as a framework, diabetes educators can tailor nutrition and lifestyle strategies to an individual’s preferences, abilities, and cultural context as we know is recommended by the American Diabetes Association.³ Practical considerations to address diet quality include seeking opportunities to increase vegetables and fruits, whole grains and legumes, plant proteins, fish, and nuts and seeds, while minimizing red/processed meat consumption, added sugars, sodium, and ultra-processed foods.³
Optimizing CKM health requires a comprehensive and collaborative approach.¹ This includes recognizing the impact of social determinants of health, expanding education and access to pharmacotherapies, and filling critical research gaps. It also means strengthening care coordination among providers, offering better education for both professionals and the public, and focusing on factors to address dysfunctional adiposity as a key driver of CKM. Finally, building strong partnerships across health systems and communities will be essential to support at-risk communities and help people achieve healthy outcomes. Diabetes educators can serve as guides, assisting individuals to understand their risks, supporting behavior change, and ensuring evidence-based CKM strategies are translated into practical, sustainable care.
References:

Join us live October 22nd – 23rd, 2025!
30+ CEs with Expanded Accreditation!

Join our expert team for engaging, interactive sessions that bring the ADA Standards of Care to life—covering medications, behavior change, technology, and more. Ideal for CDCES or BC-ADM exam prep, this course also includes a 4-hour Virtual Medical Nutrition Therapy Toolkit and bonus content that also meets CDCES renewal requirements.
Upon completion of this activity, participants should be able to:

Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES

Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun!
Program Faculty Disclosures:
Partners for Advancing Clinical Education (Partners) requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated according to Partners policies. Others involved in the planning of this activity have no relevant financial relationships.
Faculy Bios & Disclosures:
 Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd Services
Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd ServicesDisclosures:
Beverly Thomassian has no financial disclosures
Bio:
 Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Disclosures:
Dr. Diana Isaacs has the following relevant financial relationships:
Bio:
Diana Isaacs was awarded 2020 ADCES Diabetes Educator of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She serves in leadership roles for several pharmacies and diabetes organizations. She has numerous diabetes publications and research projects with a focus on medications, CGM and diabetes technology.
For the past three year, Dr. Isaacs has served as a contributing author for the 2023 ADA Standards of Care.
As the Program Coordinator and clinical pharmacist specialist in the Cleveland Clinic Diabetes Center, Dr. Isaacs brings a wealth of clinical knowledge combined with extensive research and speaking experience to this program.
Activity Start and End Date: 10/22/25 – 10/23/2025
Estimated time to complete the activity: 15 hours and 30 minutes
_____________________________________
Jointly provided by Partners for Advancing Clinical Education and Diabetes Education Services
![]()
![]()
Joint Accreditation Statement:
![]() In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Physician Continuing Education:
Partners designates this enduring material for a maximum of 15.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nursing Continuing Professional Development:
The maximum number of hours awarded for this Nursing Continuing Professional Development activity is 15.50 contact hours.
Pharmacy Continuing Education:
Partners designates this continuing education activity for 15.50 contact hour(s) (1.550 CEUs) of the Accreditation Council for Pharmacy Education.
(Universal Activity Number – JA4008073-9999-25-206-L01-P)
Type of Activity: Application
For Pharmacists: Upon successfully completing the activity evaluation form, transcript information will be sent to the NABP CPE Monitor Service within 4 weeks.
Dietitian Continuing Education:
This program offers 15.50 CPEUs for dietitians.
Interprofessional Continuing Education:
![]() This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
For additional information about the accreditation of this activity, please visit https://partnersed.com.

Dawn Desoto RD, CDCES, celebrates the fall and winter season with a collection of recipes that nourish and heal. Dazzle your taste-buds and energize your gut bacteria with this delicious and seasonal compilation.
Choose a pie pumpkin and wash it’s exterior. Cut in half lengthwise and remove the seeds and pulp. Roast in your oven for about 45 minutes at 350 degrees F.
Simply peel away the skin from the flesh and toss the pumpkin pulp into your food processor or blender.
Ingredients:

In a large bowl, whisk eggs and pumpkin puree together. Add the rest of the ingredients and whisk them together while slowly pouring in the evaporated milk.
Pour mixture into pie crust. Bake in the oven for 20 minutes at 390 degrees, reduce oven to 350 degrees and bake for another 45 – 60 minutes until inserted toothpick comes out clean. Store in the refrigerator overnight.

Mix the melted butter or coconut oil, walnuts, and cinnamon together and pour over the apples. Bake in the preheated oven until the apples are soft, about 20 – 30 minutes. Stir once during the baking.

Pour the wine into a small saucepan along with the orange zest and juice and all of the spices
Bring almost to a boil and add the pear halves. Turn down the heat and let the pears simmer gently for 20 – 30 minutes, or until they have slightly softened. Carefully turn the pears over a few times throughout the cooking time to ensure they color evenly. When the pears are cooked remove them from the wine and place them on plates. Add a tablespoon of yogurt to each plate and sprinkle with toasted almonds.

Combine coconut milk, oats, chia, banana, maple syrup in a pint-sized jar and stir. Top with blueberries and coconut. Cover and refrigerate overnight. Heat up and sprinkle with walnuts and cinnamon in the morning.
285 calories, 6 gm protein, 57 gms carbohydrate, 7 gms fiber 6 gm fat
To add more color into our diets, I am sharing my Spinach Pomegranate Salad recipe

Toss the spinach leaves with the rest of the ingredients. Serves 4
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.