Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Rationale of the Week | New diabetes at 13, best next step?

For last week’s practice question, we quizzed test takers on MR who was recently diagnosed with diabetes at age 13. 70% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: MR is 13 years old, and went to urgent care because they weren’t feeling well and told the Provider “I feel so tired all the time and I have to go the bathroom a lot”. The provider draws labs and gets a urine sample. The A1C is 8.7% with some ketones in the urine. The antibody results aren’t back yet. Based on the ADA Standards and this information, what is the best action?
Answer Choices:
- Start MR on basal insulin
- Order a nutrition consult ASAP and provide MR with a meter
- Initiate GLP-1 therapy to help lower glucose and A1C
- Start metformin therapy, then add exenatide XR if needed
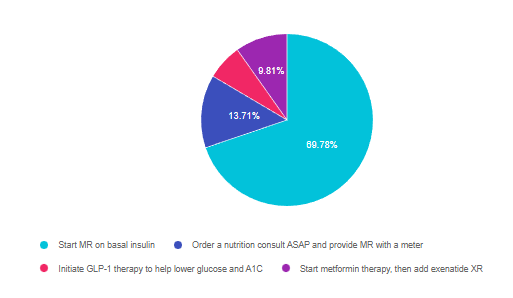
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 4, and finally 3.
Getting to the Best Answer
Answer 1 is correct. 69.78% chose this answer, “Start MR on basal insulin.” YES, GREAT JOB. This is the best answer according to ADA Standard 14 on Diabetes and Youth. If a person under the age of 18 has new-onset diabetes and an A1C of 8.5% or greater, basal insulin is needed to get blood glucose to target and stop ketosis. The next step is to determine if they have immune-mediated diabetes by evaluating their autoantibodies. If they don’t have autoantibodies (GAD, ICA, IAA), then the guidelines suggest starting metformin and gradually decreasing the insulin to see if they can be managed on metformin alone or with the addition of a GLP-1 RA. If the antibodies come back positive, MR would need to be managed on basal-bolus insulin therapy.
Answer 2 is incorrect. 13.71% of you chose this answer, “Order a nutrition consult ASAP and provide MR with a meter.” This is a juicy answer since a nutrition consult and meter are critical to managing a new diabetes diagnosis. However, we would provide the nutrition consult after we figure out what type of diabetes and after lowering blood glucose levels with insulin to prevent a hyperglycemic crisis. Regardless of the type of diabetes, ordering a meter right away and providing basic nutrition guidelines are both critical steps to keep MR safe and to evaluate treatment response.
Answer 3 is incorrect. 6.70% of respondents chose this answer, “Initiate GLP-1 therapy to help lower glucose and A1C.” Since the A1C is above 8.5%, the ADA Standards state to start basal insulin to lower glucose and prevent hyperglycemic crises. If the autoantibodies come back negative, we would start metformin therapy and consider a GLP-1 RA as a future add-on therapy.
Finally, Answer 4 is incorrect. 9.81% chose this answer, “Start metformin therapy, then add exenatide XR if needed.” Since the A1C is above 8.5%, the ADA Standards state to start basal insulin to lower glucose and prevent a hyperglycemic crisis. If the autoantibodies come back negative, we would start metformin therapy and consider a GLP-1 RA as a future add-on therapy.
Want to learn more about this question? Join us for our upcoming webinar
Test Taking Practice Exam Toolkit | FREE Webinar
Are You Ready for Exam Success?
Join us live Thursday, June 30th at 11:30 am PST

Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Two Ways to Join
Includes a review of 20 sample test questions with test-taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
From Tots to Teens | Level 2 | $29 for 1.5 CEs
Recorded & Ready to Watch!
This course includes updated goals and guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes and their families. We discuss the clinical presentation of diabetes, goals of care, and normal growth and development through the early years through adolescence. Strategies to prevent acute and long term complications are included with an emphasis on positive coping for family and child with diabetes.
Objectives:
- Discuss the goals of care for Type 1 and Type 2 Kids with Diabetes
- State Strategies to prevent acute and chronic complications
- Discuss the importance of positive psychosocial adjustment and resources
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | What is true about fatty liver disease?
For last week’s practice question, we quizzed test takers on fatty liver disease. 57% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: 45 to 75% of individuals with type 2 diabetes have non-alcoholic fatty liver disease (NAFLD). NAFLD has associated with an increased risk of steatohepatitis, cirrhosis, and liver cancer. Which of the following statements is true based on ADA Standards of Care?
Answer Choices:
- Elevated ALT and AST indicate a diagnosis of NAFLD.
- Approved treatment for NAFLD includes low-dose aspirin and pioglitazone.
- Fatty liver disease indicates that 5-10% of the liver weight is from fat.
- Surgical intervention is indicated to resect the liver in the presence of NAFLD.
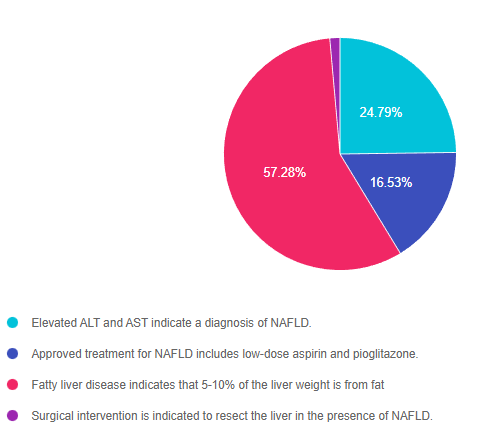
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally 4.
Getting to the Best Answer
Answer 1 is incorrect. 24.79% chose this answer, “Elevated ALT and AST indicate a diagnosis of NAFLD.” These two liver enzyme tests certainly indicate liver inflammation and are a signal that further investigation is warranted. However, to confirm and diagnose NAFLD, a comprehensive review of patient history, lab results, liver imaging studies and possibly a biopsy are required.
Answer 2 is incorrect. 16.53% of you chose this answer, “Approved treatment for NAFLD includes low-dose aspirin and pioglitazone.” The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative. There is no officially approved medication to treat NAFLD, but pioglitazone and GLP-1 RA’s appear to decrease fatty liver based on current studies.
Answer 3 is correct. 57.28% of respondents chose this answer, “Fatty liver disease indicates that 5-10% of the liver weight is from fat.” GREAT JOB, this is the best answer. The good news is that weight loss and increased activity are very effective in treating fatty liver disease. A weight loss of 7-10% linked with a 50% drop in liver fat. Every pound lost makes a big difference. The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative.
Finally, Answer 4 is incorrect. 1.41% chose this answer, “Surgical intervention is indicated to resect the liver in the presence of NAFLD.” People with NAFLD and other risk factors, have an increased risk of disease progression to cirrhosis and liver cancer, which might require surgical intervention. However, no surgical intervention is warranted for NAFLD. The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative.
Want to learn more about this question? Join us for our upcoming webinar
Test Taking Practice Exam Toolkit | FREE Webinar
Are You Ready for Exam Success?
Join us live Thursday, June 30th at 11:30 am PST
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Two Ways to Join
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Want to learn more about Diabetes Care? View our
Virtual DiabetesEd Specialist Conference
30+ CEs
Recorded & Ready to Watch!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
- Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES – Educator of the Year, 2020
- Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
- Ashley LaBrier, MS, RD, CDCES, Diabetes Program Coordinator
Virtual DiabetesEd Specialist Conference Deluxe | 30+ CEs
Deluxe Option for $449: Virtual Program includes:
- Q & A Session with the instructor after each webinar.
- LIVE Presentations by our team of experts.
- State of the art review of current diabetes care and technology.
- Resources for each session.
- Access to free podcasts and video recordings within a week of each live session for one year.
Deluxe Version includes Syllabus, Standards and Swag*:
- Diabetes Educator Course 2022 Syllabus Hard Copy – over 100 pages -This spiral-bound workbook contains the printed version of all of the instructor’s slides.
- ADA 2022 Standards of Care Book -The ADA Standards of Medical Care in Diabetes is a key resource for healthcare professionals involved in diabetes care, education, and support.
- DiabetesEd Services highlighters, Medication PocketCard, Tote Bag and Pen
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Pregnancy Surprise with Type 1 Diabetes
For last week’s practice question, we quizzed test takers on complications of hyperglycemia during pregnancy. 60% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AR has type 1 diabetes and is in shock because they just discovered they are 6 weeks pregnant. AR uses a CGM and insulin pump to manage their diabetes and their most recent A1C is 8.3%. Which of the following is a potential complication associated with hyperglycemia during the first 10 weeks of pregnancy?
Answer Choices:
- Macrosomia and post-natal jaundice
- Intrauterine hypoglycemia
- Neonatal respiratory distress
- Diabetic embryopathy
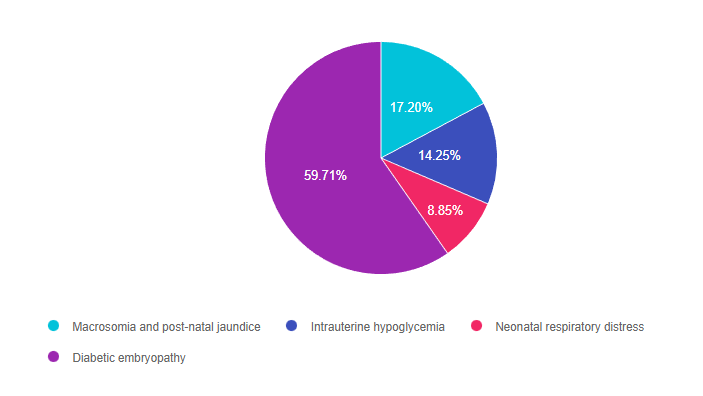
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally 3.
Getting to the Best Answer
Answer 1 is incorrect. 17.20% chose this answer, “Macrosomia and post-natal jaundice.” This is a juicy answer since macrosomia and post natal jaundice are often associated with gestational diabetes (GDM) However, this question is not asking about GDM, which is usually diagnosed between 24-28 weeks of pregnancy. In this question, AR already has type 1 when becoming pregnant and wants to know the consequence of hyperglycemia during the first 10 weeks when the fetal organs are developing.
Answer 2 is incorrect. 14.25% of you chose this answer, “Intrauterine hypoglycemia.” This answer is designed to lure the test taker in with the word hypoglycemia. A fetus who is exposed to excess glucose in utero is at risk of post natal hypoglycemia AFTER delivery, since they no longer are receiving maternal glucose and their pancreas is making abundant insulin. A fetus exposed to excess intrauterine glucose levels is at risk of hyperglycemia (not hypo).
Answer 3 is incorrect. 8.85% of respondents chose this answer, “Neonatal respiratory distress.” This is a juicy answer since neonatal respiratory distress is often associated with GDM and diabetes in pregnancy. However, this question is not asking about post delivery complications. In this question, AR already has type 1 when becoming pregnant and wants to know the consequence of hyperglycemia during the first 10 weeks when the fetal organs are developing.
Finally, Answer 4 is correct. 59.71% chose this answer, “Diabetic embryopathy.” Yes, GREAT JOB, this is the best answer. The first trimester of fetal development is when the organs are developing. A fetus exposed to excess levels of glucose during this critical time is at increased risk of congenital defects like anencephaly, microcephaly, neural tube defects and others. For people with diabetes, achieving an A1C of less than 6.5% before conceptions improves outcomes and decreases risk of congenital anomalies. With careful planning and keeping a close connection with their health care team, people with diabetes can experience healthy pregnancies and great outcomes.
Want to learn more about this question? Join us for our webinar
Pregnancy & Diabetes Standards | Level 2 | $29 for 1.5 CEs
Recorded & Ready to Watch!

Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, and understanding. This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Objectives:
- Three issues that affect pregnancy with diabetes
- The unique attributes of pre-existing diabetes in pregnancy and gestational diabetes
- Diagnostic criteria and management goals for gestational diabetes
- Potential short term and long term complications of fetal exposure to hypoglycemia
- Prevention measures to keep parent and baby healthy
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Best glucose monitoring practice in the hospital?
For last week’s practice question, we quizzed test takers on glucose monitoring in the inpatient setting. 60% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JL is a new nursing graduate and asks you questions about glucose monitoring in the inpatient setting. Which of the following statements is most accurate regarding providing diabetes care in the hospital setting?
Answer Choices:
- If a patient is experiencing morning hypoglycemia, reduce basal insulin.
- Nursing staff can use the patient’s CGM glucose results to determine insulin dose.
- Any patient admitted with a glucose of 140 mg/dl or greater, confirmed on two different occasions, needs to be started on insulin.
- Hospital point-of-care glucose meters are mostly as accurate as lab glucose results.
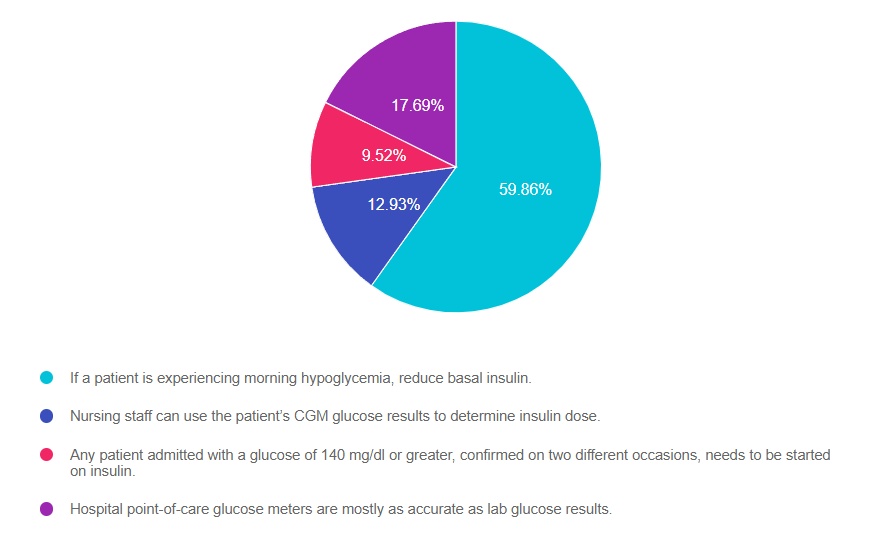
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally 3.
Getting to the Best Answer
Answer 1 is correct. 59.86% chose this answer, “If a patient is experiencing morning hypoglycemia, reduce basal insulin.” YES, GREAT JOB! During hospitalization, keeping glucose levels on target improves outcomes and decreases the length of stay. This includes preventing hypoglycemia, which can be life-threatening. The most common cause of morning hypoglycemia is basal insulin. Treating hypoglycemia rapidly with carbs and rechecking to make blood sugar is increasing is critical. However, to prevent future hypoglycemic events, determining the cause of the low blood sugar and taking corrective action is just as important. Reducing basal insulin by 20% or more when morning blood sugars are less than 100 mg/dL in the hospital setting makes a big difference in protecting against hypoglycemia.
Answer 2 is incorrect. 12.93% of you chose this answer, “Nursing staff can use the patient’s CGM glucose results to determine insulin dose.” This is a juicy answer, however, the FDA has not approved the dosing of insulin based on CGM results in the hospital setting. Inpatients with adequate cognition are allowed to use their CGM to monitor their blood sugar and keep an eye on trends based on the hospital’s policy. However, insulin dosing is based on the hospital-approved point-of-care glucose meter results.
Answer 3 is incorrect. 9.52% of respondents chose this answer, “Any patient admitted with a glucose of 140 mg/dl or greater, confirmed on two different occasions, needs to be started on insulin.” If a person is admitted with a glucose of 140 or greater, this would certainly catch our attention and require ongoing monitoring. They may have undiagnosed prediabetes or diabetes (depending on if the glucose was fasting or random). However, this glucose level of 140 does not meet the criteria to start insulin. According to the ADA Standards, insulin therapy is initiated when the admitting glucose is 180 or greater.
Finally, Answer 4 is incorrect. 17.69% chose this answer, “Hospital point-of-care glucose meters are mostly as accurate as lab glucose results.” This is another juicy answer. The lab glucose is the most accurate. Approved hospital glucose meters can read 15% higher or lower than the actual lab glucose. At home glucose meters, can be up read up to 20% higher or lower than lab glucose and still be within FDA approval parameters. For more info, see our blog, How Accurate are Glucose Meters?
Want to learn more about this question? Join us for our webinar
Hospitals & Hyperglycemia Standards | Level 2 | $29 for 1.5 CEs
Recorded & Ready to Watch!
Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control and outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest ADA Standards and provide links to resources and inpatient management templates.
Objectives:
- The impact of hyperglycemia in the hospital setting
- The importance of inpatient glucose control
- Three strategies to get glucose to the goal in the hospital setting
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Which diabetes meds safe during pregnancy?
For last week’s practice question, we quizzed test takers on pregnancy and diabetes. 63% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AR says they just found out they are pregnant. AR has type 2 diabetes and polycystic ovary syndrome and takes metformin 1000mg BID, semaglutide (Ozempic) 1.0mg weekly, and 30 units glargine insulin for diabetes management. Her most recent A1C was 8.2%. What is the most important action to take?
Answer Choices:
- Add bolus insulin to get A1C less than 6.5%.
- Increase the semaglutide (Ozempic) to 2.0mg weekly.
- Add a SGLT-2 Inhibitor to get glucose to target.
- Instruct AR to stop the semaglutide (Ozempic).
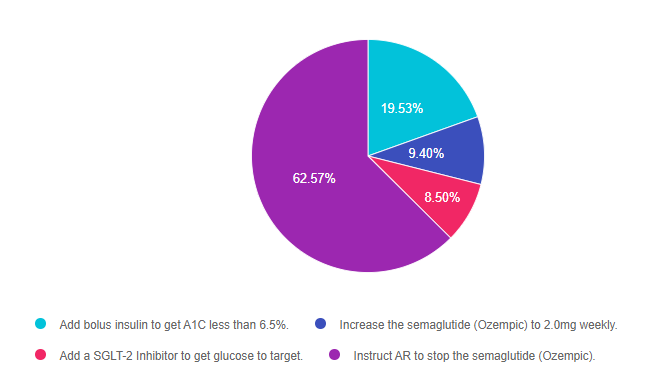
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally 3.
Getting to the Best Answer
Answer 1 is incorrect. 19.53% chose this answer, “Add bolus insulin to get A1C less than 6.5%.” This answer is accurate, but it is not the best answer. The A1C goal during pregnancy is less than 6.5% and in this case, AR will need to manage their diabetes using basal bolus insulin therapy. However, since semaglutide is not approved for pregnancy, the most important action is to stop the administration of this GLP-1 RA.
Answer 2 is incorrect. 9.40% of you chose this answer, “Increase the semaglutide (Ozempic) to 2.0mg weekly.” AR’s blood glucose levels are above the A1C pregnancy target of 6.5%, which means insulin intensification is needed. Insulin is safe during pregnancy. However, since semaglutide is not approved for pregnancy, the most important action is to stop the administration of this GLP-1 RA.
Answer 3 is incorrect. 8.50% of respondents chose this answer, “Add a SGLT-2 Inhibitor to get glucose to target.” AR’s blood glucose levels are above the A1C pregnancy target of 6.5%, which means insulin intensification is needed. Insulin is safe during pregnancy. However, SGLT-2s are not approved for pregnancy and the GLP-1 RA, semaglutide would also need to be discontinued.
Finally, Answer 4 is correct. 62.57% chose this answer, “Instruct AR to stop the semaglutide (Ozempic).” YES, GREAT JOB! AR’s blood glucose levels are above the A1C pregnancy target of 6.5%, which means insulin intensification is needed. Basal bolus insulin therapy is safe during pregnancy. However, since semaglutide is not approved for pregnancy, the most important action is to stop the administration of this GLP-1 RA. Metformin can be continued through the first trimester and the insulin would need to be intensified to get A1C to target.
Want to learn more about this question? Join us for our webinar
Pregnancy & Diabetes Standards | Level 2 | $29 for 1.5 CEs
Recorded & Ready to Watch!
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, and understanding. This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Objectives:
- Three issues that affect pregnancy with diabetes
- The unique attributes of pre-existing diabetes in pregnancy and gestational diabetes
- Diagnostic criteria and management goals for gestational diabetes
- Potential short term and long term complications of fetal exposure to hypoglycemia
- Prevention measures to keep parent and baby healthy
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Insulin safe for older adults?
For last week’s practice question, we quizzed test takers on if insulin is safe for older adults. 78% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: For older adults with diabetes using insulin therapy, which of the following is the most accurate statement?
Answer Choices:
- Due to cognitive decline, continuous glucose monitoring is not recommended for older adults.
- Older adults are at greater risk of hypoglycemia than younger adults.
- Divide basal insulin into two separate doses to enhance absorption.
- Give insulin after meals to prevent hypoglycemia.
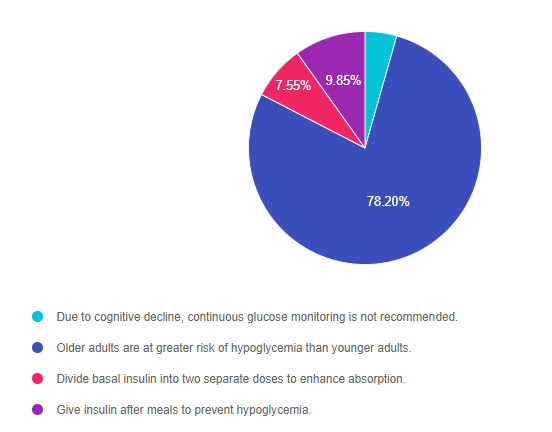
As shown above, the most common choice was option 2, the second most common answer was option 4, then option 3, and finally 1.
Getting to the Best Answer
Answer 1 is incorrect. 4.40% chose this answer, “Due to cognitive decline, continuous glucose monitoring is not recommended for older adults.” Many older adults on intensive insulin therapy with a history of hypoglycemia can benefit from CGM technology to prevent low blood sugars and fine tune carb intake and insulin dosing. Each older adult needs a individualized assessment to determine if a CGM is right for them. The rate of cognitive decline is complex and is a result of genetics, other chronic conditions and overall health combined with aging.
Answer 2 is correct. 78.20% of you chose this answer, “Older adults are at greater risk of hypoglycemia than younger adults. GREAT JOB, almost 80% of you chose this best answer. As people with diabetes age, they are at higher risk for low blood sugars for many reasons, especially if they are taking insulin or a secretagogue. Older individuals may have diminished renal function, which increases the duration of the action of insulin and secretagogues. Some can experience lower calorie intake due to decreasing appetite, trouble chewing, lack of resources, forgetfulness or depression and feelings of isolation. Others may have difficulty administering their insulin or medications accurately or may forget to eat after injections. For this reason, the ADA Standards recommends that older adults are assessed for hypoglycemia risk at each visit coupled with problem solving as needed.
Answer 3 is incorrect. 7.55% of respondents chose this answer, “Divide basal insulin into two separate doses to enhance absorption.” This is a juicy answer. For older adults at risk for hypoglycemia, the ADA does recommend scheduling the basal insulin for the morning instead of evening.
Finally, Answer 4 is incorrect. 9.85% chose this answer, “Give insulin after meals to prevent hypoglycemia.” Another juicy answer. This answer implies that all older people should take their insulin after meals. Some individuals might benefit from post-meal insulin, especially if they are not sure how much they are going to eat and they have a history of hypoglycemia. However, insulin works best when given before the meal so it peaks at the same time the post meal glucose is peaking.
Studying for the CDCES Exam?
Enroll in CDCES Online Prep Bundle + 5th Ed ADCES Review Guide Book | 47 CEs
This bundle includes our CDCES Online Prep Bundle plus the ADCES Review Guide.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
What is a Certified Diabetes Care and Education Specialist?
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM 
Why become a CDCES?
Three Reasons from Coach Beverly
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Diabetes and Earth Health interconnected?
For last week’s practice question, we quizzed test takers on how diabetes and earth health are interconnected. 78% of respondents chose the best answer, GREAT JOB. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues. We can all take action to protect the earth and prepare for extreme climate events.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: According to a NIH systematic literature review, there is clear evidence that diabetes and climate change are interconnected. Which of the following situations are due to the impact of a changing climate?
Answer Choices:
- Lack of healthy food supply due to disrupted agricultural production.
- Shortages of medications, insulin and other diabetes supplies.
- Increased risk of cardiovascular events and death in people with diabetes due to extreme heat.
- All of the above
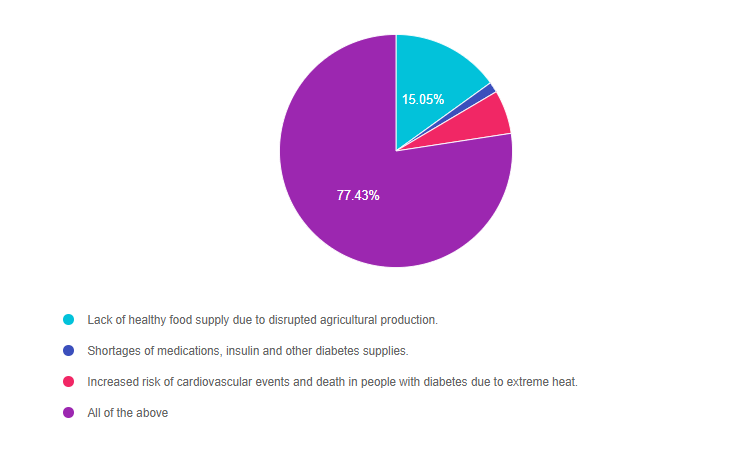
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 3, and finally 2.
Getting to the Best Answer
Answer one – 15.05% chose this answer, and it is accurate “Lack of healthy food supply due to disrupted agricultural production.” It is true that extreme weather can result in agricultural production disruptions. In our community, many fields that were once green with trees and crops, now are brown and barren. There is not enough water to keep crops alive and growing. When the healthy food supply is limited, people living with diabetes may turn to lower-cost, processed foods which are environmentally unfriendly and low in nutrients.
Answer two – 1.46% of you chose this answer and it is accurate, “Shortages of medications, insulin, and other diabetes supplies.” It is true that with recent climate disasters, like the Camp Fire, Hurricane Katrina in 2005, and Hurricane Harvey in 2017, resulted in people not being able to access, afford or safely store their medications, including insulin. In addition, we are experiencing supply chain disruptions in D50 (25 grams of glucose in a 50 ml prefilled syringe (50% glucose)) to treat hypoglycemia and certain intravenous fluids are in short supply. Other diabetes products and medications could be impacted in the future.
Answer three – 6.07% of respondents chose this answer and it is accurate, “Increased risk of cardiovascular events and death in people with diabetes due to extreme heat.” It is true that people with diabetes are at greater risk of experiencing dehydration and cardiovascular events during periods of extreme heat. With the increasing frequency of extreme heat episodes, there is an associated increased risk of heat-related death and cardiovascular events for people living with diabetes. Several studies reveal that people with diabetes have a higher risk of death on hot days, and are more likely to need emergency care and those with a history of heart disease are most vulnerable.
Finally, Answer four – 77.43% chose this answer, “All of the above.” YES. Great job, all of the answers are true, there is clear evidence that diabetes and climate changes are interconnected. As Diabetes Specialists, I believe we can make a difference by leaning into our unique blend of behavior change skills, advocacy, and scientific knowledge.
We can take a two-fold approach:
- Take action to help slow and reverse climate change – Read our blog on actions we can start taking today.
- Help people with diabetes to be prepared for natural disasters. Read our blog on How to Get Ready
Studying for the CDCES Exam?
Enroll in CDCES Online Prep Bundle + 5th Ed ADCES Review Guide Book | 47 CEs
This bundle includes our CDCES Online Prep Bundle plus the ADCES Review Guide.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
What is a Certified Diabetes Care and Education Specialist?
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Why become a CDCES?
Three Reasons from Coach Beverly
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Rationale of the Week | Type 1 or Type 2 Diabetes?
For last week’s practice question, we quizzed test takers on which labs to order for JR. 57% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR’s mom has type 1 diabetes and JR’s dad has type 2 diabetes. JR is 21 years old and in the emergency room with a glucose of 482 mg/dl. Besides checking glucose, ketones and A1C levels, which of the following lab test can be used to determine if someone has autoimmune diabetes?
Answer Choices:
- Endogenous insulin titer
- Glutamic acid decarboxylase
- Beta cells autoantibodies
- Langerhan’s antibody titer
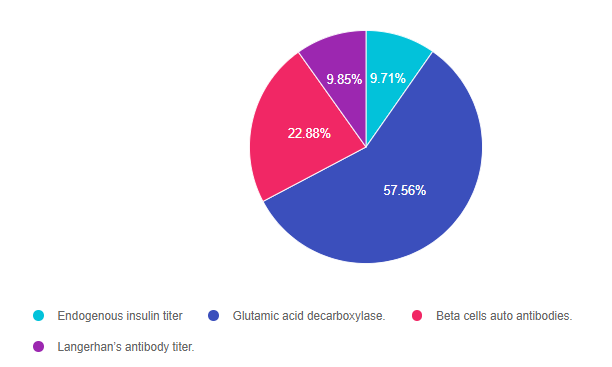
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally 1.
Getting to the Best Answer
Answer 1 is incorrect. 9.71% chose this answer, “Endogenous insulin titer.” This is a juicy answer. Evaluating endogenous insulin production is helpful since it reflects how much insulin the pancreas is secreting. However, it does not reveal if the beta cell loss is due to an immune-mediated response.
Answer 2 is correct. 57.56% of you chose this answer, “Glutamic acid decarboxylase (GAD)”, YES, this is the best answer. If the autoimmune blood test GAD comes back positive, it verifies that the pancreas is being destroyed through an immune-mediated attack of the beta cells. Autoantibodies against GAD are found in 80% of people with type 1 diabetes at clinical presentation.
Answer 3 is incorrect. 22.88% of respondents chose this answer, “Beta cells autoantibodies.” Another juicy answer that is very tempting. However, there is no blood test with this name. The three common antibodies tested are Islet Cell Autoantibodies (ICA), Insulin Autoantibodies (IAA), and Glutamic Acid Decarboxylase (GAD).
Finally, Answer 4 is incorrect. 9.85% chose this answer, “Langerhan’s antibody titer.” Another juicy answer that is very tempting. However, there is no blood test with this name. The three common antibodies tested are Islet Cell Autoantibodies (ICA), Insulin Autoantibodies (IAA), and Glutamic Acid Decarboxylase (GAD).
Studying for the CDCES Exam?
Enroll in CDCES Online Prep Bundle + 5th Ed ADCES Review Guide Book | 47 CEs
This bundle includes our CDCES Online Prep Bundle plus the ADCES Review Guide.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
What is a Certified Diabetes Care and Education Specialist?
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Why become a CDCES?
Three Reasons from Coach Beverly
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.