
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on diabetes & the impact it has on communities. 82% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: November is National Diabetes Month. This month shines a spotlight on the 37 million people living with diabetes and the 96 million with prediabetes. Certain communities are hit harder with diabetes than others due to a combination of genetics and social determinants of health.
Which of the following statements are most accurate?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
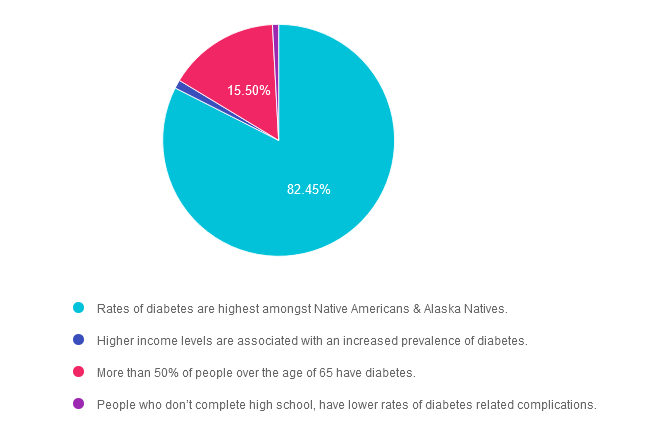
Answer 1 is correct. 82.45% chose this answer. “Rates of diabetes are highest amongst Native Americans & Alaska Natives.” YES, sadly, this is the best answer. For both men and women, prevalence of diagnosed diabetes was highest among American Indian and Alaska Native adults (13.6%), followed by non-Hispanic Black adults (12.1%), adults of Hispanic origin (11.7%), non-Hispanic Asian adults (9.1%) and non-Hispanic White adults (6.9%) (See CDC Appendix Table 3). As diabetes advocates, we can campaign for improved access to health care and address social determinants of health for communities at highest risk of prediabetes and diabetes.
Answer 2 is incorrect. 1.19% of you chose this answer. “Higher income levels are associated with an increased prevalence of diabetes.” People who have the lowest earnings and who don’t graduate high school have the highest rates of diabetes. Socioeconomic status and rates of diabetes are inversely related.
Answer 3 is incorrect. About 15.5% of respondents chose this. “More than 50% of people over the age of 65 have diabetes.” This is a tempting answer, but a little exaggerated. According to CDC Stats, 30% of people age 65 or live with diabetes.
Finally, Answer 4 is incorrect. 0.85% chose this answer. “People who don’t complete high school, have lower rates of diabetes related complications.” People who don’t graduate high school have the highest rates of diabetes and less resources to engage in preventive care.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
.png?h=459&iar=0&w=1459&hash=E665292742D2BABAECCFA59A56B88D3C)
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on the 5 different tongue tastes. 67% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR thinks that their ability to taste food has diminished recently. They ask you, what are the five confirmed basic tastes of the tongue?
Which of the following lists describes the best answer?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
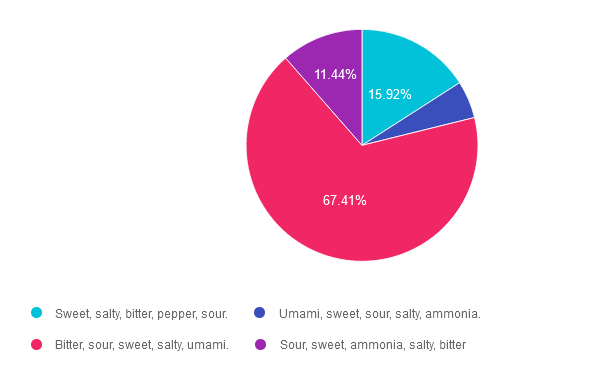
Answer 1 is incorrect. 15.92% chose this answer. “Sweet, salty, bitter, pepper, sour.” This answer is really close, however there are no specific receptors on the tongue to detect the flavor pepper.
Answer 2 is incorrect. 5.22% of you chose this answer. “Umami, sweet, sour, salty, ammonia.” This answer is really close, however, ammonia is not a confirmed flavor and this list is missing the flavor, bitter.
Answer 3 is correct. About 67.41% of respondents chose this. “Bitter, sour, sweet, salty, umami.” YES, these are the 5 confirmed tastes and one more taste might be added to list, ammonium chloride. According to an article in Neuroscience News, “The tongue’s response to ammonium chloride, a component in some candies, may indicate a sixth basic taste. The study illuminated that OTOP1, a protein receptor that signals sour taste, also responds notably to ammonium chloride.”
Finally, Answer 4 is incorrect. 11.44% chose this answer. “Sour, sweet, ammonia, salty, bitter” This answer is really close, however, ammonia is not a confirmed flavor and this list is missing the flavor, umami.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on checking for fibrosis & liver elastography. 52% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: The provider is sending JR for a Liver Elastography or FibroScan test since JR has elevated ALT and AST levels along with an elevated Fib-4 score.
Which of the following are measured during this liver ultrasound procedure?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
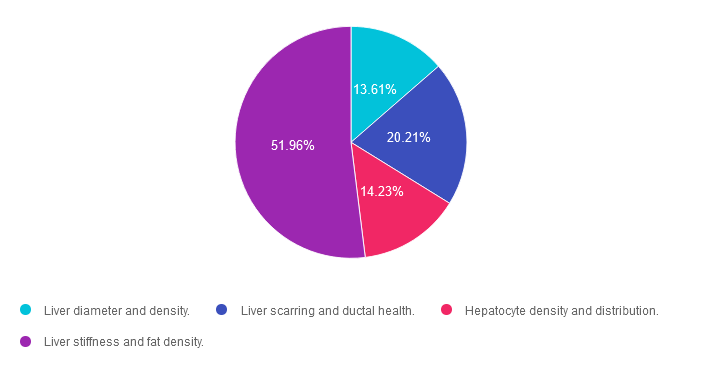
Answer 1 is incorrect. 13.61% chose this answer. “Liver diameter and density.” This answer is tempting, but unfortunately, it is not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Answer 2 is incorrect. 20.21% of you chose this answer. “Liver scarring and ductal health.” This answer is also tempting, but not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Answer 3 is incorrect. About 14.23% of respondents chose this. “Hepatocyte density and distribution.” Unfortunately, this tempting answer is not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Finally, Answer 4 is correct. 51.96% chose this answer. “Liver stiffness and fat density.” YES, this is the BEST Answer. This 5-10 minute, non-invasive test, measures liver stiffness or degree of fibrosis (reported as the kPa score) and the amount of fat in the liver (reported as the CAP score). Join our FREE Webinar on Exploring the GI System – From the Gut to the Butt on November 16th to learn more!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on how glucose levels impact gastric emptying. 46% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
Glucose fluctuations can impact gastric emptying rates.
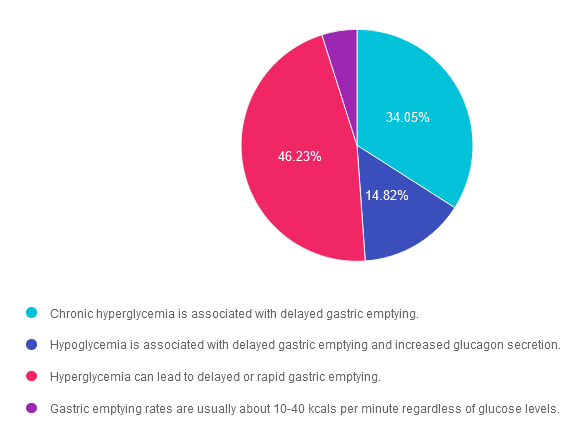
Which of the following is the MOST accurate statement that describes the impact of glucose levels on gastric emptying rates?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 34.05% chose this answer. “Chronic hyperglycemia is associated with delayed gastric emptying.” This tempting answer implies that chronic hyperglycemia only causes delayed gastric emptying. However, more recent data suggests that acute and chronic hyperglycemia can also cause faster gastric emptying, resulting in post meal hyperglycemia and increased hunger.
Answer 2 is incorrect. 14.82% of you chose this answer. “Hypoglycemia is associated with delayed gastric emptying and increased glucagon secretion.” This answer has elements of accuracy. If someone injects bolus insulin before eating a meal, and they have gastroparesis, this can result in post meal hypoglycemia due to a mismatch of insulin action and carbohydrate absorption. The second part of the answer is inaccurate, since increased glucagon secretion is associated with hyperglycemia.
Answer 3 is correct. About 46.23% of respondents chose this. “Hyperglycemia can lead to delayed or rapid gastric emptying.” YES, great job. Acute and chronic hyperglycemia can wreak havoc on stomach emptying, causing either delayed or expediated bolus propulsion to the duodenum.
Finally, Answer 4 is incorrect. 4.9% chose this answer. “Gastric emptying rates are usually about 10-40 kcals per minute regardless of glucose levels.” This answer sounds accurate, but gastric emptying rates are approximately 1-4 Kcals per minute.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
A helpful research article recommended by Coach Beverly that expounds upon this topic:
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on treating H. pylori. 78.42% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 50, has type two diabetes, and was referred to G.I. due to six months of stomach pain, intestinal, bloating, and generalized G.I. discomfort. Since they were due for their colonoscopy, the doctor also ordered an upper endoscopy to biopsy the esophagus, stomach and duodenum for any abnormalities.
The biopsy revealed that JR had moderate chronic gastritis and an H. pylori infection. JR wants to learn more about H. pylori infection.
Which of the following statements are accurate?
Answer Choices:

If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 5.27% chose this answer. “Since H. pylori is found in about half the population, it is a normal finding, and there is no need for treatment.” It is true that 50% of people worldwide house H. plyori in their stomach. However, in a small percentage of human hosts, this little bacteria “goes rogue” and causes gastritis, loss of stomach mucous lining, peptic ulcers and can be associated with some stomach cancers.
Answer 2 is correct. 78.42% of you chose this answer. “Treatment includes double antibiotic therapy and a medication to decrease gastric acidity.” YES, GREAT JOB. According to the Cleveland Clinic, 2 antibiotics and a proton pump inhibitor are prescribed to address H. pylori infections.
Antibiotics: Among the common choices are amoxicillin, clarithromycin (Biaxin®), metronidazole (Flagyl®) and tetracycline.
Proton pump inhibitor: Commonly used proton pump inhibitors include lansoprazole (Prevacid®), omeprazole (Prilosec®), pantoprazole (Protonix®), rabeprazole (Aciphex®) or esomeprazole (Nexium®).
Answer 3 is incorrect. About 13.84% of respondents chose this. “The preferred treatment is the consumption of prebiotics and probiotics to increase bacterial diversity.” Consuming prebiotics and probiotics are a recommended adjunctive therapy to antibiotics and a proton pump inhibitor. However, current evidence does not support pre and probiotics as the only treatment.
Finally, Answer 4 is incorrect. 2.47% chose this answer.” Most people with H. pylori infection experience stomach cancer within the next 20 years.” There is a slightly increased risk (~5%) of stomach cancer for those with H. plyori infection, especially if the H. pylori isn’t treated or if there is a family history of stomach cancer. This answer is suspicious because of the extreme statement that “Most” people get cancer from this bacteria gone rogue.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information

ADCES Hawaii Chapter & Coach Bev invite you to join this class that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Location: Honolulu Country Club, 1689 Ala Pu’umalu Street, Honolulu, HI
CEs: 6.5 CEs for physicians, nurses, pharmacists, physician assistants, dieticians & social workers.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on reviewing insulin dosing adjustments. 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR lives with type 1 diabetes and severe gastroparesis, despite maintaining an A1C of less than 7% for the past few years. The endocrinologist referred JR to a GI specialist, who recommended a surgical procedure called a Gastric Peroral Endoscopic Myotomy, G-POEM, to address JR’s longstanding gastroparesis.
JR asks what you think about this intervention. What is the best response?
Answer Choices:

If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 28.90% chose this answer. “It sounds like you are worried about the effectiveness and risks of this procedure. Is that right?” This tempting answer is not the best answer since JR never states that they are worried about the effectiveness of the G-POEM. Instead they just want to see what the Diabetes Care and Education Specialist thinks about this procedure. When in doubt, re-examine the key intent of the question.
Answer 2 is correct. 69.27% of you chose this answer. “Tell me more about what your GI doctor told you about this procedure.” YES, this is the BEST answer. Great job. By asking what JR knows about the procedure, we provide JR an opportunity to share their knowledge and assess areas of concern. In addition, we may let JR know that we haven’t heard of this procedure, but we will look into it.
Answer 3 is incorrect. About 0.92% of respondents chose this. “I know you are frustrated, but the primary treatment for gastroparesis is low fiber meals.” It is true that we recommend low fiber meals for gastroparesis, but JR was asking about a procedure not meal planning.
Finally, Answer 4 is incorrect. 0.92% chose this answer. “Usually, gastroparesis improves as your A1C reaches target so I would wait and see if things improve.” It is true that the stomach is better at moving its’ content forward when blood sugars are closer to target most of the time. But, sometimes, despite having an A1C on target, severe autonomic neuropathy interferes with stomach propulsion past the pyloric sphincter.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on reviewing insulin dosing adjustments. 67% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: MR is 68 with type 2 diabetes and tells you that their provider increased their NPH insulin to three times a day and told them to adjust the NPH insulin dose based on their pre-meal blood sugar levels.
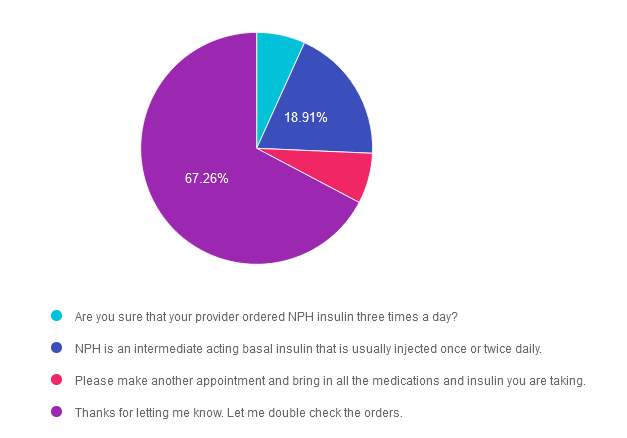
What is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 6.77% chose this answer. “Are you sure that your provider ordered NPH insulin three times a day?” This is not the best response, since it might make the individual feel like they did something wrong and put them in a defensive position.
Answer 2 is incorrect. 18.91% of you chose this answer. “NPH is an intermediate acting basal insulin that is usually injected once or twice daily.” This is a correct factual answer, but it is not the best answer since it summarizes how NPH insulin works, but doesn’t address the root of the issue or assist with problem solving.
Answer 3 is incorrect. About 7.06% of respondents chose this. “Please make another appointment and bring in all the medications and insulin you are taking.” Although “brown bagging” meds is always a good idea, this answer means that MR would continue giving NPH three times a day on a sliding scale until the next appointment is available. This delay of action could result in unstable blood glucose levels.
Finally, Answer 4 is correct. 67.26% chose this answer. “Thanks for letting me know. Let me double check the orders.” This affirmational, person centered answer is the best choice! It acknowledges MR’s concern and is followed by action to help with problem solving. GREAT JOB!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on the importance of annual kidney testing. 52% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Only about 40% of individuals with diabetes get their kidney function tested annually.
Why is the evaluation of glomerular filtration rate (GFR) and Urinary Albumin Creatinine Ratio (UACR) of critical importance for people with diabetes?
Answer Choices:

If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 3.43% chose this answer. “Evaluate if peritoneal or hemodialysis is necessary for the individual.” For people experiencing chronic kidney disease and worsening kidney function, they would need their GFR and UACR checked more frequently than annually along with a referral to a kidney specialist.
Answer 2 is correct. 51.56% of you chose this answer. “Determine best anti-hypertensive and glucose pharmacotherapy.” YES, this is the best answer. Knowing the GFR and UACR is critical to determining best medication therapies. For individuals with diabetes and a GFR less than 60 and/or a UACR of 30mg/g or greater, the ADA Standards recommend starting a SGLT-2 Inhibitor to preserve renal function. In addition, in individuals with hypertension and a UACR of 30mg/g or greater, the antihypertensive of choice is either an ACE or ARB. Yearly kidney function screening helps not only direct best diabetes and hypertensive medication therapy, it also identifies early kidney disease so preventive action can be taken.
Answer 3 is incorrect. About 8.48% of respondents chose this. “Protect against immune mediated renal complications.” This juicy answer is tempting and sounds good, but it is not an accurate response or a recognized condition.
Finally, Answer 4 is incorrect. 36.53% chose this answer. “Slow the progression of chronic kidney disease development.” This answer is tempting, but it does not address the intent of the question. Yearly kidney function testing informs the care providers about the health of the kidney. but simply testing does not slow kidney disease. Action is required.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
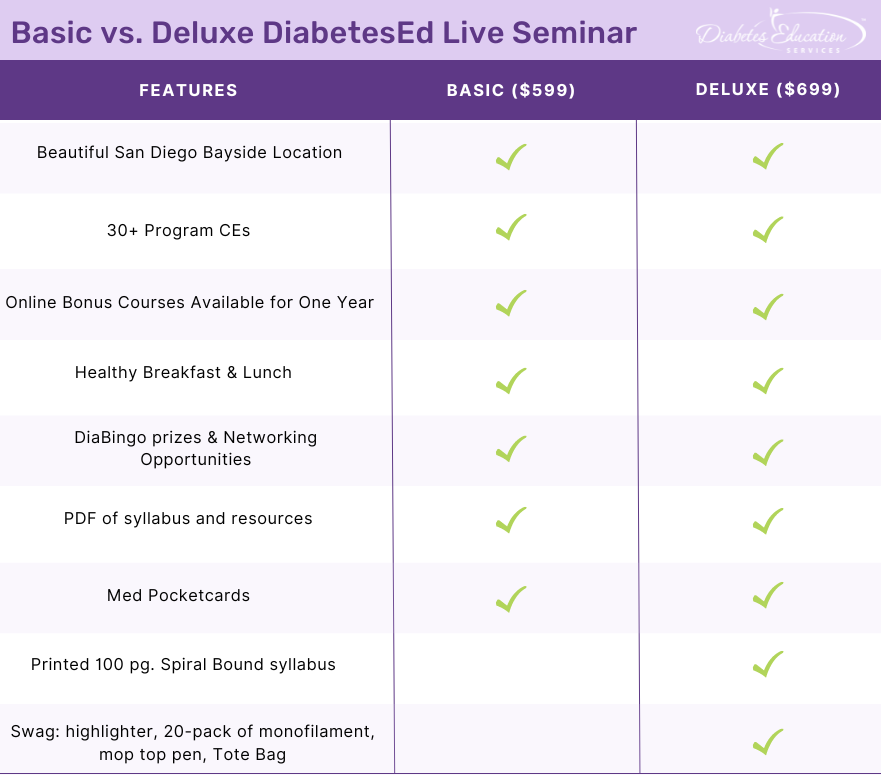
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.