
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on best approach to treat hypoglycemia according to 2024 ADA Standards. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: The 2024 ADA Standards of Care includes expanded content on the prevention and treatment of hypoglycemia.
Based on the updated guidelines for the treatment of hypoglycemia, which of the following is true?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
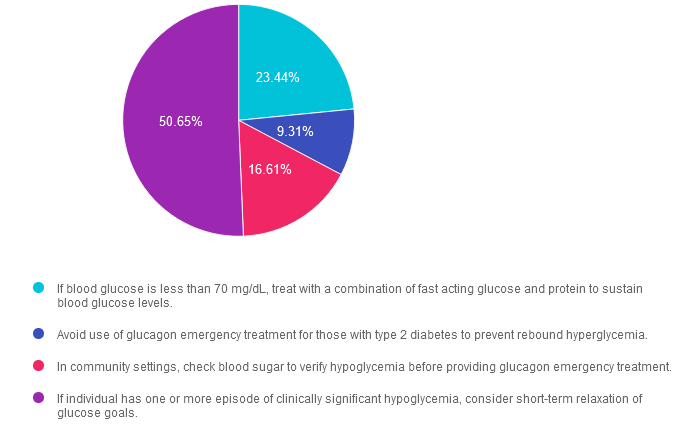
Answer 1 is incorrect. 23.44% chose this answer. “If blood glucose is less than 70 mg/dL, treat with a combination of fast acting glucose and protein to sustain blood glucose levels.” Part of this answer is correct. We need to treat a blood glucose of less than 70 with mg/dL with 15gms of carbohydrate. However, there is no recommendation to add protein to the carbohydrate treatment. As a matter of fact, adding protein (which if often combined with fat) can slow the absorption of the carbohydrate and delay glucose improvement. In addition, for people with beta cell function, the ingestion of protein can stimulate insulin production.
Answer 2 is incorrect. 9.31% of you chose this answer. “Avoid use of glucagon emergency treatment for those with type 2 diabetes to prevent rebound hyperglycemia.” The new standards recommend that all people using insulin therapy have access and training on glucagon rescue medications. See our Glucagon Pocketcards.
Answer 3 is incorrect. 16.61% of respondents chose this. “In community settings, check blood sugar to verify hypoglycemia before providing glucagon emergency treatment.” In the community or home setting, there may be limited access to glucose monitors and the public may not know how to check blood sugars, which could lead to delayed treatment for this emergency situation. For this reason, if a person has diabetes and is experiencing an episode of severe hypoglycemia, it is recommended to provide a glucagon rescue medication and activate the emergency response system if warranted. See our Glucagon Pocketcards.
Finally, Answer 4 is correct. 50.65% chose this answer. “If individual has one or more episode of clinically significant hypoglycemia, consider short-term relaxation of glucose goals.” YES, this is the BEST answer. If a person has an episode of clinically significant hypoglycemia, it is an indication that they may be taking too much insulin or diabetes medication. In addition, experiencing hypoglycemia puts individuals at a higher risk for another episode of significant hypoglycemia. Relaxing glucose goals and up-adjusting them can help the person re-set their “glucose thermostat” in a safer range with the ultimate goal of preventing future hypoglycemia.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on 2024 ADA Standards. 44% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
The new ADA 2024 Standards of Care include dozens of updates to diabetes clinical practice.
Which of the following statements has actually been added to the ADA 2024 Standards of Care?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
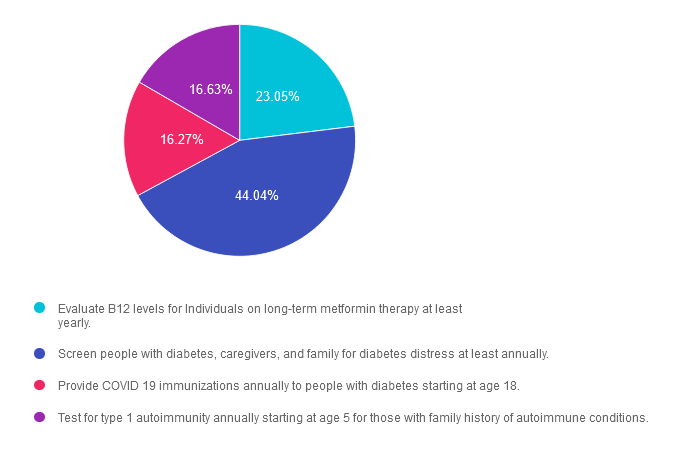
Answer 1 is incorrect. 23.05% chose this answer. “Evaluate B12 levels for Individuals on long-term metformin therapy at least yearly.” This juicy answer is very tempting. It is true the metformin can be associated with lower B12 levels. However, the ADA does not recommend checking B12 levels annually for people taking this biguanide. Instead, they suggest regularly monitoring B12 levels in people on metformin therapy who have signs of B12 deficiency such as neuropathy or anemia.
Answer 2 is correct. 44.04% of you chose this answer. “Screen people with diabetes, caregivers, and family for diabetes distress at least annually.” Yes, this is the BEST answer! Many individuals with diabetes experience unrecognized and undertreated diabetes distress, which can lead to decreased engagement in self-management activities and worsen outcomes. We address diabetes distress and discuss strategies to address this common emotional response to diabetes in our ReVive 5 Training Program.
Answer 3 is incorrect. About 16.27% of respondents chose this. “Provide COVID 19 immunizations annually to people with diabetes starting at age 18.” The ADA recommends starting COVID 19 immunizations in people with diabetes starting at 6 months and follow-up with boosters as recommended,
Finally, Answer 4 is incorrect. 16.63% chose this answer. “Test for type 1 autoimmunity annually starting at age 5 for those with family history of autoimmune conditions.” Autoimmune testing is recommended for those with immediate family members with type 1 diabetes and other risk factors. There is no age cut-off nor is there a recommendation for annual testing.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Objectives:
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other healthcare providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on the new ADA Standards for type 2 diabetes medication. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Based on the newly released 2024 American Diabetes Association (ADA) Standards of Care, which of the following statements is NOT accurate regarding treatment for hyperglycemia?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
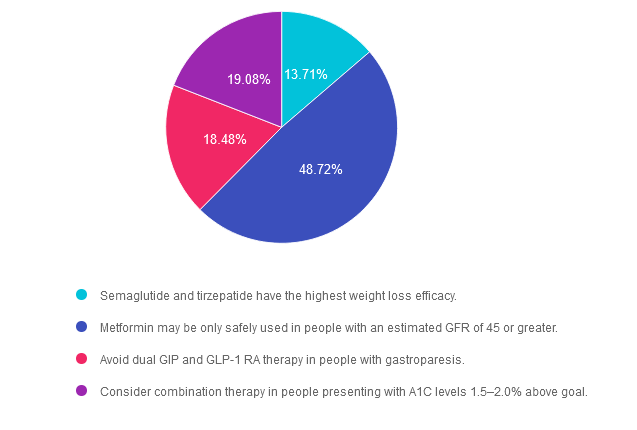
Answer 1 is incorrect. 13.71% chose this answer. “Semaglutide and tirzepatide have the highest weight loss efficacy.” This statement is accurate. These two incretin mimetics not only substantially lower A1C levels, they also are associated with the highest percentage of weight loss of all the diabetes medications. See Diabetes Med PocketCards for more information.
Answer 2 is correct. 48.72% of you chose this answer. “Metformin may be only safely used in people with an estimated GFR of 45 or greater.” YES, great job! This answer is FALSE (making it the best answer). If a person with diabetes is taking metformin and their GFR drops below 30, then we stop the medication. However, we can start or continue metformin therapy if the GFR is 45 or greater. In addition, metformin doesn’t harm the kidneys, it actually protects them by lowering blood glucose levels. See Diabetes Med PocketCards for more information.
Answer 3 is incorrect. About 18.48% of respondents chose this. “Avoid dual GIP and GLP-1 RA therapy in people with gastroparesis.” This answer is also accurate. Tirzepatide (Mounjaro) can substantially slow gastric emptying which could exacerbate gastroparesis. For that reason, it is not a recommended therapy for people with gastroparesis.
Finally, Answer 4 is incorrect. 19.08% chose this answer. “Consider combination therapy in people presenting with A1C levels 1.5–2.0% above goal.” This answer is also accurate. The ADA Standards of Care recommend more intensive pharmacologic intervention for those with substantially elevated A1C to improve and prolong pancreatic function.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Topics:
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on what is the best approach for people with low literacy skills. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Which of the following strategies is most effective when working with someone with low literacy skills?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
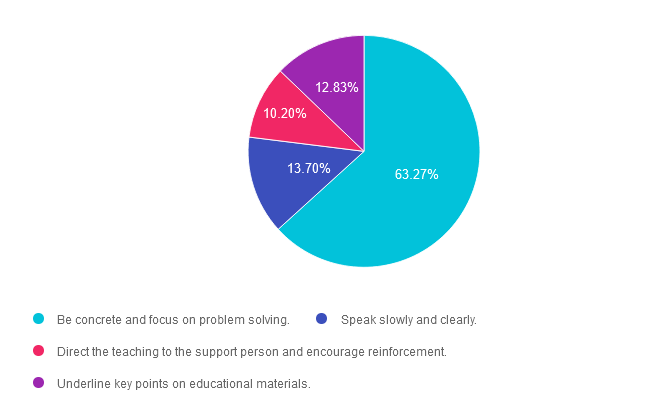
Answer 1 is correct. 63.27% chose this answer. “Be concrete and focus on problem solving.” Yes, this is the best answer. Since a person with low literacy can’t take notes or read information later, they will need to commit new information to memory. By providing concrete examples and engaging in collaborative problem solving, a person with low literacy can more effectively retain the information.
Answer 2 is incorrect. 13.70% of you chose this answer. “Speak slowly and clearly.” Just because a person hast low literacy doesn’t mean they have an intellectual disability. Maybe they didn’t have a chance to complete their education or experienced some other impediment to learning how to read and write. We can use a usual conversational pace and annunciation with this individual.
Answer 3 is incorrect. About 10.20% of respondents chose this. “Direct the teaching to the support person and encourage reinforcement.” A general rule of effective communication is to direct the teaching and education to the person with diabetes, while including the support person.
Finally, Answer 4 is incorrect. 12.83% chose this answer. “Underline key points on educational materials.” Since people with low literacy have limited ability to read and write, using print materials with words would not be an effective method to provide education. Use of pictures and infographics, videos, podcasts or other educational strategies that don’t require literacy, would be excellent alternatives.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Topics:
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on what is the difference between a CDCES & BC-ADM. 57% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
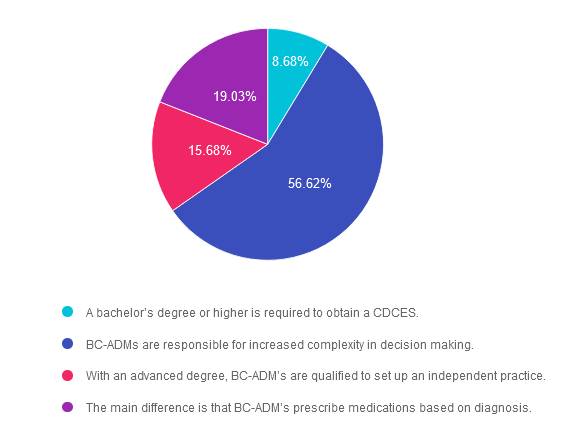
Answer 1 is incorrect. 8.68% chose this answer.” A bachelor’s degree or higher is required to obtain a CDCES.”
Eligibility to take the exam is based on licensure, registration, or certification. According to the CDCES website, the following health care professionals meet the discipline requirement.
Answer 2 is correct. 56.62% of you chose this answer.” BC-ADMs are responsible for increased complexity in decision making.”
Answer 3 is incorrect. About 15.68% of respondents chose this. “With an advanced degree, BC-ADM’s are qualified to set up an independent practice.”
This is a juicy answer but is not correct. Let’s say I want to set up shop as a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. Even with my BC-ADM, I couldn’t bill for services, and under whose oversight would I see people with diabetes and make treatment recommendations?
Again, it’s not the BC-ADM that creates the opportunity to set up an independent practice. As a licensed RN, I can’t set up an independent practice and bill for my services in my state. Certification does not change your scope of practice and can come from different organizations. Each state’s licensure and scope of practice regulations come from a governmental authority. We must practice within the legal parameters of our scope of practice based on licensure.
Finally, Answer 4 is incorrect. 19.03% chose this answer. “The main difference is that BC-ADM’s prescribe medications based on diagnosis.”
The BC-ADM is a certification exam and it does not confer prescriptive authority. Only those with certain licenses can prescribe medications, and the regulations can vary from state to state. For example, I am a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. As a licensed RN, I do not have prescriptive authority. Certification does not change your scope of practice and can come from different organizations. Licensure comes from governmental authority.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Topics:
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Topics:
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on how to best detect euglycemic ketosis. 53% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
According to recent research by the ADA/EASD, about 10% of people admitted to the hospital in diabetes crisis have euglycemic diabetes ketoacidosis.
Since blood sugars are at normal levels or only slightly elevated, which of the following lab tests most accurately evaluate for euglycemic ketosis?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
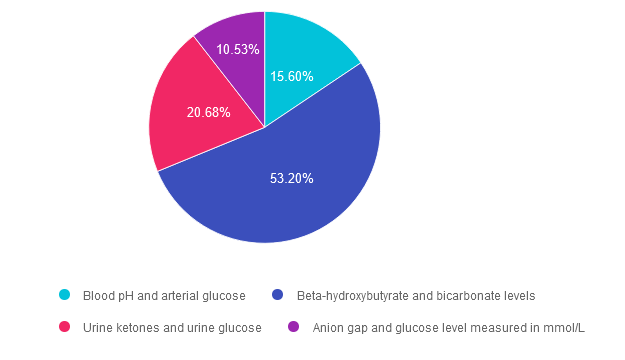
Answer 1 is incorrect. 15.60% chose this answer. “Blood pH and arterial glucose.” Since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL, checking arterial glucose levels won’t provide additional clarity on diagnosis. However, checking pH levels is recommended, since a pH less than 7.3 is a clear clinical indication of ketosis.
Answer 2 is correct. 53.20% of you chose this answer. “Beta-hydroxybutyrate and bicarbonate levels.” YES, this is the best answer. Beta-hydroxybutyrate evaluation with a low cutoff equal to or greater than 3.0 mmol/L, whether by lab or point-of-care-testing, is one of the most accurate measurements to evaluate if a person is in ketosis. Bicarbonate level concentration < 18 mmol/L also helps to provide confirmation of ketosis. Ketoacidosis in diabetes is due to inadequate circulating insulin, so the body switches to burning fat for fuel (instead of glucose), which leads to a build up of ketones or ketosis.
Answer 3 is incorrect. About 20.68% of respondents chose this. “Urine ketones and urine glucose.” Urine ketone testing can be used if Beta-hydroxybutyrate evaluation is not available. A urine ketone strip value of 2+ or greater indicates ketosis. However, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
Finally, Answer 4 is incorrect. 10.53% chose this answer. “Anion gap and glucose level measured in mmol/L.” he anion gap has long been a clinical measure of acidosis; however it is not considered to be a key indicator in the new guidelines. Metabolic acidosis is now defined as a pH < 7.3 and a bicarbonate concentration < 18 mmol/L. The anion gap can still be used in settings where ketone testing is unavailable. In addition, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on how much does Diabetes Cost the U.S? 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: According to the recently published ADA report on the 2022 Economic Costs of Diabetes in the U.S., which of the following statements is most accurate?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
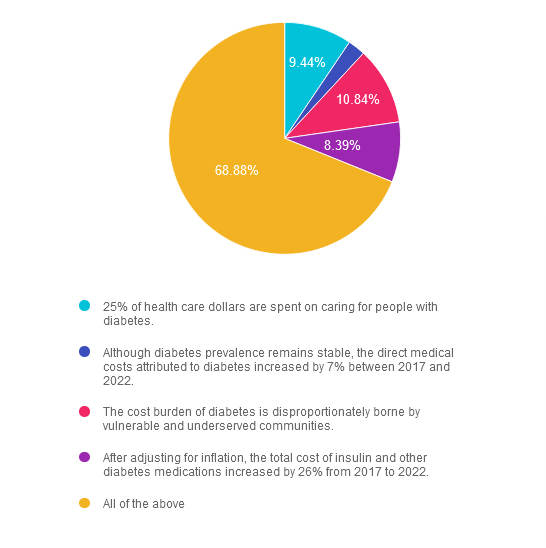
Answer 1 is incorrect. 9.44% chose this answer. “25% of health care dollars are spent on caring for people with diabetes.” Yes, a quarter of all health care dollars are spent on diabetes, with the majority of money spent on hospitalizations due to cardiovascular complications and medications. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 2 is incorrect. 2.45% of you chose this answer. “Although diabetes prevalence remains stable, the direct medical costs attributed to diabetes increased by 7% between 2017 and 2022.” The cost of treating diabetes keeps increasing, putting additional financial strain on people living with diabetes. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 3 is incorrect. About 10.84% of respondents chose this. “The cost burden of diabetes is disproportionately borne by vulnerable and underserved communities.” People who earn the least amount of money and live in under-resourced areas, continue to have the highest rates of diabetes and other chronic health conditions. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 4 is incorrect. About 8.39% of respondents chose this. “After adjusting for inflation, the total cost of insulin and other diabetes medications increased by 26% from 2017 to 2022.” Yes, the cost of medications keeps increasing, which may prevent many people from accessing optimal diabetes treatment. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022
Finally, Answer 5 is correct. 68.88% chose this answer. “All of the above” YES, GREAT JOB. Most of you chose the BEST Answer. Thank you for participating in our Question of the Week. All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
Topics:
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on why we celebrate World Diabetes Day on Nov 14th. 39% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: In 1923, the Nobel prize in Physiology or Medicine was awarded to Frederick Grant Banting and John James Richard MacLeod “for the discovery of insulin”. 100 years later, we celebrate this life-saving discovery each year on November 14th, a day designated as World Diabetes Day.
Why do we celebrate World Diabetes Day on November 14th? Please choose the best answer.
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, and choose the BEST answer.
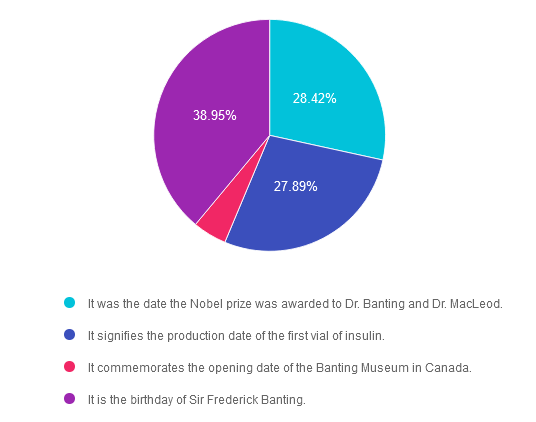
Answer 1 is incorrect. 28.42% chose this answer. “It was the date the Nobel Prize was awarded to Dr. Banting and Dr. MacLeod.” This is not the reason, however it is interesting to note that the Nobel prize for the discovery of insulin was awarded on December 10, 1923 in Stockholm, Sweden.
Answer 2 is incorrect. 27.89% of you chose this answer. “It signifies the production date of the first vial of insulin.” Great guess. However, it wasn’t until 1923 that the first vials of insulin were commercially produced and distributed.
Answer 3 is incorrect. About 4.74% of respondents chose this. “It commemorates the opening date of the Banting Museum in Canada.” The Banting House is a former residence and current museum in London, Ontario, Canada, known as the “Birthplace of Insulin.” It is the house where Sir Frederick Banting woke up at two o’clock in the morning on October 31, 1920 with the idea that led to the discovery of insulin. Since 1984, the house has been a museum dedicated to Banting’s discovery and his life.
Finally, Answer 4 is correct. 38.95% chose this answer. “It is the birthday of Sir Frederick Banting.” YES, this is the best answer. Dr. Banting was born on November 14, 1891. That is why we celebrate World Diabetes Day on November 14th.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
.png?h=459&iar=0&w=1459&hash=E665292742D2BABAECCFA59A56B88D3C)
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.